
Abstract
BACKGROUND:
No general recommendations are yet available for the application of robot-assisted treadmill therapy for children with cerebral palsy regarding the length and intensity of the intervention.
OBJECTIVE:
The aim of the study was to evaluate patient-specific determinants of responsiveness to robot-assisted gait training (RAGT) in patients with bilateral spastic cerebral palsy.
METHOD:
During 12 months, the patients underwent 1–4 blocks of RAGT, representing 16–82 TUs. The following parameters were evaluated before (V0) and after each therapeutic block (V1–V4): dimension A (lying and rolling), B (sitting), C (crawling and kneeling), D (standing), E (walking, running and jumping) of the Gross Motor Function Measure (GMFM-88). We evaluated the change in motor functions in relation to the severity of disability, age, gender and number of therapeutic units.
RESULTS:
Ninety-seven patients aged between 3.7 and 27 years (mean age 10.02 years (SD±5.29); Gross Motor Function Classification System level I [n = 5], II [n = 25], III [n = 48], IV [n = 19]) underwent 16–82 TUs (overall average number 34.06 TUs, SD±16.41) of RAGT. In the patient group, we recorded clinically meaningful improvement and statistically significant improvement (p < 0.001) in gross motor functions with gradual increase in the effect size after each therapeutic block. Using correlation and regression analysis, we found a statistically significant associations between the number of therapeutic units, severity of disability, and improvement in motor functions after RAGT.
CONCLUSION:
We have identified two determinants –the severity of disability and the number of therapeutic units –which could have a decisive and predictive character in setting rehabilitation/designing programmes. The duration of the applied RAGT period, frequency and intensity could be a crucial factor for the potential of improvement in children with BS-CP.
Introduction
Cerebral palsy (CP) is the most common neurodevelopmental disorder and it is considered to be the most frequent cause of physical disability in childhood. The consequences of CP often limit an individual’s activity and participation in society. The motor disorder can often be accompanied by disturbances of perception, communication, behaviour, cognition, by epilepsy and by secondary musculoskeletal abnormalities (Rosenbaum, 2007).
Population-based studies from around the world report that the prevalence estimates of CP range from 1.5 to more than 4 per 1,000 live births (Odding, 2006; Oskoui, 2013; Novak, 2017; Stavsky, 2017).
A comprehensive and multidisciplinary approach is required in the care of children with CP. Early rehabilitation is very important; its basic element is a therapeutic physical education/kinesiotherapy. Therapy is not intended to cure or achieve a normal state. The real goal of the therapy is to improve the functionality and skills and maintain health in terms of locomotor, cognitive development, social integration and independence. Currently, there is an increased emphasis on an active approach in the therapy, including intensive, repetitive, and task-specific training to enhance neuroplasticity (Hsu, 2019; Das & Ganesh, 2019).
In the last 15 years, there has been a noticeable increase in the use of robot-assisted rehabilitation, particularly in patients after stroke, cerebrospinal trauma and, last but not least, in children with cerebral palsy. The neurophysiological background of RAGT is based on the spinal automatism (central pattern generators), plasticity of the central nervous system and motor learning (Wiart, 2016). In addition to the improvement of locomotor functions, positive effects of training on postural adaptation, cardiovascular function, muscle metabolism, intestinal motility, tissue trophicity, and overall improvement in quality of life are apparent (Riener, 2006; Shackleton, 2019). Recent systematic reviews and meta-analyses evaluating the effectiveness of RAGT in children, adolescents and young adults with CP have documented the effectiveness of robot-assisted training primarily in standing ability, balance control in gait, walking speed and distance, walking endurance and improvement of gross motor functions (Carvalho, 2017; Bayon, 2016; Lefmann, 2017; Wallard, 2017). RAGT is a promising tool that allows prolonged, controlled, intensive, task-specific training that is goal-directed and cognitively engaging with the high repetition of steps. These aspects promote a reproducible and kinematically consistent, symmetric, physiological-like movement of limbs (gait pattern) able to enhance motor learning and neuroplasticity.
The optimal intensity of the therapy in patients with CP has been frequently discussed in studies. If the therapeutic goal is to improve gross motor functions, increasing the frequency of physical therapy and kinesiotherapy may be beneficial. Given the time and effort that patients with CP and their families invest in motor skills training and prevention of secondary complications, it is important to know whether more frequent rehabilitation really represents a potentiating success aspect in achieving motor improvement (Novak, 2012).
There are a multitude of patient-specific factors that could affect the responsiveness to robot-assisted gait training in children with central movement disorders (Schroeder, 2014b). Age and severity of motor impairment are the most obvious variables, as natural psychomotor development is known to slow down significantly within the first decade of life, and gross motor ability is known to deteriorate in the second decade of life in more severely impaired children (e.g. children with CP classified as GMFCS levels III, IV and V) (Hanna, 2009). Gender could influence the responsiveness to task-specific therapies, as anthropometric measures in children with CP are known to be gender-dependent (e.g. CP –adapted growth charts) (Brooks, 2011).
The identification of patient-specific factors potentially allowing the prediction of the extent of RAGT effect could help in establishing indication criteria and therapeutic objectives in daily clinical practice. The standardised evaluation of observed parameters in exactly defined and unified therapy allows to assess the relationship between patient-specific factors and the change in motor functions after RAGT.
