
Abstract
BACKGROUND:
Acoustic Neuroma (AN) is a benign tumour of the eighth cranial nerve. Stereotactic Radiosurgery (SRS) is a common treatment approach. Studies have explored the primary effects of SRS and documented equivalent efficacy for tumour control compared to neurosurgery.
OBJECTIVE:
Examine the longer term cognitive and psychosocial outcomes of SRS in non-Neurofibromatosis Type II patients utilising both objective and subjective cognitive outcomes associated with quality of life and health related distress.
METHODS:
Nineteen individuals treated via SRS were assessed using a battery of standardised psychometric tests as well as measures of quality of life and psychological distress.
RESULTS:
Participants had largely preserved cognitive function except for processing speed, aspects of attention and visual memory relative to age norms. Self-reported quality of life was better than in other AN population studies. Level of psychological distress was equivalent to general population norms. More than half of participants reported subjective cognitive decline though this was not fully supported by objective testing. Subjective cognitive complaints may be associated with lower reported quality of life.
CONCLUSIONS:
Results are largely consistent with previous findings on the effects of SRS in other clinical groups, which supports SRS as a targeted radiation treatment for AN.
Introduction
Acoustic Neuroma (AN), also known as Vestibular Schwannoma, is among the most common type of benign brain tumour, making up approximately 6–10% of all intracranial lesions (Betkas, Zverina & Balogova, 2014). AN typically manifests as unilateral hearing loss, unilateral tinnitus and as the tumour develops in the eighth cranial nerve, approximately 50% of individuals develop reduced balance and dizziness (Broomfield & O’Donoghue, 2016). Facial sensory disturbances is observed where larger tumours exist as they begin to press on the trigeminal nerve, and in fewer cases facial weakness, twitching or paralysis when pressing on the facial nerve. With increasing mass, the tumour can impact upon other brain structures including the brain stem, cerebellum or cause cerebrospinal fluid (CSF) blockage, and in these cases AN can become life-threatening (Bambakidis et al., 2011).
AN is typically managed by observation and monitoring, surgical removal (partial or complete resection) or radiation treatment (Carlson, Tveiten, Driscoll et al., 2015). Stereotactic Radiosurgery (SRS) has become an increasingly utilised treatment for small to medium sized benign tumours including AN, and its efficacy has been well established among individuals up to 10 years post treatment (Carlson et al., 2015; Hasegawa, Kida, Kato et al., 2013). Theoretically, it is a radiation technique which aims to irradiate pathological tissues, while minimising the amount of healthy tissue exposed to radiation (Kondziolka, Shin, Brunswick et al., 2015).
The primary effects of radiation in terms of tumour progression and cranial neuropathy in AN have been well documented (Kondziolka et al., 2015). However, few studies to date have explored the longer term outcomes of SRS on AN and those that have, focus on the primary effects of radiation dose on tumour control, latent cyst formation and hearing and facial function, with relative dearth exploring long-term cognitive sequelae (Dutta, Balaji Subramanian, Murli et al., 2012; Hasegawa, Kida, Kato et al., 2013). To date, those studies which have explored the neuropsychological outcomes following SRS in other clinical conditions such as cerebral arteriovenous malformations (AVM) and recurrent craniopharyngioma have observed disturbance in memory, executive function and processing speed, although the mechanism by which cognitive function is impacted among these populations is not directly comparable to AN (Murray, Dally, Jeffreys et al., 2014).
Previous research has illustrated the relationship between cognitive function and quality of life (QoL) in neuro-oncology. There is now increased recognition of the importance of measuring quality of life alongside other traditional outcome measures of survival, and time from treatment to disease progression (Witgert & Meyers, 2011) A review article (Mitchell, Kemp, Benito-Leon et al., 2010) observed that among those with Mild Cognitive Impairment (MCI), QoL was compromised. QoL is now increasingly viewed as second only to survival when considering outcome following treatment in clinical trials (Dirven, Reijneveld, Aaronson NK et al., 2013; O’Reilly, Murray & Hadley, 2008). Perceived cognitive function has also been related to quality of life among other clinical populations (e.g. oncology, cardiology, bi-polar disorder and Multiple Sclerosis) (Mackala, Torres, Kozicky et al., 2014; Sandau, Lindguist, Treat-Jacobson et al., 2008) and increasingly self-report methods are used in neuropsychological settings as an adjunct to standardised tests, enhancing the ecological validity of assessments (Sbordone, Saul & Purisch, 2007, pp. 142–144). In particular, AN population studies have observed elevated rates of anxiety in those who have undergone radiation (O’Reilly, Murray & Hadley, 2008). While the risk of radiation toxicity is likely to be reduced when SRS is used compared to whole brain radiation therapy (Chang, Wefel, Hess et al., 2009), there is a paucity of studies documenting the longer term cognitive sequelae of SRS in AN patients. In particular, as illustrated in Fig. 1 the inferior temporal lobe inevitably receives some dose due to its proximity to the AN. Accordingly consideration of the potential cognitive consequence of radiation exposure to the temporal lobe as well as surrounding structures is of clinical relevance. This study investigated the extent or otherwise of domain specific cognitive impairments and quality of life following SRS for AN. In addition, participant’s subjective accounts of their cognitive and psychosocial outcomes were also analysed. It was predicted that AN cases will show impairment in cognitive performance relative to the normal population.
