
Abstract
BACKGROUND:
Laryngeal penetration, which is a less serious form of aspiration, should be considered in patients with stroke to ensure early detection of risk of laryngeal aspiration and prevention of pneumonia.
OBJECTIVE:
As a follow-up to a previous study that demonstrated the association of pharyngeal width to laryngeal aspiration, the present study sought to determine whether the pharyngeal width was related to not only laryngeal aspiration but also laryngeal penetration in patients with deglutition disorder following stroke.
METHODS:
The pharyngeal width on the roentgenogram was measured and compared based on the severity of aspiration. Moreover, the optimal cut-off points were determined for predicting the penetration and aspiration so that the difference between the penetration and the aspiration could be elucidated.
RESULTS:
The pharyngeal width of the patients was wider than the controls. The increase of the pharyngeal width by aspiration severity was more evident in the patients with chronic and right cerebral stroke. The optimal cut-off point of the pharyngeal width was approximately 1 mm lesser for the prediction of penetration than for aspiration.
CONCLUSIONS:
The pharyngeal width could be an ancillary method for detecting penetration and aspiration in stroke patients.
Introduction
This study is a continuation of a previously published study (Jung et al., 2019), in which we reported the relation between the pharyngeal width and laryngeal aspiration in 270 patients with dysphagia following stroke. Herein, we report the pharyngeal width as a value for detecting laryngeal aspiration as well as the laryngeal penetration, which is a milder form and a predictor of laryngeal aspiration in 690 patients with stroke.
The pharynx is formed by the pharyngeal muscles that determine the shape of its lumen. The pharyngeal width of patients with post-stroke dysphagia was reported to be wider than that of healthy controls; this was interpreted as a phenomenon caused by low strength and decreased pharyngeal muscle tone following stroke (Jung et al., 2019). Moreover, the change in the pharyngeal width over the course of stroke was consistent with the change in the degree of dysphagia (Baek et al., 2020).
Laryngeal penetration during the swallowing process is defined as the passage of materials into the laryngeal space but not beyond the true vocal cords. It is a less severe symptom than laryngeal aspiration. In contrast, laryngeal aspiration is defined as the entry of bolus material below the true vocal cords (Rosenbek, Robbins, Roecker, Coyle, & Wood, 1996). Laryngeal penetration may progress into laryngeal aspiration, a risk factor for pneumonia (Friedman & Frazier, 2000; Gurberg, Birnbaum, & Daniel, 2015; Ha, Kim, Park, & Eun, 1999). Ha et al. and Friedeman et al. reported that over 70%of people with penetration eventually developed aspiration (Friedman & Frazier, 2000; Ha, Kim, Park, & Eun, 1999). Patients with laryngeal penetration on videofluoroscopic swallowing study (VFSS) were approximately four times more likely to develop pneumonia than those with normal swallowing (Pikus et al., 2003). Therefore, patients who experience only laryngeal penetration should be closely observed to prevent complications. Evaluating the risk of laryngeal penetration as a separate diagnostic event is essential to distinguish it from aspiration in swallowing function studies.
Hence, the present study aimed to compare the pharyngeal widths based on the aspiration severity, the stage and lesion location of stroke, and to determine the two different cut-off values of pharyngeal width for detecting penetration and aspiration.
Methods
Participants
This retrospective analysis was based on the medical charts of 1150 patients who complained of swallowing difficulty and/or aspiration during a meal and had undergone VFSS in the dysphagia rehabilitation clinic. A total of 690 patients who fulfilled the inclusion and exclusion criteria were included in our study (Table 1). The inclusion criteria were as follows: (1) stroke diagnosed through computed tomography and/or magnetic resonance imaging, (2) age 20 years or above, (3) alert level of consciousness (Raman, Sreenivas, Puliyel, & Kumar, 2011; Wasserman et al., 2015), and (4) underwent complete VFSS with lateral neck roentgenogram. The exclusion criteria were as follows: (1) history of other neurovascular diseases, (2) history of cervical spine, head, or neck surgery, (3) tracheostomy condition, and (4) the oral and/or oesophageal phasic dysphagia as confirmed on VFSS. The stroke group was subdivided into acute stroke (duration of stroke≤30 days) and chronic stroke (duration of stroke > 30 days) groups based on stroke duration and subdivided into cerebral hemisphere (right or left hemisphere), cerebellum, and brainstem stroke groups based on stroke lesion location. Additionally, we included the data of 56 people who participated in the previously published studies (Baek et al., 2020; Jung et al., 2019; Lee et al., 2019; Song et al., 2020) with normal swallowing function.
