
Abstract
BACKGROUND:
Pisa syndrome (PS) is a postural disorder characterised by lateral flexion of the spine (> 10°), predisposing the affected individuals to falls, and contributing to increased mortality in neurodegenerative diseases.
OBJECTIVE:
An overview of currently applied therapeutic management options, primarily focused on specifically structured rehabilitation exercises, in conjunction with falls-risk assessment in the individuals affected by PS.
METHODS:
A narrative literature review, augmented with the authors’ own experience in physical rehabilitation management.
RESULTS:
As individuals affected by PS are evidenced to be intrinsically exposed to higher falls-risk through acquired postural deformities, they often fall victims of traumatic accidents, occasionally also facing relocation into 24-hour nursing facilities due to the injuries sustained/resultant disability, consequently having overall quality of their life appreciably reduced.
CONCLUSIONS:s
A comprehensive approach is postulated in designing optimal therapeutic management, comprised of the exercises controlling postural stability, whilst reducing lower back pain, and the ones also promoting specific skills essential for coping unassisted after an accidental fall effectively. Rehabilitation of individuals affected by PS should be a fully integrated service, eliminating all identified risk factors for falls. As clinical PS symptoms tend to recur after completion of a full course of therapeutic management, all PS patients should continue the pursuit of therapeutic exercises on an individual basis, to effectively retard their recurrence. In view of overall scarcity of clinical studies completed on the large population samples of PS patients, further in-depth research is still required to ensure higher credence to overall efficacy of the presently proposed therapeutic solutions.
Background
While setting out to provide a comprehensive overview of currently applied therapeutic management options in treating Pisa syndrome (PS), the authors opted for a narrative review as by far the most suitable format for addressing certain deficits within the scope of research on the subject, as published to date.
A thorough search of medical databases revealed that not a single review of literature has tackled PS in terms of a diversity of rehabilitation issues, in conjunction with assessing attendant falls-risk, both construed as the essential components of effective therapeutic management.
This prompted the authors to address such an obvious deficit and put together a narrative review focused specifically on both issues, which also offered the added benefit of their own clinical experience, making it, in a manner of speaking, a pioneering effort in this particular domain.
PS was first described by Karl Axel Ekbom, a Swedish neurologist, in 1972, and initially treated as trunk dystonia or pleurothotonus resulting from the treatment with neuroleptics (Ekbom, Lindholm, & Ljungberg, 1972). PS is a postural deformity manifested by a lateral tilt of the trunk, accompanied by a characteristic bent of 10° or more (Doherty et al., 2011), generally acknowledged the most common diagnostic criterion. A milder form of this syndrome is diagnosed when the lateral tilt of the trunk is less than10°, and a severe one when in excess of this value (Broussolle et al., 2007). PS manifests itself as a series of involuntary muscle contractions causing the trunk to twist, which can be reduced by laying the patient down on his back (Dutta, 2020). It has been referenced in dementia with Lewy bodies, progressive supranuclear palsy, multiple system atrophy (MSA), Huntington’s disease, and Parkinson’s disease (PD) (Michel, Oscar, Correa, Alejandro,& Micheli, 2015). It impairs overall postural stability, adversely affects upper limb functionality, and exacerbates back pain (Alwardat et al., 2019). This postural impairment is deemed one of the most common complications causing disability in the individuals affected by Parkinson’s disease, as well as contributes to higher mortality rate (Doherty et al., 2011; Laudisio et al., 2017).
Pathophysiology of PS
Severity of postural impairments in neurodegenerative diseases varies, whereas overall postural instability is deemed a typical feature of PD. Propulsion (a tendency to fall forward), retropulsion (a tendency to fall backward), and lateropulsion (a tendency to fall) are the most common characteristics (Dobosiewicz, Kwiatkowski, Mietkowska, Marszalek, & Wendland, 2017). Lateral tilting of the entire body frame is characteristic of PS. In some cases, patients fail to notice how long it has been since they actually started experiencing the stooping phenomenon (Yokochi, 2006). Experience indicates that in the initial phase, the leaning is manifest while sitting. As PS develops, the tilt also becomes noticeable while standing and walking (Castrioto, Piscicelli, Pérennou, Krack, & Debû, 2014).