In paediatric neurorehabilitation, the GMFM is currently a widely accepted, reliable and frequently used tool for assessing gross motor functions in patients with CP (Russel, 1989, 2010; Sulivan, 2009; Alotaibi, 2014). In most studies, dimensions D (standing), E (walking, running and jumping) of GMFM and spatiotemporal and kinematic gait parameters have been used to objectify the effect of RAGT on motor functions (Bayon, 2016; Carvalho, 2017; Lefmann, 2017; Wallard, 2017). In patients enrolled into a pilot study published in domestic journals, after the completion of a series of 20 therapeutic units of RAGT in the intensive regimen (3–5 times a week) we also observed the stabilisation of trunk muscles, which also led to an improvement in sitting, crawling and rolling. Therefore, we decided to test all GMFM-88 dimensions (A, B, C, D, E) and GMFM-88 total score in each patient.
The aim of the presented observational study was to assess the effect of RAGT on gross motor functions in patients with bilateral spastic cerebral palsy and to evaluate patient-specific factors potentially influencing the response(s) to robot-assisted gait training in these patients.
Materials and methods
Experimental design
The study was conducted as a single-centre prospective observational long-term study in an out-patient rehabilitation healthcare facility in Slovakia from September 2009 to August 2018. Of the 107 patients examined, 97 paediatric, adolescent and adult patients with bilateral spastic CP were enrolled in the study; they underwent 1–4 blocks of RAGT, representing 16–82 TUs of RAGT. We evaluated the change in motor functions after the therapy in relation to the severity of disability, age, gender and number of therapeutic units. We examined whether any of these variables could significantly affect the resulting improvement and whether it would be necessary to match these variables in future prospective controlled studies related to RAGT. The flowchart of the study is given as Fig. 1.
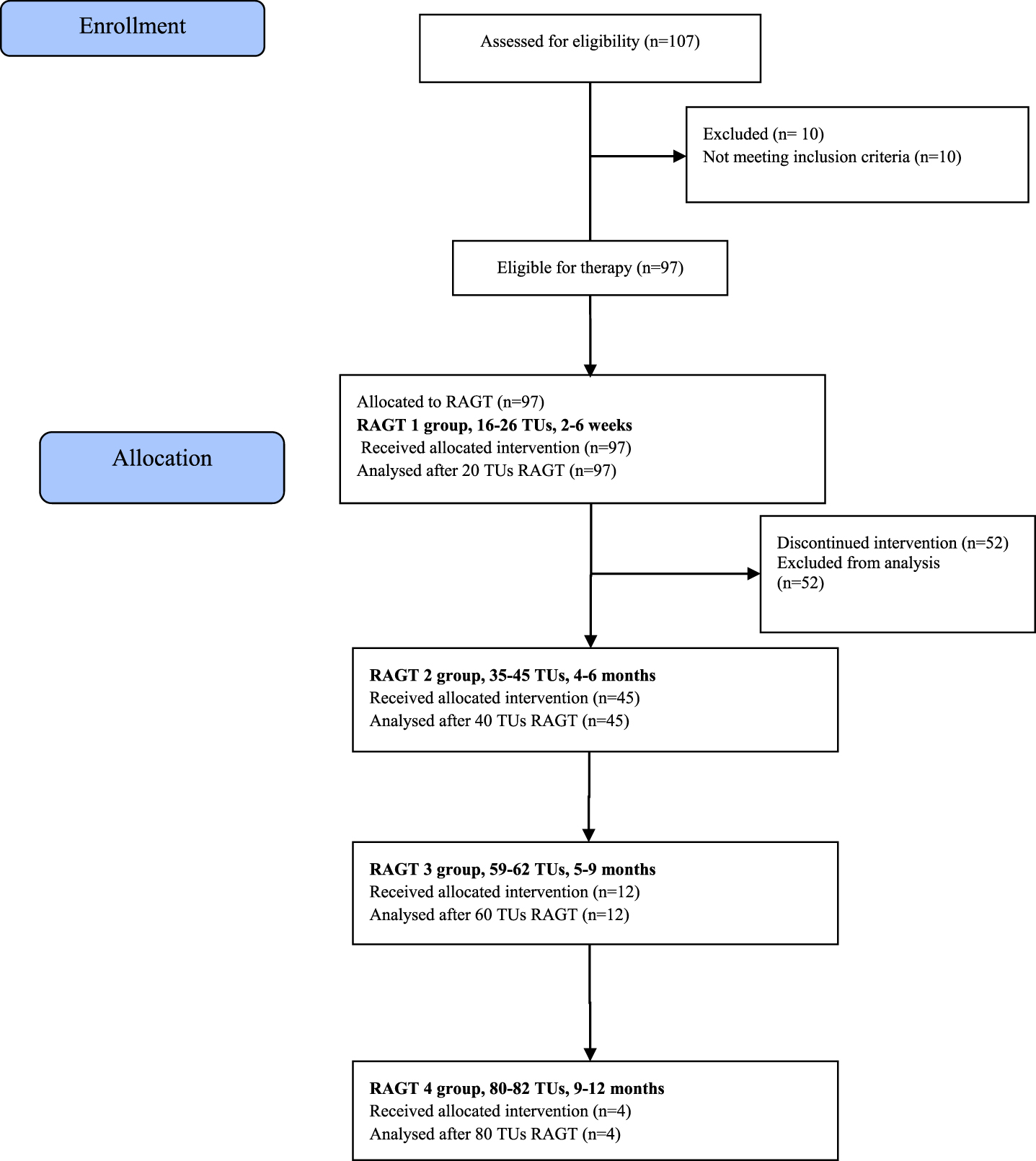
Flow diagram of the study.