Participants’ demographics and clinical characteristics
Participants’ demographics and clinical characteristics
Age, height, weight, neck circumference, and grasp power are average±standard deviation. PAS, Penetration-Aspiration Scale; NA, Not applicable. *p < 0.05 using analysis of variance (ANOVA) test with post hoc Tukey’s test between whole stroke group, acute stroke group, chronic stroke group, and control group.
Participants’ characteristics such as age, height, weight, neck circumference, and grasp power (of the hemiplegic hand in the stroke group and the dominant hand in the control group, measured using a hydraulic hand dynamometer) were used in our analysis. All aspects of the study, including enrolment, clinical assessment, VFSS protocol, and statistical analysis, were approved by the local Institutional Review Board (IRB No. 2020-05-008-002).
The method to measure pharyngeal width was the same as in the previous studies (Baek et al., 2020; Jung et al., 2019; Lee et al., 2019; Song et al., 2020). Using the lateral neck roentgenograms, the average of the two pharyngeal widths, [A + B]/2, was calculated and referred to as the JOSCYL width, which is a combination of the first letters of the authors’ surnames used in our previous study (Fig. 1). Furthermore, we measured the adjusted pharyngeal width-related value, as the JOSCYL scale, obtained by the formula ‘JOSCYL width x 100/Neck circumference (mm)’, as the neck size may affect the pharyngeal width.
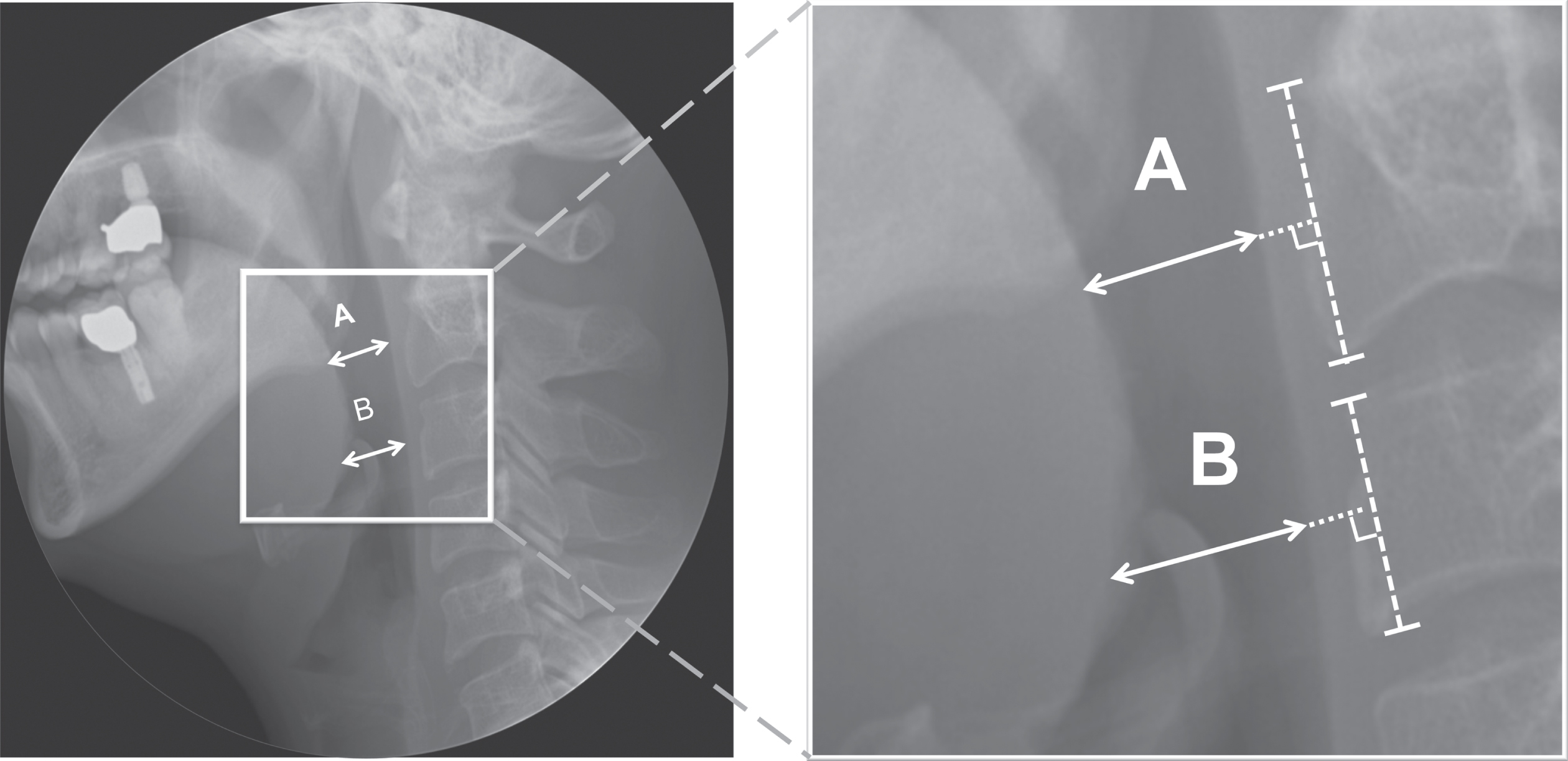
The JOSCYL width. The two lines, lines A and B, were both perpendicular to the posterior pharyngeal wall and were located at the following positions: (1) line A around the mid-oropharynx corresponding to the middle level of the second (C2) vertebral body, and (2) line B around the lower oropharynx, corresponding to the middle level of the third cervical (C3) vertebral body. The average of the two pharyngeal widths, [A + B]/2, was named as the JOSCYL width.
Next, the swallowing study had been conducted using the protocols routinely followed at our centre. Three types of diets with different viscosities (semisolid, liquid, and solid were prepared to be similar to Greek yogurt, juice, and Korean rice cake, respectively) were tested in the swallowing study (Nicosia & Robbins, 2007). After the swallowing study, the physician rated the patient on the penetration-aspiration scale (PAS) (Rosenbek et al., 1996). The PAS score 1 indicates no penetration and no aspiration, the PAS scores from 2 to 5 indicate penetration and no aspiration, and the PAS scores from 6 to 8 indicate aspiration.