The lateral curvature of the spine in PS is significantly reduced when a patient assumes a supine position. This actually distinguishes this syndrome from scoliosis, in which the curvature is permanent, and the radiographically evidenced properties of vertebral rotation are encountered (Tinazzi et al., 2016). The highest incidence of this phenomenon is observed in the patients affected by MSA (Colosimo, 1998), in advanced Alzheimer’s disease (AD) (Davidson, Powchik, Davis, 1998; Vanacore et al., 2005), advanced parkinsonism, and among the individuals undergoing neuroleptic therapy (Patel, Tariot, & Hamill, 1991; Tassorelli et al., 2012).
These tend to be the older individuals who have long experienced the disease in its advanced stage (Barone, Santangelo, Amboni, Pellecchia, & Vitale, 2016). Studies indicate that elderly individuals who had previously been diagnosed with degenerative spine disease, osteoporosis or arthrosis, i.e. pathologies associated with the aging process, are exposed to a higher risk of PS (Fife et al., 2017). Its additional properties, as well as those differentiating it from the degenerative changes consist in the fact that PS symptoms are exacerbated during physical activity, and alleviated in the supine position. There are no mechanical restrictions on the spinal mobility associated with osteoarthritis, and there is a continuous electrical activity in the paraspinal muscles, in parallel to the direction in which the trunk tilts (Doherty et al., 2011).
A review of the available studies indicates that PS has been encountered in the patients with subdural haematoma, normotensive hydrocephalus, and subacutesclerosing panencephalitis. It may also occur as an idiopathic or isolated condition. The established risk factors are older age, longer disease duration, osteoporosis and/or arthrosis, female gender, and a sudden boosting in the dosage of antipsychotic medications (Cerri, Mus & Blandini, 2019). In the individuals affected by neurodegenerative diseases, incidence of PS may be caused by pharmacotherapy (Table 1) (Miletic, 2016; Barone, Santangelo, Amboni, Pellecchia, & Vitale, 2016).
Conditions associated with Pisa syndrome (according to Tinazzi, Geroin, Gandolfi, Smania, Tamburin, Morgante & Fasano, 2016)
Conditions associated with Pisa syndrome (according to Tinazzi, Geroin, Gandolfi, Smania, Tamburin, Morgante & Fasano, 2016)
PNS: Peripheral Nervous System, CNS: Central Nervous System.
The origin of PS is far from fully understood. Such factors as proprioceptive reflex disorders, myopathies, degenerative bone lesions, connective tissue pathologies, adverse effects of pharmacotherapy, and dysfunctions of extrapyramidal system manifesting as central muscle tone dysregulation, are therefore taken into account (Fig. 1). There are two hypotheses on the pathophysiology of PS, i.e. a central and a peripheral one. The central hypothesis is based on the assumption that PS appears as a consequence of disorders of the basal ganglia and neurotransmission in sensorimotor integration pathways, which may be exacerbated by dopaminergic treatment. The changes that may occur in the musculoskeletal system are consistent with the peripheral hypothesis (Dutta, 2020).