This observational cohort study is reported in adherence to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) (See https://www.strobe-statement.org/fileadmin/Strobe/uploads/checklists/STROBE_checklist_v4_cohort.pdf).
All subjects –patients, parents or legal representatives of patients were informed about the course and conditions related to the applied therapy, as well as about the use of test results for research purposes, and they gave the informed consent before inclusion. This study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice (GCP) and was approved by the local ethics committee.
Therapy device
The robot-assisted gait training was performed using the Lokomat® system (Hocoma Inc., Volketswil, Switzerland), which we classify as exoskeletons. Exoskeletons are devices that operate mechanically and simultaneously on the human body. They generally use a set of cuffs connected to the patient’s lower limbs (Swinnen, 2020). A detailed description of the device was published, inter alia, in our previous randomised controlled trial (Klobucká, 2020).
Therapeutic interventions
Patients from the study group underwent 16–82 therapeutic units of the robot-assisted locomotor therapy in one to four therapeutic blocks during one year. During this period, the robot-assisted locomotor therapy using the Lokomat® system was the basic (main) therapeutic intervention in these patients. No other kinesiotherapy was scheduled. Patients in this group had no previous experience with RAGT. We determined the therapy duration and frequency of particular therapeutic units based on existing experience and knowledge from foreign studies and recommendations (Meyer-Heim, 2007, 2009; Borggraefe, 2008) and we have also taken into account individual possibilities of patients and their parents. As available data from published studies indicate the persistence of achieved improvement after RAGT for 2–6 months in patients with CP (Meyer-Heim, 2007; Borggraefe, 2010b; Patritti, 2011; Schroeder, 2014a; Bayon, 2016; Peri, 2017; Klobucká, 2020), the interval between individual therapeutic blocks was set to 2–4 months. One therapeutic unit lasted 30 minutes. Walking speed ranged from 1.2 km/h (in more severely affected patients) to 1.8 km/h (in mildly affected patients). The body weight support and guidance force were individually adjusted according to clinical judgement and the patient’s abilities in order to maximise the intensity of the training and to keep the motivation during each session (Klobucká, 2020). The therapist provided verbal enhancement to step actively and to raise the patient’s awareness to correct gait patterns and posture during the therapeutic unit.
Active patient participation was additionally achieved by changing the walking speed, body weight support or guidance force of the exoskeleton. Patients trained in the virtual reality-based environment.
Prior to the robot-assisted locomotor therapy and between particular therapeutic blocks, patients from the experimental group (RAGT) underwent a conventional rehabilitation (most commonly a neurodevelopmental treatment NDT –Bobath concept, Vojta's method of reflex locomotion, ergotherapy, physical therapy –magnet therapy, bio laser phototherapy, and some patients also underwent complementary methods of therapeutic rehabilitation –synergetic reflex therapy, hippotherapy, ball training, circular training, TheraSuit, hydrotherapy, acupuncture, etc.) in various combinations and at different frequencies (most commonly 1–2 times a week) depending on the type and options of the healthcare facility they visited.
One therapeutic unit of conventional kinesiotherapy, in which patients continued between individual RAGT blocks, lasted for 30–45 minutes, representing the usual care from their local physical therapist in Slovakia.
Both RAGT and conventional therapy were delivered by trained physical therapists specialised in the management of patients with cerebral palsy.
Evaluations
All evaluations were performed within 24 hours prior to the first therapeutic block (V0) and within 24 hours after each subsequent therapeutic unit (V1–V4).
Prior to therapy, patients were routinely examined by a rehabilitation doctor in the out-patient setting. All patients were classified at admittance according to the Gross Motor Function Classification System (GMFCS) (Palisano, 1997).
Subsequently, patients were tested using the Gross Motor Function Measure (GMFM). There are 2 versions of GMFM; the 88-item version (GMFM-88) and the abbreviated 66-item version (GMFM-66). To evaluate patients' motor functions in this study, we used the more detailed 88-item version which evaluates patient's motor functions in the following five dimensions:
Assessments were performed by trained certified physical therapists.
Walking time (min), walking distance during one therapeutic unit (m) and average walking speed (km/h) during each training were evaluated by the Lokomat® system.
Statistical analysis
To process obtained data, we used descriptive statistics, non-parametric statistics, effect size, and correlation and regression analysis. We processed data using MS Office Excel and SPSS 21.0 for Windows. Data are presented as means plus minus standard deviations or medians and interquartile ranges (IQR). The normality of our data sets was tested using Kolmogorov-Smirnov normality test. Since the normal data distribution was not maintained across all data sets, the non-parametric Wilcoxon test for paired values was used to compare the input and output GMFM values in each group.
Using the Pearson χ2 test for categorical variables and Mann-Whitney U test of two independent data sets, we compared the improvement rate, severity of disability, gender and age between groups of patients who already discontinued the therapy after the first therapeutic block and those who decided to continue in the therapy. The results are considered statistically significant at p < 0.05 and highly statistically significant at p < 0.001.