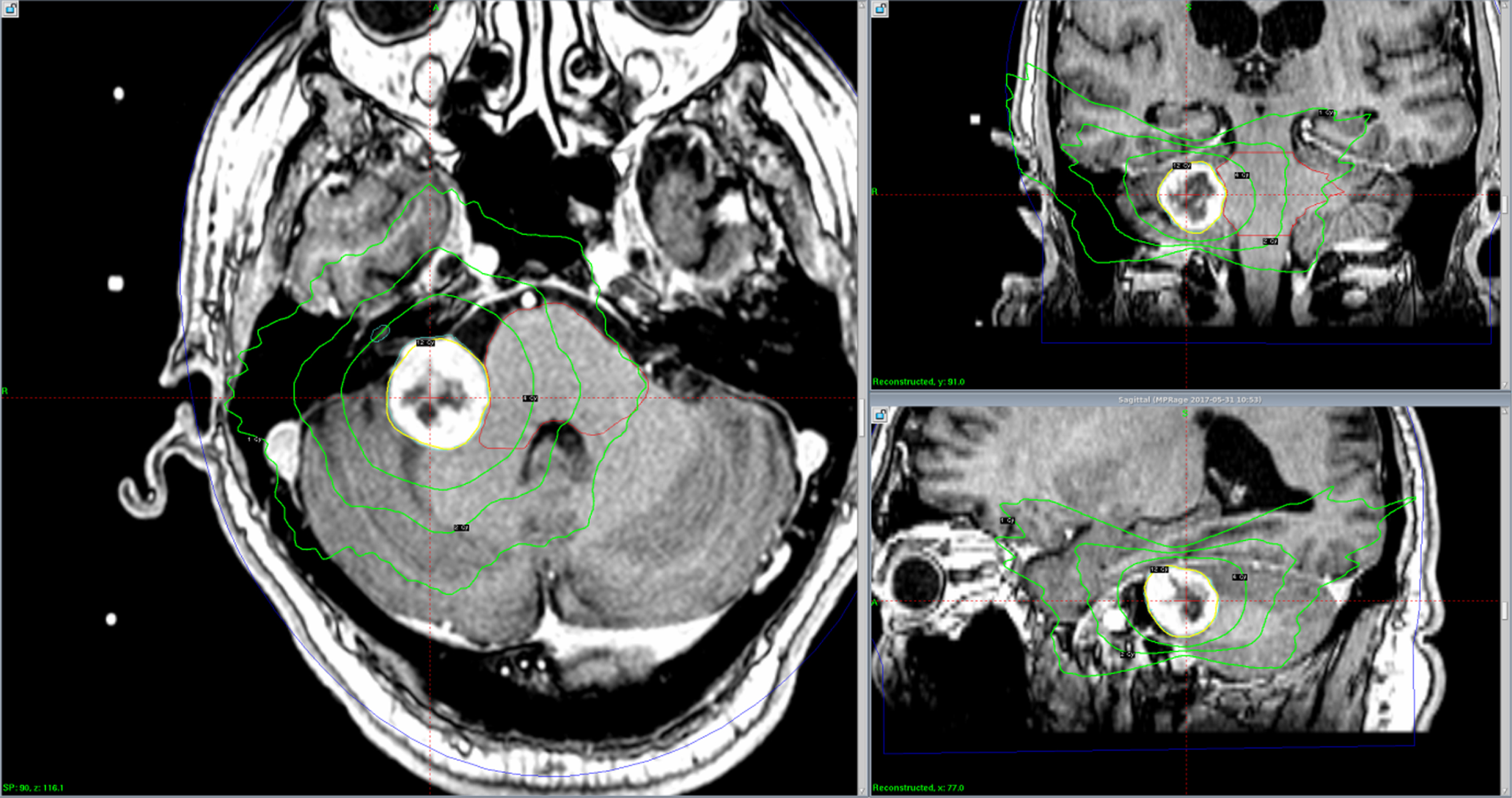
Axial, coronal and sagittal views of an acoustic neuroma Gamma Knife plan showing dose “spillage” into the inferior temporal lobe.