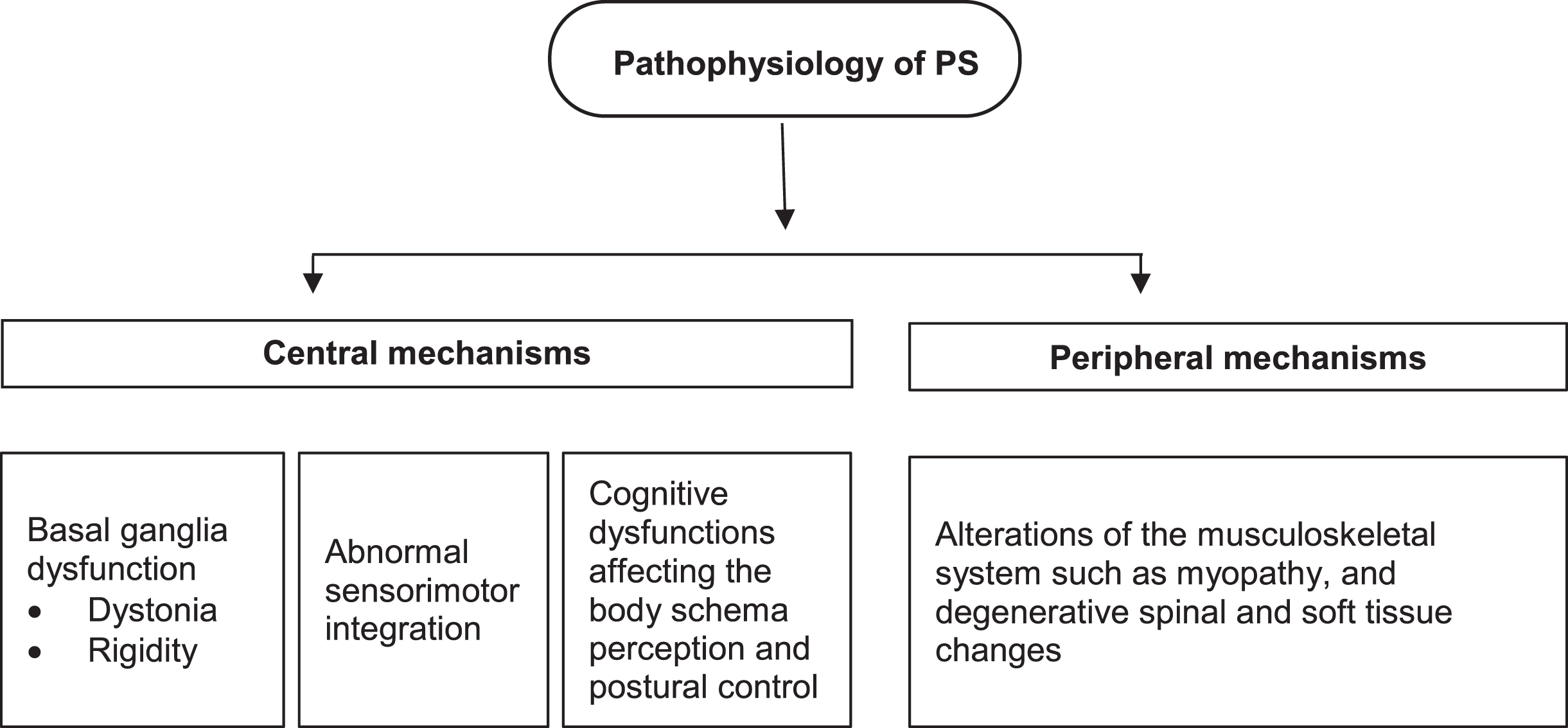
Pathophysiological mechanisms of Pisa syndrome.
Animal studies and clinical data corroborate the key role played by the basal ganglia in the origin of PS. Studies on rats indicated that degeneration of the nigrostriatal pathway causes the leaning of the trunk (Herrera-Marschitz, Utsumi, & Ungerstedt, 1990). The substantia nigra (SN) is a structure divided into two regions. The first contains dopanergic neurons (SNpr), whereas the other one contains gamma aminobutyric acid inhibitors (GABAnergic) (Margherita Fabbri et al., 2017). Damage to SN leads to neurological diseases (Ghassaban et al., 2019). The fact that patients lean away from the side that is most affected has also been corroborated in a number of clinical studies which indicate the dysfunction of the basal ganglia, even though such a conclusion may not be drawn from all research reports (Di Matteo et al., 2011; Tinazziet al., 2015; Baik et al., 2009).