To determine the substantive significance of the differences in input and output GMFM-88 values, we used the calculation of the Cohen’s effect size (d) using the pooled standard deviation. According to the concept of Cohen (1977) and Sawilowski (2009), the coefficient d = 0.01–0.2 was interpreted as a very small effect size, d = 0.2–0.5 as a small effect size, and d = 0.5–0.8 as a medium-sized effect causing the difference. The values d = 0.8–1.2 represent a large effect size and d > 1.2 a very large effect size. The calculation of mean improvements and the Cohen’s coefficient d were completed by calculating 95%confidence interval (CI 95%).
When assessing the clinical significance of the change in the GMFM-88 score, we used the results of the Wang and Yang (2006) and Storm (2020) studies. Wang and Yang (2006) divided the improvement in motor functions in patients with CP into three categories: “no improvement”, “moderate improvement” (achieved partial progress in motor functions), “high improvement” (achieved or almost achieved expected improvement in motor functions). In their study related to the sensitivity of GMFM-88, Wang and Yang (2006) stated that an improvement of≥1.29%in GMFM-88 can be considered clinically detectable, and a score increase by≥3.99%is considered as a major improvement. According to study of Storm et al. (2020), the Minimal Clinically Important Difference (MCID) values ranged between 0.1%–3.0%for GMFM-88 total score for the CP population. For GMFM dimension “D”, MCID values range was 0.8–5.2%and for dimension “E” between 0.3–4.9%.
The Spearman’s test, which examines the dependence of the order, was used to correlate the data. The result of the test is a correlation coefficient (rho), the values of which are within the interval (–1, 1). The correlation values < 0 indicate a negative linear dependence. The correlation values > 0 indicate a positive linear dependence. The values of the correlation coefficient 0.8–1 (–0.8 to –1) are considered to be particularly strong, i.e. there is a very strong interdependence between the variables. The values of 0.4–0.8 (–0.4 to –0.8) are moderately strong and the values 0–0.4 (–0.4 to 0) are considered to be weak. The determining criterion in evaluating the correlation is a statistical significance. The lower the significance value than 0.05, the more we can be sure of the effect strength. The following values are used to evaluate the significance: 0.05; 0.01; 0.001 and 0.0001.
To assess/determine the relative significance and effect of the observed independent variables (age, gender, number of TUs, severity of disability) on the observed dependent variable (improvement in gross motor functions), we added the recalculation by ANOVA multiple linear regression analysis. The result of the test is a standardised regression coefficient β, supplemented by the statistical significance. A standardised β coefficient compares the strength of the effect of each individual independent variable to the dependent variable. The higher the absolute value of the beta coefficient, the stronger the effect.
Results
97 patients (58 males and 39 females) with bilateral spastic CP aged 3.7–27 years (mean age 10.02 (SD±5.29), median 8.9)) underwent 1–4 blocks of RAGT over one year, representing 16–82 therapeutic units (mean number 34.06 (SD±16.41)) of robot-assisted locomotor therapy using the Lokomat® system. In one block, patients completed an average of 20.14 (SD±1.23) therapeutic units over two to six weeks with a frequency of three to ten times per week. The interval between the individual blocks was 2–4 months. The severity of disability was determined by GMFCS (Gross Motor Function Classification Scale) (Palisano, 1997). Patients with GMFCS level I, II (n = 30) were evaluated as mildly affected. Patients with GMFCS level III, IV were evaluated as more severely affected (n = 67). The mean GMFCS was 2.84 (SD±0.79). Baseline data of all the recruited patients are summarised in Table 1 and 2.
Demographical and clinical features of the patients
Demographical and clinical features of the patients
Distribution of patients according to the number of completed therapeutic units and therapeutic blocks of RAGT (1–4)
Of the 97 patients who completed the first RAGT therapeutic block, only 45 patients continued in other therapeutic blocks according to a predetermined study design. We then divided them into subgroups according to the number of completed therapeutic units (Table 2). 52 patients did not continue in the therapy according to the defined protocol for various reasons. There were no significant differences between the groups in age (p = 0.786, Z = –0.271), gender (p = 0.969) and severity of motor impairment (p = 0.422, Z = –0.802) (Table 2).
The following values are presented as mean±SD (min–max). The mean duration of one therapeutic unit (TU) was 30.01 min per patient (SD±4.29, ranging from 20.39 to 39.36) and the mean distance that patients walked during one therapeutic unit was 663.63 m (SD±152.39, ranging from 159 to 975). The average speed was 1.39 km/h (SD±0.18, ranging from 1.2 to 1.8). The intervention was well tolerated with no adverse events, except for minor issues such as small leg abrasions.
After the completion of 1–4 blocks of RAGT, evaluated baseline parameters have improved as follows (Table 3).
Change in dimensions A, B, C, D, E and the total score of GMFM-88 (Gross Motor Function Measure) after 1–4 blocks of robot-assisted gait training (RAGT)
Change in dimensions A, B, C, D, E and the total score of GMFM-88 (Gross Motor Function Measure) after 1–4 blocks of robot-assisted gait training (RAGT)
Values are presented as mean±SD, median (IQR, 25th; 75th percentiles). V0 - evaluation before therapy (baseline). V1 - visit 1 (post- intervention, after 1st block RAGT). V2 - visit 2 (post- intervention, after 2nd block RAGT). V3 - visit 3 (post- intervention, after 3rd block RAGT). V4 - visit 4 (post- intervention, after 4th block RAGT). GMFM - Gross Motor Function Measure. d - Cohen’s effect size, rate of substantive significance of differences: d = 0.2–0.5 (a small difference) d = 0.50–0.80 (a medium-sized difference), d = 0.80–1.2 (a large difference), d > 1.2 (a very large difference). p - statistical significance level; significant at p < 0.05. Z - value of the test criterion (statistical calculation) using the Wilcoxon test. CI 95%- confidence interval.