Axial, coronal and sagittal views of an acoustic neuroma Gamma Knife plan showing dose “spillage” into the inferior temporal lobe.
Participants
All patients who had received SRS for AN in a Regional NHS Neurosciences centre serving (circa 1.8 million) over the preceding five years were eligible to participate in the study. No individuals were excluded albeit one person had died since treatment. Of 42 eligible individuals, 19 (45%) agreed to participate (10 males and 9 females (M = 61.9 years; SD = 11.6 years; Range = 47–80). Subsequent chart review of participants completed by the treating clinician documented demographic as well as treatment specific information such as age, gender, time since diagnosis and treatment, tumour size, tumour site and radiation dose to brain tissue. Test of Pre-morbid Functioning (TOPF: Wechsler, 2011) scores observed estimated mean premorbid cognitive ability within the ‘Average’ range (M = 101.1; SD = 12.0) with no effect size observed relative to normative data (d = 0.08). Mean length of time from diagnosis to treatment was 29.7 (SD = 26.1) months and mean length of time from treatment to study participation was 33.4 months (SD = 16.9; range = 14–78 months). Among participants, no reported history of alcohol or drug abuse, no diagnosed Intellectual Disability (ID) nor known progressive neurological condition was documented. All individuals received the same dose to the tumour margin (12 Gy) with the 50% isodose line applied to the tumour margin in 94% of participants. Mean target volume among the sample was 3.05 cm3 (SD = 4.3; range 0.73 cm3 –6.98 cm3). Whilst no clinical details were available on non-respondents, participants were comparable to AN prevalence data for gender but not for age. The present sample is older relative to prevalence data on age (M = 45.0; SD = 21.2) (Berkowitz, Iyer, Kano et al., 2015).
Materials
A battery of standardised psychometric measures and psychosocial measures was utilised (Supplementary Table 1). Participants were compared to normative data in terms of gender, age and intellectual function (Supplementary Table 2).
Procedure
The study was reviewed and given favourable opinion by The Research Ethics Committee HSC REC B (REC Ref. 16/NI.0041) prior to its commencement. All eligible participants were contacted using a mailed consent pack. Psychometric and psychosocial measures were administered in adherence to standardised administration guidelines by a Trainee Clinical Psychologist under supervision of a Consultant Neuropsychologist. A brief semi-structured interview explored subjective views of cognitive impairment. Performance validity was examined using the Rey-15 Item Test.
Data analysis
Clinical significance of cognitive tests were examined with reference to existing age scaled scores derived from an adult normative sample. Comparisons of mean performance of the clinical sample and normative data were facilitated by calculation of effect size (Cohen’s d) and One Sample t-Test where appropriate.
Results
Cognitive outcomes are summarised in Table 1. Overall mean performance for AN participants was compared to the pooled mean performance of the normative population. As Table 1 illustrates participants were relatively preserved across a number of cognitive domains including memory and learning, object spatial perception as well as some certain aspects of executive function.
Mean cognitive outcomes for AN participants relative to age norms
Mean cognitive outcomes for AN participants relative to age norms
Comparison based on pooled mean of normative data. *Timed task with greater score indicating poorer performance. Brixton Spatial Anticipation Test; Repeatable Battery for the Assessment of Neuropsychological Status (RBANS); Test of Everyday Attention (TEA); Wechsler Adult Intelligence Scale (WAIS IV); Grooved Peg Board Test (GPB).