There is a notable scarcity of data supporting the peripheral or musculoskeletal hypothesis. Neuropathological studies in which the investigators set out to account for abnormal posture through the primary changes, which might possibly occur in the musculoskeletal system, are very few indeed (Castrioto et al., 2014; Wrede, Margraf, Goebel, Deuschl, & Schulz-Schaeffer, 2012). Most of the studies seem to give credence to the central hypothesis with regard to the origin of PS.
The origins and development of PS is complex, and may vary depending on the concomitant disease. In the individuals diagnosed with Parkinson’s disease, the actual onset of the syndrome has been associated with the intake of typical and atypical antipsychotics, antidepressants, antiemetics, and cholinesterase inhibitors, or alterations in their dosage. Investigators put forward a working hypothesis that the development of PS may well be associated with a cholinergic-dopaminergic imbalance (Villarejo et al., 2003).
Dysfunction of the somatosensory and sensory systems, responsible for postural and balance control, also play a significant role (Borel & Alescio-Lautier, 2014). Individuals affected by Parkinson’s disease do not exert any control over their posture by making use of the proprioceptive signals, which come from the joints and muscles. Consequently, such individuals additionally affected by PS find it far more difficult to maintain correct posture (Michel et al., 2015; Geroin et al., 2015). Overall postural stability depends on the time and speed at which the nervous system actually processes any postural feedback caused by a loss of balance.
Disturbances in its control are associated with dysfunctional eyesight, vestibular system, somatosensory system, and inappropriate performance of the motoneuron caused by SN (Vaugoyeau & Azulay, 2010).There is a correlation between postural control and cognitive processes. Postural control depends on motor-cognitive integration (Horak, 2006). A study by Vitale et al. assessed the effect of cognitive functions and their impairments on the incidence of PS in the individuals affected by PD. The study group was comprised of 40 patients, half of them diagnosed with PS. Following the assessment of the results yielded by a neuropsychological exam, a significant association was established between the incidence of PS and attention disorders, and also with the visual and perceptual functions (Vitale et al., 2015).
The outcomes of the study conducted by Laudisio et al. 2019 indicate that PS is associated with an increased risk of 2-year mortality in PD (Laudisio et al., 2019). This association was independent of comorbid conditions, use of medications, disease severity, and individual lifestyle habits. The prevalence of PS was 21%, thus corroborating the assertion whereby this syndrome was commonplace among the older PD patients.
Axial symptoms have been associated with increased mortality in PD patients, but several factors might be instrumental in this mechanism. In line with the “central hypothesis”, PS is characterized by an imbalance in the dopaminergic-cholinergic and serotonergic adrenergic pathways. This condition might lead to autonomic dysfunction, associated with disability and mortality. As far as the “peripheral hypothesis” is concerned, though, PS depends on myopathy with degenerative spinal and soft-tissue changes. Notably, sarcopenia has been associated with a decreased survival rate in several settings. Regardless of the pathophysiological pathway, PS has been associated with dopaminergic therapy, stage of the disease, and comorbidities effectively reflecting the actual severity of the disease.
The management of PS, owing to insufficient appreciation of principal pathophysiological mechanisms directly accountable for the development of postural deformities, poses a major clinical challenge in a therapeutic approach. As evidenced through available research data, redesigning and suitable adjustment of pursued pharmacotherapy (i.e. antipsychotics, antiparkinsonian therapies) may well be considered the first-line intervention, whereas specific pharmacological, non-pharmacological, and surgical strategies as the second- or third-line interventions (Fig. 2).

Management of Pisa syndrome (according to Barone, Santangelo, Amboni, Pellecchia & Vitale, 2016).