Sex in each group (whole stroke, acute stroke, chronic stroke, and control) was analysed using the chi-square test. Age, height, weight, and neck circumference in each group were compared using an analysis of variance (ANOVA) test with a post-hoc Tukey’s test. Grasp power of the three-stroke groups was compared using an analysis of variance (ANOVA) test with a post-hoc Tukey’s test.
The JOSCYL widths and JOSCYL scales based on the stroke stage and the stroke lesion location were compared using an ANOVA test with a post-hoc Tukey’s test between each stroke group and control group. Furthermore, the JOSCYL width and JOSCYL scale according to the aspiration severity of VFSS (no penetration/aspiration; PAS 1, penetration; PAS 2–5, and aspiration; PAS 6–8) were compared using an ANOVA test with a post-hoc Tukey’s test in each stroke group.
Correlations between the patient’s characteristics and the JOSCYL width and JOSCYL scale were evaluated in the whole stroke group using the Spearman correlation analysis. Correlations between the JOSCYL width, JOSCYL scale, and dysphagia severity scales represented as PAS were evaluated in each group using the Spearman correlation analysis. Additionally, we determined the optimal cut-off points of the JOSCYL width and JOSCYL scale for predicting laryngeal penetration and aspiration in each stroke group, except cerebellum and brainstem groups with small numbers participants, via receiver operating characteristic curve analyses. All the statistical analyses were performed using SPSS Statistics software ver. 24 (IBM Corp., Armonk, NY, USA), and the level of statistical significance was set to p-values < 0.05 and confidence intervals (CIs) > 95%.
Results
Participant characteristics
Sex, age, weight, and neck circumference were not different between the groups (Table 1). Height was larger in the whole stroke group and the chronic stroke group compared to the control group (p < 0.05). Grasp power was larger in the acute stroke group than the whole stroke and chronic stroke groups (p < 0.05).