On tasks of selective (auditory distractibility) and divided attention (auditory and visual attention), participants performed below what would be expected when compared to normed data. Notably, the divided attention task has an auditory component and most (89.5%) of the sample reported experiencing hearing decline and tinnitus post-treatment. Nevertheless their performance compared to hearing impaired norms (Robertson, Ward, Ridgeway and Nimmo-Smith, 1994) showed disturbances in attention persisted to significance level (Supplementary Table 3). On another timed task (the Grooved Peg Board, a timed visuo-motor coordination task), participants performed below the mean of an equivalent non-clinical sample. When performance was matched on age Cohen’s d calculation ranged from 0.33–2.24. One sample t Test showed that the overall difference in mean performance when compared to normed data was not significant with exception to the youngest members of the sample (40–49 years).
Participant’s cognitive performance was also compared by tumour site (Left Sided Tumour n = 9; Right Sided Tumour n = 10) and is detailed in Supplementary Table 4. On the Brixton Spatial Anticipation Test (an untimed rule formation and cognitive flexibility task), those with a left sided tumour showed a small effect size with mean performance below normative data. A medium effect size (d = 0.40) above the normed population was observed for those with a right sided tumour. Those with a right sided tumour performed below the normed mean on a processing speed task. Whereas those with a left sided tumour were equivalent to age norms. On verbal learning tasks (immediate recall of a word list and short story), the performance of those with a right sided tumour was comparable to normative data, while those with a left sided tumour performed above the population mean. On a task of delayed visual memory (drawing of a previously presented figure) those with a right-sided AN performed below normative data, while those with a left sided tumour performed better on visual memory tasks compared to normed data (d = 0.49). On psychomotor speed tests (Grooved Peg Board), both groups showed performance below normative data with a large effect size observed.
Psychosocial outcomes
Table 2 illustrates data on a psychosocial measure of distress (DASS-21: Henry & Crawford, 2005). Endorsed symptoms of mood and stress were found to be within normal limits and equivalent to the general population (d = 0.12; d = 0.13). Cohen’s d calculation revealed a small effect size (d = 0.35) for anxiety symptoms compared to normative data (M = 3.76; SD = 5.90). One Sample t Test showed the difference in endorsed anxiety symptoms compared to the general population was not significant (t (18)=1.72, p = .102).
Psychosocial outcomes for AN group vs. normative population
Psychosocial outcomes for AN group vs. normative population
Depression Anxiety Stress Scale-21 (DASS-21); Penn Acoustic Neuroma Quality of Life Scale (PANQUOL).
Self-reported quality of life using the disease specific measure PANQUOL Scale (Shaffer, Cohen, Bigelow & Ruckenstein, 2010) showed less reported problems with facial dysfunction, balance, hearing, energy, pain and overall better HRQOL compared to normed data. Cohen’s d calculations revealed a medium effect size (d = 0.72) with overall better self-reported quality of life among the AN group compared to normed data which reached significance (Supplementary Table 5).
Participants were asked about their subjective view of cognitive function, 11(55%) endorsed memory disturbance since treatment, while 8 (40%) identified no perceived decline. As Table 3 illustrates when the mean performance on memory tasks of those who reported memory problems was compared to individuals who did not perceive memory problems, no effect size was found on a task of new learning (12-item story) (d = 0.10) and visual memory (d = 0.01). A small effect size was observed between means for a learning task (10-item word list) (d = 0.22) and a word list recognition task (d = 0.39). Notably, the mean performance of those who perceived memory decline since treatment was better than those who did not perceive a decline in memory function. A medium effect size (d = 0.59) was found for list recall performance, with those who reported memory disturbance since treatment having a higher overall mean score compared to normed data and also to those who did not report memory disturbance.
Mean performance for those with subjective memory decline, those who did not and normed data
Mean performance for those with subjective memory decline, those who did not and normed data
Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) based on the pooled mean of normed data.
Five participants (25%) complained of reduced ability to sustain attention since treatment while 14 (75%) did not. However, on objective assessment attention was found to be impaired among the AN population relative to normative data. As Table 4 illustrates there was no effect size (d = 0.13) found when the means of those citing a decline in attention compared to those who did not on a task of selective attention. In terms of divided attention a small-medium effect size (d = 0.47) was observed, with those who did not report problems with attention showing a lower mean performance compared to normed data and also to individuals who reported decline in their attention.
Mean performance for those who perceived decline in attention, those who did not and normed data
Test of Everyday Attention (TEA).
In Table 5, when overall self-reported health related quality of life was compared for those who perceived a decline in their cognitive function post treatment and those who did not, a large effect size was observed (d = 1.63).
Comparison of subjective cognitive decline and self-reported psychological distress
Penn Acoustic Neuroma Quality of Life Scale (PANQUOL).