Effective diagnosis of PS in the course of extrapyramidal symptoms is hard to accomplish, especially if it appears an isolated symptom. In the event when it happens to be a component of a fully-fledged syndrome, it is much easier to have it identified. In view of the fact there are no clear-cut diagnostic criteria in place, the diagnostic process is based primarily on telling apart (distinguishing) specific dysfunctions. First and foremost, the imaging studies help rule out any pathologies of the skeletal system. Neurophysiological tests (electromyography, peripheral nerve conduction study), muscle biopsy and serological tests are helpful in looking for the neuromuscular etiology of the presented symptoms. What counts most, however, is an in-depth interview, accompanied by a comprehensive neurological exam, in due consideration of any pharmacotherapy which might possibly affect the dopaminergic system.
In tackling PS, following prior diagnostic appraisal of the caseat issue, dopaminergic treatment may be pursued, deep brain stimulation applied, surgical intervention specifically targeted at the fixed bone deformities, as well as a course of botulinum toxin injections (Barone et al., 2016; Galbusera et al., 2018; Chieng, Madhavan & Wang, 2015). Early motor rehabilitation may also prove helpful in preventing the development of PS. A target-oriented, physical regimen offers an effective option in prevention, as well as generally supports the entire rehabilitation process in the individuals affected by PS (Dutta, 2020).
Physiotherapy aimed at counteracting the symptoms of PS should commence as soon as PD is diagnosed, even with no visible postural deformities at the time (Frazzitta et al., 2015). Therapeutic exercises should comprise, inter alia, the components aimed specifically at strengthening and stretching the paraspinal, pectoral, and lumbar muscles, as not only would this measure help improve their overall functionality, but also effectively prevent any undue shortening of these muscles (Frazzitta et al., 2015). The patient’s external oblique abdominal muscle should be strengthened on the weakened side, whereas on the less affected one - stretched out (Frazzitta et al., 2015; Di Martino et al., 2011).
As a result of the proprioceptive disintegration, which takes place in PS, a patient should work on correcting his posture and pursue the exercises with the aid of a mirror, so as to enhance his awareness of his own posture through visual feedback (Okada et al., 2014). Physiotherapy offered in an aquatic environment is yet another form of training for the individuals exposed to the risk of PS, as it facilitates correction of postural deformities in the sagittal and frontal planes (Volpe et al., 2017). Backstroke swimming is an effective exercise specifically aimed at improving body symmetry and strengthening the back muscles (Frazzitta et al., 2015). Due attention should also be paid to the osteporotically related fractures in the course of PS, as there are some case reports directly indicative of such a correlation (Etoom et al., 2020).
Physical rehabilitation in PS
There have been few clinical studies to date focused specifically on assessing the effect of target-oriented exercise regimens aimed at remedying any postural deformities, or at having them delayed in the individuals affected by PS.
In the study by Bartolo et al. (2010), the study group consisted of 22 subjects affected by PS (mean age 71.9 years; mean Unified Parkinson Disease Rating Scale-III (UPDRS-III) score 32.9). In each exercise session, the main focus rested on improving trunk control during the pursuit of tasks of different levels of difficulty, as well as on correcting any existing trunk deviations in the subjects. The subjects pursued the exercises under supervision for 90 minutes (including warm-up and a series of relaxation exercises), 5 days per week, for 4 weeks. Postural exercises were based on the strength training grounded in a functional context, stretching exercises, and gait and balance training.
Upon conclusion of the study, improvement was reported in UPDRS-III (mean score of 24), and a noticeable improvement in the trunk lateral flexion. The subjects had visibly improved quality of their gait and posture, and standing up from a chair, whilst overall stiffness also receded. On the other hand, those benefits failed to prove of lasting character and declined after 6 months. The investigators concluded that the motor exercises of the trunk could improve clinical status in the subjects affected by PS in PD, whereas assessment of individual movement and posture appeared a useful tool in predicting and routine monitoring of pharmacological interventions in the PD patients with lateral trunk flexion. Continuing the exercises by the patients in the post-therapy period might appreciably help retain the already gained benefits.