JOSCYL width and JOSCYL scale
The JOSCYL widths were 17.45±6.21 mm, 17.10±5.75 mm, 17.60±6.41 mm, and 14.68±4.01 mm in the whole stroke, acute stroke, chronic stroke, and control groups, respectively. The JOSCYL widths in each stroke group were wider than that of the control group (p < 0.05) (Fig. 2a). The JOSCYL scales were 4.90±1.78, 4.82±1.60, 4.95±1.86, and 4.23±1.16 in the whole stroke, acute stroke, chronic stroke, and control groups, respectively. The JOSCYL scales of the whole stroke group and the chronic stroke group were significantly larger than that of the control group (p < 0.05) (Fig. 2b).

JOSCYL width and JOSCYL scale according to stroke stages. The JOSCYL widths of the whole stroke, acute stroke, and chronic stroke groups were wider than those of the control group (p < 0.05) (a). The JOSCYL scales of the whole stroke and chronic stroke groups were larger than those of the control group (p < 0.05) (b). *p < 0.05 using ANOVA test with post-hoc Tukey’s test between the whole stroke, acute stroke, chronic stroke, and control groups.
In addition, the JOSCYL widths were 18.49±6.36 mm, 17.03±5.80 mm, 18.49±7.48 mm, and 18.45±5.67 mm in the right cerebral hemisphere, left cerebral hemisphere, cerebellum, and brainstem stroke groups, respectively. The JOSCYL widths of the right cerebral hemisphere and brainstem lesion group were wider than that of the control group (p < 0.05) (Fig. 3a). The JOSCYL scales were 5.20±1.84, 4.78±1.65, 5.24±2.23, and 5.11±1.47 in the right cerebral hemisphere, left cerebral hemisphere, cerebellum, and brainstem stroke groups, respectively. The JOSCYL scales of the right cerebral hemisphere and brainstem lesion group were larger than that of the control group (p < 0.05) (Fig. 3b).
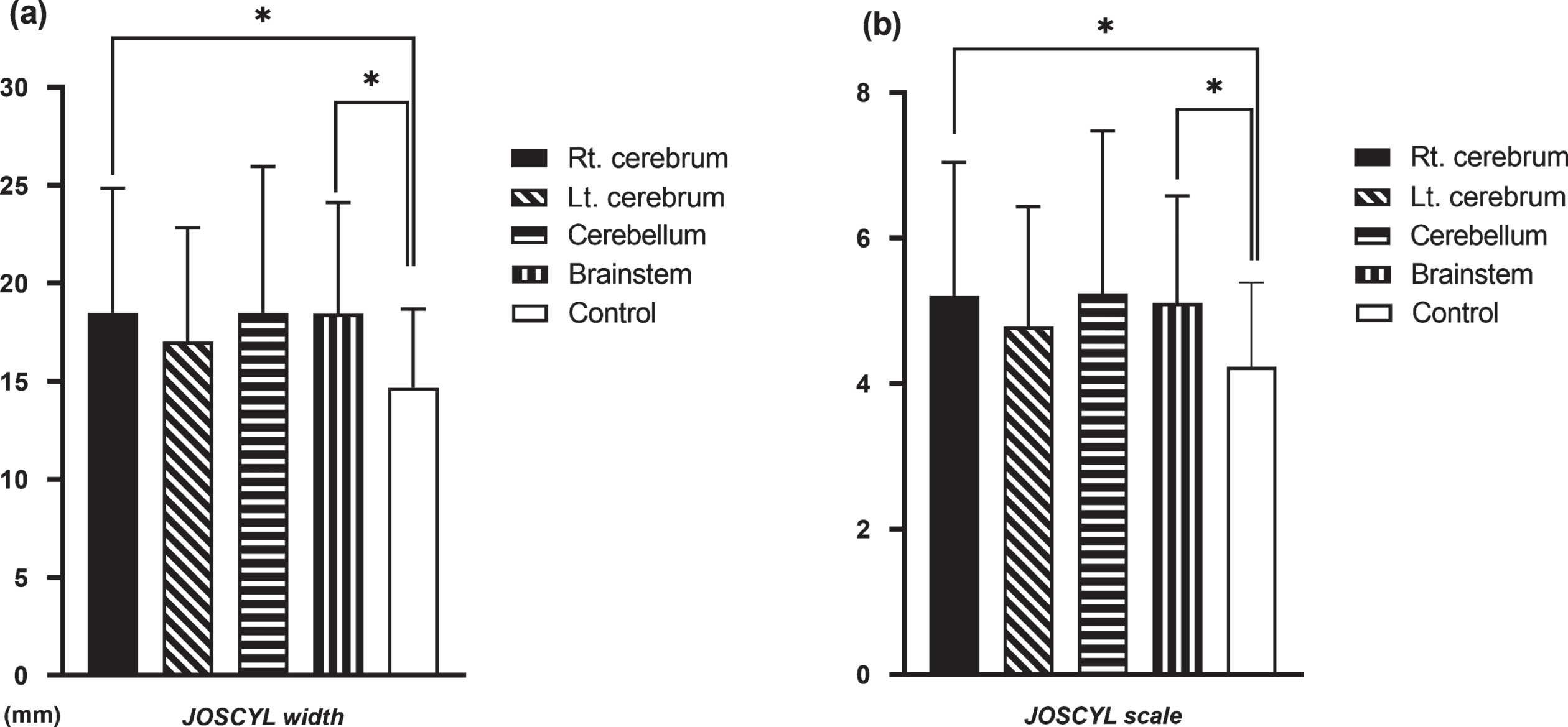
JOSCYL width and JOSCYL scale according to stroke lesion location. The JOSCYL widths of the right cerebral hemisphere and brainstem group were wider than that of the control group (p < 0.05) (a). The JOSCYL scales of the right cerebral hemisphere and brainstem group were larger than that of the control group (p < 0.05) (b). There was no significant difference of the JOSCYL width and scales among every stroke lesion groups. *p < 0.05 using ANOVA test with post-hoc Tukey’s test between the stroke lesion groups and control group.