After completing the first block of RAGT (16–26 TUs over two to six weeks), we observed clinically meaningful and statistically significant improvements in GMFM-assessed motor functions in all dimensions of the test. The improvement in motor functions represented a medium effect size in dimension A and a small effect size in dimensions B, C, D, E and total GMFM.
After completing two blocks of RAGT (35–45 TUs over four to six months), we observed clinically meaningful and statistically significant improvements in GMFM-assessed motor functions in all dimensions of the test. The improvement in motor functions represented a large effect size in dimension A, a medium effect size in dimension B, C, total GMFM and a small effect size in dimensions D, E.
After completing three blocks of RAGT (59–62 TUs over five to nine months), we observed clinically meaningful and statistically significant improvements in GMFM-assessed motor functions in all dimensions of the test. The improvement in motor functions represented a very large ES in dimensions C and total GMFM, a large ES in dimensions A, B, D and a medium effect size in dimension E.
After completing four blocks of RAGT (80–82 TUs over nine to twelve months), we observed clinically meaningful improvements in motor functions in all GMFM dimensions.
The improvement in motor functions represented a very large effect size in dimensions B, C, D and total GMFM and a large ES in GMFM dimensions A and E. Considering the small number of patients in the group RAGT 4, the statistical significance of the improvement was not evaluated.
To evaluate the correlation between age, gender, severity of disability, number of therapeutic units and observed parameters evaluating patient’s motor function (improvement in motor functions), we used Spearman’s correlation coefficient.
We supplemented the correlation analysis by ANOVA multiple linear regression, which allowed us to assess the relative importance and effect of predictors (patient-specific factors) on the observed dependent variable (improvement in gross motor functions).
The correlation analysis did not demonstrate a statistically significant dependence of the improvement in GMFM-assessed motor functions on age. Thus, the patients of all age categories have improved similarly.
We also did not observe a correlation between the improvement and the gender in any of the GMFM dimensions.
We observed a statistically significant dependence of the improvement rate in GMFM dimensions A, B, D and E on the severity of disability at the level of significance p < 0.05.
More severely affected patients have improved more markedly in dimensions A and B (statistically significant positive correlation, p < 0.01).
Mildly affected patients have improved more markedly in dimensions D and E (statistically significant negative correlation, p < 0.05).
Using the analysis of the dependence of motor improvement on the number of TUs,
we have documented statistically significant dependence of the improvement rate in all GMFM dimensions on the number of completed TUs (statistically significant positive correlation, p < 0.05).
It follows from the above that patients who completed a higher number of TUs have improved more markedly.
Using ANOVA regression analysis, we did not confirm the effect of age or gender on the observed parameters of GMFM-assessed motor functions. According to the data obtained, the number of therapeutic units (for all GMFM dimensions) and the severity of disability (for GMFM dimensions A, B and E) are the most important predictors for improving motor functions in patients with BS-CP in our cohort (Table 4).
Correlation and regression analysis of the dependence of motor improvement on age, gender, severity of disability and number of therapeutic units
Correlation and regression analysis of the dependence of motor improvement on age, gender, severity of disability and number of therapeutic units
rho –Spearman’s correlation coefficient. p - statistical significance level; significant at p < 0.05. ** The correlation coefficient is significant at the level of 0.01 (2-way). *The correlation coefficient is significant at the level of 0.05 (2-way). β –standardised regression coefficient.
There is evidence that gait rehabilitation robots have beneficial effects on the rehabilitation of children with cerebral palsy (Carvalho, 2017; Swinnen, 2020). Robot-assisted therapies –in contrast to most therapeutic interventions in CP –allow an objective quantification of treatment intensity and outcome (Schroeder, 2014a). Functional gait training results in clinically important benefits for children and young adults with CP, with a therapeutic goal of improved walking speed. Meta-analysis suggests that the gait training results in a larger positive effect than standard physical therapy (Booth, 2018). But there are still many questions that remain unanswered. Such as, what kind of children would benefit the most? What is the optimal training dose? Currently, there is no widely accepted consensus for application of RAGT in patients with CP. We recommend to determine the duration, intensity and frequency of the therapy according to the expert judgement, experience, knowledge from foreign studies with regard to the individual possibilities of the patient and his/her parents.
The aim of this study was to assess the effect of RAGT on gross motor functions in patients with BS-CP and to identify patient-specific factors that could affect the patient’s response/responsiveness to this therapy.
The observational study presented by us demonstrated a significant improvement (p < 0.001) in motor functions evaluated by the GMFM-88 in all patients with BS-CP in the study cohort after RAGT. The effect of the therapeutic intervention on gross motor functions was comparable to the results of studies reported to date (Carvalho, 2017). According to the reference data for the minimum clinically important differences in gross motor functions evaluated by GMFM-88 and GMFM-66 (MCIDs, Wang and Yang, 2006; Offringer, 2008; Storm, 2020), the improvement in our study was clinically significant, emphasising the effectiveness and justification for the use of task-specific locomotor therapies in patients with CP.