Capecci et al. (2014) randomly assigned the patients to 3 groups. Group I pursued an exercise regimen (7 patients), Group II - postural exercises and kinesiotaping (6 patients), whereas the Controls (7 patients) had no exercise regimen assigned. Both study groups comprised the patients with postural deformities in PD, two patients affected by PS among them. The mean age in Group I was 66.8 years, Unified Parkinson Disease Rating Scale-II (UPDRS-II) range of 7–24, and UPDRS-III range of 9–36. In Group II, the mean age was 73.4 years, UPRDS-II scores ranged 5–23, and UPRDS-III scores ranged 7–28.
Both exercise groups pursued a 40-minute therapy for 4 weeks, 3 days a week. Group II benefited from extra kinesiotaping, apart from the pursuit of routine postural exercises. The therapeutic goals were defined as aligning the trunk to the head in the sagittal and frontal planes, and improving its motor coordination along with the physiological respiratory one. The applied therapy improved balance in the BBS test (Berg Balance Scale), gait TUG (Timed Up and Go Test) and trunk posture in the sagittal and frontal plane. Within one month of the therapy the effects were established to persist (except for the lateral trunk flexion).
The authors concluded that proprioceptive stimulation combined with the stretching of contracted muscles and correction of the trunk posture stood a fair chance of improving the axial symptoms in the PD patients. Owing to the inherent limitations of the study design, in conjunction with a small number of the patients affected by PS, the authors found themselves unable to offer a reliable statistical analysis with regard to their investigative effort.
Lena et al. (2017) conducted postural exercise therapy on 6 individuals (mean age 68.6 years) affected by PS in PD. Group I consisted of 3 subjects with ipsilateral paraspinal muscle hyperactivity, whereas Group II two consisted of 3 subjects with a contralateral one. The therapy was comprised of 10 sessions of 90 minutes each, focused on a special trunk rehabilitation exercise regimen. Stretching, strengthening, and breathing exercises, as well as gait training, balance, and passive mobilisation of the spine were addressed in each training session. The therapeutic goal consisted in correcting postural deformities, and improving overall trunk control and functionality.
Upon concluding the physiotherapeutic intervention, significant improvement was noted in both groups. In Group I, the mean UPDRS-II (activities of daily living) score dropped from 14.67 to 8.33, UPDRS-III (motor functions) from 21 to 17.67, back pain according to VAS scale from 7 to 5.33 and trunk lateral flexion from 24 degrees to 15. In group II, UPDRS-II from 18.67 to 14.67, UPDRS-III 36.67 to 33.67, pain from 7 to 5.67 and trunk lateral flexion from 22° to 8.33°. There was no control group in the study, whilst duly acknowledging the small group of subjects, the authors postulated that further clinical studies be pursued on much larger population samples.
There is no information regarding the third measurement point, nor indeed any mention how the effects of the training were maintained within a few months of completing the study protocol. Taking into account the actual results yielded by that pilot study, the authors concluded that postural exercises might well be a legitimate component of any rehabilitation regimen specifically intended for the patients affected by PS.
Some studies also highlight the benefits of combining rehabilitation treatment with the injections of botulinum toxin (BTX), where the exercises should be primarily focused on the actual strengthening of the weaker side, whereas the application of BTX should be meant to effectively relieve the extra tension in the overstretched muscles (Santamato et al., 2010; Tassorelli et al., 2014).
Tasorelli et al. (2014) randomly allocated 26 individuals affected by PS into 2 separate groups. Both groups were subjected to a 4-week therapeutic intervention focused on the pursuit of rehabilitation exercises, whereas in Group I,BTX type A was injected into the hypertoned muscles (paravertebral, abdominal, and iliac-lumbar ones) prior to the first exercise session, and in Group II saline placebo was injected instead. Therapists focused on reducing overall back pain, and on correcting trunk lateral flexion and UPDRS scores.