The JOSCYL width was larger in patients with aspiration (PAS 6–8) than patients without penetration/aspiration (PAS 1) (p = 0.003 in the whole stroke group, p = 0.023 in the chronic stroke group) and patients with penetration (PAS 2–5) (p = 0.026 in the whole stroke group, p = 0.032 in the chronic stroke group) (Table 2). The JOSCYL scale was larger in patients with aspiration (PAS 6–8) than patients without penetration/aspiration (PAS 1) (p = 0.007 in the whole stroke group, p = 0.027 in the chronic stroke group) and penetration group (PAS 2–5) (p = 0.048 in the chronic stroke group) (Table 2). In addition, the JOSCYL width and the JOSCYL scale were larger in patients with aspiration (PAS 6–8) than patients without penetration/aspiration (PAS 1) in the right cerebral hemisphere stroke group (JOSCYL width; p = 0.014, JOSCYL scale; p = 0.007) (Table 3). Meanwhile, in patients with similar aspiration severity, the JOSCYL width and the JOSCYL scale were not different in stroke stage and stroke lesion.
JOSCYL width and JOSCYL scale according to aspiration severity and stroke stage
*p < 0.05 using analysis of variance (ANOVA) test with post hoc Tukey’s test between three different severity scale (No penetration/aspiration, penetration, and aspiration) in each stroke group.
JOSCYL width and JOSCYL scale according to aspiration severity and lesion location
*p < 0.05 using analysis of variance (ANOVA) test with post hoc Tukey’s test between three different severity scale (No penetration/aspiration, penetration, and aspiration) in each stroke lesion group.
The JOSCYL width of the whole stroke group was significantly correlated with age (r = 0.107, p =0.005), height (r = 0.164, p < 0.001), weight (r =0.079, p = 0.038), and neck circumference (r = 0.159, p = 0.000). The JOSCYL scale of the whole stroke group was correlated with age (r = 0.142, p < 001). The JOSCYL width and the JOSCYL scale of the whole stroke group, chronic stroke groups (Table 4), and right cerebral hemisphere group (Table 5) were significantly correlated with the PAS.
Correlation of JOSCYL width and JOSCYL scale with dysphagia scale according to stroke stage
Values are correlation coefficient (p-value). *p < 0.05 using Spearman’s rank correlation test. PAS, Penetration-Aspiration Scale.
Correlation of JOSCYL width and JOSCYL scale with dysphagia scale according to stroke lesion
Values are correlation coefficient (p-value). *p < 0.05 using Spearman’s rank correlation test. PAS, Penetration-Aspiration Scale.