Improvement in motor functions after RAGT, intensity, frequency of therapy
In our study, we recorded a statistically significant improvement in all evaluated dimensions (p < 0.001) –GMFM A, B, C, D, E and total GMFM-88 –after the completion of RAGT using the Lokomat® system. In agreement with other authors, we documented this improvement in our previous studies in which we also confirmed an increase in walking speed and endurance after RAGT (Meyer-Heim, 2007, 2009; Patritti, 2009; Borggraefe, 2010a; Klobucká, 2013a, 2014, 2020). Patients in our current/most recent study, who continued in therapy after the first therapeutic block, continued to experience statistically significant improvement, which was accompanied by an increase in the effect size for gross motor improvements (medium to very large ES).
We have confirmed this fact to some extent in the previous study comparing the improvement of motor functions after 20 TUs and 40 TUs. Patients who completed 40 TUs have improved more markedly compared to patients who underwent 20 TUs (Klobucká, 2013b).
However, to date there is no generally valid recommendation regarding the duration and intensity of training for the application of locomotor therapy using electronically controlled orthoses with body weight support in children with gait disorder.
Clinical studies evaluating the change in gross motor functions after assisted gait training with respect to the age, impairment and diagnosis have shown relevant differences in treatment protocols and outcome measures, making it difficult to compare these studies (Bayon, 2016; Lefmann, 2017; Carvalho, 2017; Booth, 2019). Currently, in the rehabilitation of children with CP, an intensive targeted therapy is preferred over less intensive programmes (Carvalho, 2017; Hsu, 2019).
The results of studies of foreign authors, including controlled clinical trials, have suggested that the total number of therapeutic units of intervention programmes is more important than their number per week (Dodd, 2007; Borggraefe, 2008; Hsu, 2019). In their pragmatic, randomised, crossover trial on RAGT in children with CP, Ammann-Reiffer et al. (2020) did not confirm a statistically significant improvement in ambulatory patients with BS-CP in dimensions D, E, 6 minute walk test and 10 metre walk test. According to their conclusions, 15 sessions of RAGT within five weeks are not effective in improving walking abilities in ambulatory children with CP.
However, Peri et al. (2017) adopted 40 therapy (RAGT) sessions within ten weeks in their groups with significant and clinically meaningful improvements, while their group with a mixed protocol of 20 RAGT and 20 physiotherapy sessions over four weeks did not improve. The duration of the applied RAGT period could be a crucial factor for the potential of improvement in these children.
In our research, we pointed out the fact that the number of therapeutic units at a sufficient frequency can be a significant determinant influencing the final effect of the therapeutic intervention. By correlation and regression analysis, we confirmed a positive linear dependence between the improvement in gross motor functions and the number of RAGT therapeutic units in the group of children, adolescents and young adults with BS-CP. Compared to studies by foreign authors (Carvalho, 2017; Ammann-Reiffer, 2020), the frequency and intensity of training in our study was relatively high (1 therapeutic block with a frequency of 3–10 times a week over 2–6 weeks), and one therapeutic unit lasted for 30 minutes. A positive correlation between the improvement in the GMFM dimension E, distance and walking time during the therapeutic unit could also suggest a dose-dependent effect of the therapeutic intervention on functional gait parameters (Borggraefe, 2010a).
Most patients with CP undergo rehabilitation 1–2 times a week, but the frequency of therapy varies from less than 2 times a month to more than 3 times a week (Palisano, 2012; Park, 2018). However, if the therapeutic goal is to improve gross motor functions, increasing the frequency of physical therapy/kinesiotherapy may be beneficial. In most studies, the intensive rehabilitation/therapeutic regimen (with a frequency of 3–11 times a week) with a therapeutic unit duration of 30–60 min led to a significant improvement in the endpoints (Størvold, 2018; Park 2018; Hsu, 2019).
In their review study, Hsu et al. (2019) evaluated the frequency and intensity of therapeutic interventions in patients with CP. They unequivocally confirmed that intensive training (more than 3 times a week) improves the observed motor parameters in patients with CP. At the same time, they pointed out the fact that in conventional methodologies (among others, also NDT), the improvement in motor functions was recorded with increasing number of daily hours, while in interventional methodologies (among others, also treadmill training), the improvement was recorded only with a longer training period. In specific structured, goal-oriented intervention therapies, the overall duration of the rehabilitation programme has a significantly more pronounced effect on the motor improvement (Hsu, 2019).
However, Schroeder et al. (2014a) drew attention to the “ceiling-effect” in improving motor functions in individual patients when performing repeated series of robot-assisted gait training. In their protocol, one block of RAGT included 12 therapeutic units over 3 weeks. Of the group of 18 patients aged 5–21.8 years (GMFCS I–IV, average 2.33), 12 patients underwent 2–5 blocks of RAGT with undefined intervals between blocks, while for 6 patients it was the first and the last experience with RAGT within the therapy. They found a significant negative correlation between GMFM 66 score improvement and the number of robot-assisted treadmill training blocks in their study population (patients who completed more blocks did not improve more markedly). In contrast to the patients from the study of Schroeder et al. (2014a), the patients in our current study were more severely affected (97 patients, GMFCS I–IV, average 2.84); we evaluated all dimensions A, B, C, D, E and the total score of the GMFM-88, all our patients experienced RAGT for the first time in the current study, and they completed a higher number of therapeutic units in one therapeutic block (average 20.14 (±1.230)) with a standardised time interval between individual subsequent therapeutic blocks. In his systematic review, Hsu (2019) reported that GMFM scores exhibited greater improvement in intensive therapeutic programmes than in non-intensive programmes and with intermittent therapeutic schedules than in continuous schedules.