This regional single centre study examined cognitive and psychosocial outcomes in individuals who received SRS treatment for AN. Unfortunately, no standardised pre-treatment standardised assessment of cognition was conducted, post-treatment cognition including performance validity was assessed using a battery of neuropsychological tests. Given the primary effects of radiation through SRS reported in the literature for other tumour manifestations (Aoyama, Shirato, Nishioka et al., 2001; Chang, Shirator, Aoyama et al., 2004), it was predicted participants would show cognitive impairments relative to population norms. Findings are pertinent given the increased use of SRS in the treatment of benign tumours (Hasegawa et al., 2013) and recognition of the long-term effects of radiation treatment on overall quality of life (Scheibel, Meyers & Levin, 1996).
Results showed relatively preserved cognitive function compared to age-equivalent norms in terms of verbal memory, visuospatial/constructional abilities, psychomotor speed and information processing speed, verbal fluency and sequencing. Findings are consistent with previous studies exploring the outcome of SRS among those with other cerebral lesions (e.g. meningioma, pituitary adenomas and cerebral arteriovenous malformations), which have shown similar stability and in some cases improvement in cognitive profile over time (2–3 years) (Kangas, Tate, Williams et al., 2012; Murray, Dally, Jeffreys et al., 2014; Tooze, Gittoes, Jones et al., 2009). Notwithstanding participants did show discrete impairments in attention, visual memory and psychomotor speed. Previous studies exploring radiation exposure through SRS for other tumour types have also reported impairment in verbal fluency and abstract reasoning (Kangas, Tate, Williams et al., 2012). However, in the current study tests of visual speed and divided attention (multi-tasking) detected disturbance in aspects of attention which is a novel finding relative to otherwise preserved cognitive functioning. Although participants performed within normal limits on a test of executive function involving cognitive flexibility. On a task of dual attention involving auditory input and output, processing speed and visual search, individuals showed greater impairment. In addition, sustained attention, dividing attention between two simultaneous tasks and the ability to inhibit irrelevant material shows non-clinical age-related decline which may have contributed to the outcome profile observed (Commodari & Guarnera, 2008). Traditional theories of lateralisation might in part explain the visual memory impairments observed among right-sided AN participants (Gasparini, Hufty, Masciarelli et al., 2008; Scheibel, Meyers & Levin, 1996).
The variability in premorbid cognitive function (estimates based on performance on the TOPF and education and employment history) among the sample is notable and has implications for the results. While most individuals fell within average limits, those whose pre-treatment cognitive ability was estimated in the ‘Superior’ and ‘High Average’ range showed a likely decrement in ability across some cognitive domains (Supplementary Table 6) which is likely to be perceived as a significant decline relative to pre-morbid functioning.
Psychosocial outcomes
Among participants, levels of self-reported anxiety and depression were within the normal range and equivalent to the general population (Henry & Crawford, 2005). Overall health related quality of life was higher when compared to other AN populations (Shaffer, Cohen, Bigelow et al., 2010). Previous AN studies have document that the incidence of anxiety and depression is comparable to the general population and found time since treatment, symptoms and comorbid ill-health as most predictive of elevated anxiety and depression (Brooker, Fletcher, Dally et al., 2014). In this study, it is possible both the mean time since SRS treatment (33.4 months) and high rates of quality of life found by the PANQUOL contributed to the low incidence of psychological distress observed. Of note, the association between distress and AN management has not been consistently reported in the literature (Brooker, Fletcher, Dally et al., 2014; Carlson et al., 2015). Current findings do not support previous studies which have proposed elevated rates of anxiety among patients who have undergone radiation exist because the tumour, although controlled, and in some cases reduced, remains in situ (O’Reilly, Murray & Hadley, 2008).
Earlier literature observed that receiving a diagnosis of AN rather than the treatment per se most significantly impacted quality of life (Carlson et al., 2015). This may have contributed to overall better HRQOL among the study’s sample given the difference in mean time from diagnosis to treatment to data collection (33.4 months). Further, it has been proposed that the secondary effects of SRS may not be evident until several years after treatment, thus assessing HRQOL among this sample was timely (Carlson et al., 2015). It may also support the existing evidence which describes the complex and dynamic adjustment trajectory of those with a chronic illness overtime (Chang et al., 2009). Finally, the higher HRQOL among the AN population in the present study may also be explained by the largely spared cognitive function observed, given previous studies which report on the associations between poorer quality of life and cognitive decline in a variety of clinical populations (Lawson, Yarnall, Duncan et al., 2014).