The optimal cut-off points of the JOSCYL width for predicting penetration were 16.3 mm, 16.6 mm, 15.8 mm, 17.2 mm, and 15.4 mm in the whole stroke, acute stroke, chronic stroke, right cerebral hemisphere, and left cerebral hemisphere group, respectively. The optimal cut-off points of the JOSCYL scale for predicting penetration were 4.62, 4.64, 4.53, 4.69, and 4.48, respectively (Table 6). The optimal cut-off points of the JOSCYL width for predicting aspiration were 17.0 mm, 17.0 mm, 17.0 mm, 18.0 mm, and 16.4mm, respectively. The optimal cut-off points of the JOSCYL scale for predicting aspiration were 4.79, 4.81, 4.77, 5.10, and 4.64, respectively (Table 7).
Accuracy of JOSCYL width and JOSCYL scale for detecting penetration
Accuracy of JOSCYL width and JOSCYL scale for detecting aspiration
This study confirmed that the JOSCYL width and scale increased significantly in the patients with dysphagia than normal controls. The increase was evident in the patients with aspiration compared to the patients with penetration, evident in the chronic stroke stage. In the acute stroke stage, the JOSCYL width and JOSCYL scale were not different between the patients with penetration and aspiration. Based on the location of the stroke lesions, the above trend was evident only in patients with a lesion in the right cerebral hemisphere.
Differences in outcomes from stroke stages are thought to be due to various comorbid symptoms in the acute stage. The increase in pharyngeal width in the chronic stage, where many comorbid symptoms are resolved, and sensory-motor dysfunction is the main cause of dysphagia, will work better as a determinant of aspiration. The location of the stroke lesion influences the neuromuscular response of an individual in swallowing. Previous studies have found that the right hemisphere is more involved in the pharyngeal phase of swallowing and the left hemisphere is more involved in the oral phase (Hamdy et al., 1996; Mosier, Liu, Maldjian, Shah, & Modi, 1999; Teismann, Dziewas, Steinstraeter, & Pantev, 2009). The right hemisphere lesion, primarily including insula cortex, sensory-motor integration area, and corresponding white matter tracts, delayed pharyngeal swallowing, and increased pharyngeal stasis (Daniels, Foundas, Iglesia, & Sullivan, 1996). The left hemisphere lesion, especially in the inferior frontal lobe and precentral gyrus, was associated with reduced tongue movement and prolonged oral transit time (Jang, Yang, Yang, & Kim, 2017; Saito, Hayashi, Nakazawa, & Ota, 2016). Brainstem lesions can affect the sensory-motor dysfunction of the mouth, tongue, and pharynx and pose broad problems at the pharyngeal contraction, laryngeal elevation, glottic closure, and cricopharyngeal relaxation (Flowers, Skoretz, Streiner, Silver, & Martino, 2011; Horner, Buoyer, Alberts, & Helms, 1991; Kim, Cha, & Lee, 2019; Veis & Logemann, 1985). Our study revealed that the patients with a stroke lesion in the right cerebral hemisphere or brainstem showed the larger JOSCYL width and scale, and it was consistent with previous studies that confirmed the relationship between stroke lesion and swallowing physiology. Moreover, the JOSCYL width and scale differences according to aspiration severity were evident in the patients with stroke in the right hemisphere, and this could be interpreted as a tendency for the pharyngeal phase of swallowing to be associated with the right hemisphere rather than the left hemisphere.
This study focused on the laryngeal aspiration and laryngeal penetration that has not been focused on in our previous studies (Baek et al., 2020; Jung et al., 2019). The time delay in laryngeal vestibule closure, shortening of closure duration, and insufficiency of the epiglottic closure determine the depth to which the material would enter the laryngeal vestibule during swallowing. Penetration occurred when these factors were less severe, and aspiration occurred as they worsen. Therefore, laryngeal penetration is particularly important given its fairly strong association with laryngeal aspiration (Friedman & Frazier, 2000; Kiyohara et al., 2018; Seo, Oh, & Han, 2016). In our previous study on senile dysphagia, the pharyngeal width could differentiate between the risk of penetration and aspiration. The cut-off point of the pharyngeal width to detect the penetration was 2 mm lower than aspiration (Song et al., 2020).