Correlation analysis –relationship of age, gender and severity of disability
This study focused primarily on the identification and assessment of patient-specific determinants that could affect the resulting improvement in motor functions in patients with BS-CP after RAGT.
The severity of disability (GMFCS level) can be one of the determinants.
In accordance with the findings in the review study of Carvalho et al. (2017), in the current study we also confirmed a significant negative linear dependence in the evaluation of the relationship between the severity of disability and the motor improvement in the GMFM dimensions D (standing) and E (walking). Thus, mildly affected patients (GMFCS I, II) improved more markedly in these specific dimensions. At the same time, we confirmed a significant positive linear dependence in the evaluation of the relationship between the motor improvement in the GMFM dimensions A (lying, rolling) and B (sitting) and the severity of GMFCS-determined disability, indicating that more severely affected patients improved more markedly in GMFM dimensions A and B (GMFM III, IV). The regression analysis supported these findings and pointed out that the severity of disability is a crucial factor predicting the improvement rate, especially in GMFM dimensions A, B, and E. We came to similar conclusions in our study from 2013 (Klobucká, 2013a), which also confirmed a statistically insignificant trend towards higher improvement –total GMFM-88 in more severely affected patients (GMFCS level III, IV), corresponding to conclusions of the systematic review, which pointed to higher effectiveness of treadmill training in children with motor functions classified as GMFCS level III, IV, compared to those who were classified as GMFCS level I, II at baseline (Willoughby, 2009). In contrast to these findings, Schroeder et al. (2014b) confirmed a negative correlation of improvement in motor functions (GMFM-66 total score) with increasing GMFCS score. According to their results, the baseline total GMFM-66 score appears to be an important predictive factor. The linear dependence in the study of Schroeder et al. (2014b) implies that patients with CP (various forms in their study, aged 4–18) with a higher baseline GMFM-66 score (mildly affected) will achieve a more significant improvement in gross motor skills after RAGT than patients with a lower baseline score (more severely affected with lower gross motor skills).
In our opinion, this discrepancy in the resulting findings of the above-mentioned studies reflects the heterogeneity of analysed studies and the use of different evaluation criteria.
We hypothesised that the age could be another determinant that could potentially affect the magnitude of the therapeutic effect of RAGT.
In our previous studies, we also assessed the influence of age and severity of disability on the improvement of motor functions (Klobucká, 2014). We demonstrated a statistically significant improvement in motor functions evaluated using GMFM-88 in 78 children, adolescents and young adults with CP (GMFCS I–IV) after completing 20 TUs of RAGT. In the group of mildly affected patients (GMFCS I, II), we observed a statistically insignificant trend towards higher improvement in younger patients (up to 11 years old). However, in the group of more severely affected patients (GMFCS III, IV), a trend towards higher improvement was observed in patients older than 11 years (Klobucká, 2014).
In their prospective, controlled cohort study focusing on the effect of robot-enhanced repetitive treadmill therapy on gross motor function, activity and participation in patients with bilateral spastic cerebral palsy (BS-CP), Schroeder et al. (2014a) also observed an insignificant negative correlation between GMFM-66 score improvement and age. They observed more than a twofold but statistically insignificant improvement in gross motor functions in the GMFM-66 score in younger patients up to 10 years of age compared to older patients (GMFCS I–IV, average 2.3) (Schroeder, 2014a). The group of older children was at an age when –according to the reference curves –the natural motor development was no longer expected (Hanna, 2008). Nevertheless, the improvement in their GMFM-66 scores still represented a large effect size in MCID (Minimal Clinically Important Difference change) change (Schroeder, 2014a). This supports the hypothesis that RAGT may provide benefits even after reaching the maximum predicted motor development in patients with CP. In our controlled randomised prospective bicentric study (2020), we investigated this interesting fact in greater depth and more specifically, and we evaluated the effect of RAGT on adolescents and adults with CP. By comparing the mean improvement in motor functions evaluated by all five dimensions of GMFM-88 after 20 therapeutic units in two treatment groups, we observed a significantly greater improvement in the experimental RAGT group consisting of patients who underwent the therapy in the intensive regimen, compared to the control group consisting of patients who underwent the conventional training. Furthermore, such improvement has persisted after 3–4 months (Klobucká, 2020).
Even in the current observational study, we did not demonstrate a significant linear dependence using correlation and regression analysis, indicating a relationship between age and motor improvement as assessed by the GMFM-88, which supports the findings of our previous studies. Thus, children, adolescents and adults with BS-CP improved after intensive RAGT. Similar conclusions were reached by Schroeder et al. (2014a, b) who, despite the trend in favour of younger children, did not show a significant effect of the age on the improvement in GMFM-66 total score.