Subjective cognitive decline
Participant’s subjective view of their cognitive function since treatment was explored, those who reported cognitive decline (in memory and attention) showed equivalent or better performance on testing relative to those who did not. This finding supports previous literature which reports a modest relationship between subjective reports and objective assessment of cognitive function (Gehring, Taphoorn, Sitskoorn et al., 2015). While causality cannot be determined, those with subjective cognitive decline (SCD) had poorer self-reported quality of life consistent with previous studies which observed a relationship between cognitive function and quality of life (Pusswald, Moser, Pfluer et al., 2016). This discrepancy between objective test findings and subjective cognitive performance has been attributed to the presence of psychological distress in the literature (Studer, Donati, Popp et al., 2013) and is consistent with reports that individuals with greater psychological distress are more likely to perceive a decline in functioning as more severe compared to those with no reported distress (Schagen, Klein, Reijneveld et al., 2014). Notably, impairment in attention ability was observed and those who reported subjective decline were accurate in their perception compared to those who did not. Finally, reduced awareness or psychological minimisation may explain this discrepancy given findings which report individuals can underreport cognitive deficits in clinical settings or be unaware of symptomatology until objective cognitive measures are administered (Roberts, Clare, Woods, 2009).
Study findings augment the evidence base regarding the SRS efficacy for AN, which to date has mostly focused on the primary effects on tumour control and physical morbidity, by offering insight into the cognitive and psychosocial sequelae following AN treatment. For specialists working in this area the study offers useful information, which may aid clinical decision making and provide greater clarity around the potential risks and benefits of treatment. The clinical significance of the relatively mild toxicity observed, in particular, the temporal lobe as a radiation “avoidance” structure relative to the brainstem is notable. The study also recognizes that those patients with brainstem and cerebellum involvement who show neuropsychological impairment (Schmahmann & Sherman, 1998; Tavano, 2007; Schmahmann, 2018), could be impacted by the effects of potential incidental irradiation. Further, the comparison of subjective and objective cognitive profiles alongside HRQOL is notable given research which describes the mediating effect of cognition on psychological distress (e.g. low mood) (Lam, Kennedy, McIntyre et al., 2014). These findings also offer a tentative contribution to health related evidence base regarding perception of health symptoms, psychological distress and quality of life. Finally, the finding that those who perceived a decline in their cognitive function reported poorer overall quality of life, contributes to the increased recognition of HRQOL measures in addition to traditional outcome measures (e.g. survival rates) in neuro-oncology settings and research (Witgert & Meyers, 2011).
Study limitations
While all participants were community dwelling with no known progressive neurological conditions documented, the impact of premorbid function on outcome cannot be conclusively controlled for. The study employed a measure of estimated premorbid cognitive function in combination with demographic variables which has its limitations particularly domain specific cognitive functioning. Future studies will benefit from pre-treatment neuropsychology assessment. Given current observations, future longitudinal studies should further explore the relationship between psychological and cognitive functioning and potential changes in these variables over time. In addition, it is possible that selection bias may have influenced sample representativeness in relation to health, education and socio economic status. Consequently, future studies involving larger multi-centre recruitment which offers direct comparison to other methods of treatment are likely to be of value.
In conclusion, this study examined the cognitive and psychosocial outcomes for patients who have undergone SRS for AN. Results are largely consistent with findings on the effects of SRS reported for other clinical groups, which support SRS as a targeted method of radiation treatment in AN. Findings of the current study indicated that patients treated with SRS demonstrate relatively preserved cognitive function despite their baseline disease. Finally, tentative findings that those who reported SCD also endorse poorer self-reported HRQOL have important implications for treating clinicians in relation to assessment of depressive symptoms and health related distress.
Footnotes
Acknowledgments
The authors extend their gratitude to all participants and wish to acknowledge their time commitment, enthusiasm to contribute to the clinical knowledge base. Finally, the invaluable assistance of Dr Donncha Hanna, Queen’s University Belfast in relation to statistical analysis and data interpretation is acknowledged.
Conflict of interest
This study was co-sponsored by The Queen’s University Belfast and The Belfast Health and Social Care (HSC) Trust. The authors did not receive any third-party financial support and therefore declare no conflicts of interest.