This study supports our hypothesis whereby decreased muscle strength and muscle tone following stroke might maintain the pharyngeal lumen larger than normal at rest. The pharynx has been shown to atrophy as a natural aging process in healthy elderly individuals and appears increased in pharyngeal volume and area, as measured by acoustic pharyngometry, fluoroscopy, and computed tomography (Aminpour, Leonard, Fuller, & Belafsky, 2011; Inamoto et al., 2015; Leonard, Kendall, & McKenzie, 2004; Molfenter et al., 2015). These changes can negatively affect the deglutition. People with a larger pharyngeal lumen than normal demonstrated lesser pharyngeal constriction and a larger amount of post-swallowing pharyngeal residue (Molfenter, Lenell, & Lazarus, 2019). In patients with Parkinson’s disease, the pharyngeal areas were larger than those in healthy people, associated with maladaptive changes to swallowing kinematics and material residue, eventually increasing the incidence of laryngeal penetration and laryngeal aspiration (Curtis, Molfenter, & Troche, 2020). Similarly, post-stroke pharyngeal muscle weakness may result in an enlargement of the pharyngeal area, and this change could manifest as an increase in the pharyngeal width on the lateral neck roentgenogram in this study.
Several clinical features could have affected the pharyngeal width. The JOSCYL width showed significant positive correlations with age and body size features (height, weight, and neck circumference). The positive correlation with age can be explained by the fact that the swallowing musculature tends to develop sarcopenic changes associated with aging, leading to increased pharyngeal width and increased aspiration prevalence in elderly people (Lee et al., 2019; Song et al., 2020). There is a need to exclude the possibility of the JOSCYL width being affected by the body size; therefore, we suggest that the JOSCYL scale (JOSCYL width divided by neck circumference) may be a reasonable indicator of laryngeal penetration and laryngeal aspiration. Accordingly, we found that the JOSCYL scale was only correlated with age and had similar sensitivity and specificity as the JOSCYL width. Thus, the JOSCYL scale can be a useful indicator for people who have a very large or small body size.
The optimal cut-off points of the JOSCYL width and scale for predicting penetration were shorter and lower than those for predicting aspiration, though the difference was very small (approximately 1 mm). This supports the suggestion that laryngeal penetration is more common and may appear when there is less oropharyngeal dysfunction than laryngeal aspiration in patients with stroke. However, the sensitivities and specificities of the cut-off values were insufficient to be noteworthy as independent screening factors. The sensitivities and specificities of the cut-off values for detecting aspiration were not improved in this study despite including many patients with stroke compared to the previous study, including 270 stroke patients. Therefore, the JOSCYL width and scale can be used as ancillary methods to detect laryngeal penetration and laryngeal aspiration in patients with stroke.
There were limitations in this study. First, there were fewer controls (n = 56) compared to the stroke patients. We focused on the analysis within each stroke group because this study aimed to confirm the relationship between the pharyngeal width and the severity of aspiration/penetration of stroke patients with dysphagia. Although we thought that there was no limit to the number of controls applied in statistical description, the large difference in the number of participants between groups is a limitation. Second, we did not evaluate the effects of the lesion volume and its secondary load on white matter, the pharyngeal size, and penetration/aspiration. Hence, further evaluations are required in a future study. Third, because the number of patients with a lesion in the cerebellum and brainstem is smaller than that of the cerebral hemisphere, the analyses related to those groups may be less reliable. Therefore, we did not obtain the cut-off values of the JOSYCL width and scale for predicting penetration/aspiration in patients with a lesion in the cerebellum and brainstem.
In conclusion, this study is a continuation of our previous study. The main updated points observed were that the JOSCYL width and scale increase was more evident in the patients with aspiration than the patients with penetration, which was evident in the chronic stroke stage. In addition, based on the location of the stroke lesions, the above trend was more evident in patients with a lesion in the right cerebral hemisphere. The cut-off points of the JOSCYL width and scale for predicting laryngeal penetration were shorter and lower than those for predicting laryngeal aspiration, regardless of the stroke stage and lesion location. Therefore, the JOSCYL width and scale can be used as ancillary methods to detect laryngeal penetration and aspiration in patients with stroke. Hence, physicians’ attention to laryngeal penetration would be helpful in the early rehabilitation of dysphagia, thereby preventing aspiration.
Conflict of interest
The authors declare no conflicts of interest.