In the evaluated results, we cannot rule out the influence of the natural continuation of the development of gross motor functions. Hanna et al. (2008, 2009) and Rosenbaum (2002) processed reference curves of motor development in individuals with CP based on the longitudinal observation in various age categories and different degrees of disability. They evaluated motor functions using the GMFM-66 test. According to these curves, maximal motor function can be expected to be reached in children with CP aged 5–10 years, depending on the severity of disability. At the same time, however, there is evidence that children and adolescents with CP do not show significant changes in motor functions as assessed by GMFM without therapeutic intervention during the 3–6-week follow-up period (Knox, 2002; Cherng, 2007; Hanna, 2008; Novak, 2013; Carvalho, 2017; Booth, 2018). In their study, Park et al. (2017) assessed gross motor functions in patients with bilateral spastic CP aged 3–18 years during a year-long NDT therapy with a frequency of 2–3 times a week. The reduction in spasticity was observed in patients, however no statistically significant change in motor function was recorded.
We also do not expect a significant effect of conventional therapy performed with a frequency of 1–2 times a week between individual therapeutic blocks on the motor improvement in the patient group. It has been confirmed that significant changes occur only at a higher frequency and in intensive regimen (Park, 2018).
Strengths and limitations of the study
Our latest study summarises many years of research on the effect of RAGT on motor functions in patients with BS-CP. The study patient group was heterogeneous in terms of age and degree of disability (3.7–27 years, GMFCS I–IV). It basically reflected the standard population of a neurorehabilitation clinic. After intensive robot-assisted treadmill training using Lokomat®, we recorded an objective improvement in motor functions in mildly, as well as severely affected patients with bilateral spastic CP.
Patients of all age categories improved with a statistically insignificant trend towards higher improvement in younger patients; however, also the improvement in the group of adolescents and adults with CP was statistically significant and clinically meaningful.
In the study, motor functions were assessed using all GMFM-88 items before and after each treatment block over 12 months. To the best of our knowledge, there is no similar study that would continuously evaluate gross motor functions during the year-long RAGT.
It should be noted that our study has some limitations. Firstly, it is not a randomised, placebo-controlled study. However, in a previously published randomised controlled bicentric study from 2020, we have already demonstrated a clinically meaningful and statistically significant effect of RAGT in adolescents and adults with CP compared to the conventional therapy (Klobucká, 2020).
One limitation of our study may also be the non-blinded assessment of the outcome. However, since this is an observational study and the assessors were not informed of the underlying hypothesis regarding potential patient-specific determinants influencing the effect of therapeutic intervention, this criterion can be considered as irrelevant.
The issue of identifying potential determinants affecting the size of RAGT therapeutic effect requires a sample of appropriate size, standardised therapy, and uniform evaluation. These criteria are met in the study, although only a small number of patients have completed the third and fourth block of RAGT (59–82 TUs) respecting predetermined therapeutic protocol criteria (with standardised time intervals between blocks). The small sizes of groups RAGT 3 and 4 reduce the statistical power. One of the reasons for the smaller number of patients in groups RAGT 3 and 4 was also the fact that some patients achieved a significant improvement after 20 or 40 TUs and decided not to continue in RAGT, or they came to the next therapy with a longer time interval. Despite a consistent effort to standardise therapeutic intervention, we adapted to some extent to the individual capabilities of patients and their parents in terms of the number of therapeutic units in individual blocks, who often arrived for therapy from distant places, as we are the only rehabilitation facility in Slovakia that offers robot-assisted gait training in children with CP. Thus, the number of TUs is not the same in individual blocks, but there is no statistically significant difference between individual blocks (patients completed an average of 20.14 (±1.230) TUs in one block).
The GMFM is considered the gold standard for the evaluation of gross motor functions in children with CP (Ammann-Reiffer, 2020). In contrast to other outcome measures, responsiveness and MCID have been determined for GMFM score changes in prospective longitudinal studies and a direct relationship to GMFCS levels is possible (Oeffinger, 2008; Storm, 2020). Both versions –GMFM-88 and GMFM-66 –are validated tools and represent two of the most frequently used tools for assessment of functional motor ability in children with CP (Alotaibi in Hsu, 2019). Most studies now use the shorter GMFM-66 version of the test more due to the reported better psychometric properties (Russel, 2010). Since the pilot phase of our study started already in 2008, we started testing with the more extensive 88-item version of the GMFM. To maintain data homogeneity and to seek more detailed monitoring of motor functions in all dimensions, we continued to use this version throughout the study.
Conclusion
This study aimed at identifying potential relevant patient-specific factors that could predict the effectiveness of RAGT on motor functions in patients with BS-CP. The data presented in this study confirm heterogeneity as well as some uniformity in responses to RAGT in children, adolescents and young adult patients with BS-CP. We did not confirm the significant association between gender, age and improvement in gross motor functions tested by GMFM. We have identified two determinants –the severity of disability and the number of therapeutic units –that could be determining and predictive in establishing/designing rehabilitation programmes. However, the prognostic value of these determinants will need to be verified in future studies with an appropriate design.
Not only the optimal responder, but also the optimal intensity of this intervention, as well as the effect of repetitive RAGT blocks will need to be determined more specifically in the future.
Footnotes
Acknowledgments
The authors would like to express their appreciation to all the subjects and their families for their co-operation and participation in this study. We thank the physiotherapy team of the Rehabilitation Centre Harmony for their assistance and cooperation.
We are grateful to Alojz Halas - director of the Rehabilitation Centre Harmony, for support and willingness to help in performing this study.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
This work was partly supported by the Framework Programme for Research and Technology Development, Project: Building of Centre of Excellency for Sudden Cerebral Vascular Events, Comenius University Faculty of Medicine in Bratislava (ITMS:26240120023), cofinanced by European Regional Development Fund.