Upon concluding the therapeutic intervention, the patients exhibited significant improvement in the key variables under study, in both the BTX and the placebo groups. In the BTX group, a greater reduction in pain was noted, in line with the Visual Analog Scale for pain (VAS),accompanied by appreciably smaller reduction in the befits originally gained through the intervention within 6 months of its conclusion (established at the 3rd measurement point). The authors believe that BTX enhances the effects of exercise therapy and supports overall treatment management in terms of overall postural stability, trunk mobility, and pain reduction.
Santamato et al. (2010) in their case study addressed the outcome of a therapeutic intervention in a 68-year-old man, combining rehabilitation exercises and the injections of BTX-A. The subject’s trunk lateral flexion was 35° (Cobb angle), pain on a VAS scale –7/10, plus mobility problems. The therapy was pursued 5 times a week, in 2-hour sessions, whereas the BTX-A injection was applied prior to the first training session, in the lower back, in the excessively tight muscles located in the area from the 10th thoracic vertebra to the 2nd lumbar vertebra. The physical therapy comprised a system of Pilates exercises, stretching, and mobility exercises.
Within 15 days, the lateral flexion angle was reduced down to 15°, pain was self-assessed by the patient as 3/10, and the Trunk Dystonia Disability Scale (TDDS) score improved by 5 points. Training was then reduced to 3 times a week for 1 hour, for further 3 months. The originally gained benefits were established to have been maintained. The authors believe that combining the exercise regimen with BTX-A injections may be an effective method for patients affected by PS. There is no follow-up data on the patient after the therapy, though.
Falls risk in PS
The balance control system, which is based on the processing of somatosensory, visual, and vestibular signals, allows the body to adopt and maintain a stable posture, protecting it against the risk of falling. Adequate operation of this system deteriorates with age, along with the incidence of comorbidities, as confirmed by the study pursued by Skalska et al. (Skalska, Ocetkiewicz, Zak, & Grodzicki, 2004; Puszczalowska-Lizis, Bujas, Jandzis, Omorczyk, & Zak, 2018). Putting in place an interdisciplinary team, tasked with having the individuals particularly at risk of falling identified, is deemed expedient in terms of offering an opportunity for effective preventive actions to be immediately undertaken (Szczerbinska, Zak, & Ziomkiewicz, 2010).
Trunk control is an essential prerequisite for retaining balance, moving around effectively (gait), and being functionally independent (Shih, Gordon, & Kulig, 2021; Zak, Krupnik, Puzio, Staszczak-Gawelda, & Czesak, 2015, Zak et al., 2017). PS, in view of accounting for impaired postural control, may become instrumental in potentially dangerous incidents like falls, some of which might result in femoral neck fractures (Grisso et al., 1991; Cole, Silburn, Wood, Worringham, & Kerr, 2010; Horak, 2006).
Falls risk in the individuals affected by PS is high in view of a deformed trunk resultant from the lateral flexion (Cheng et al., 2014; Lena et al., 2017). Van de Raktand Mccarthy-Grunwald (Van de Rakt, & Mccarthy-Grunwald, 2020) applied therapy to a 73-year-old man who was placed in a 24-hour nursing home. While living on his own, he would fall 5–10 times per day on average. The man scored 30/56 in the BBS test, whereby a score below 45 indicates an exposure to falls risk (Berg, Wood-Dauphinee, Williams, & Maki, 1992). The therapeutic management making use of hydrotherapy proved effective for this patient and appreciably improved his overall functionality.
In a large cohort study conducted by Tinazzi et al. (2015) on 1631 individuals affected by PD, 143 of them were also affected by PS. Patients affected by PS were exposed to a higher falls risk, reported more frequent falls, and were characterised by the so-called “veering gait”. The PS patients were exposed to a higher falls risk, admitted to a higher number of reported falls, and to the “veering gait”, i.e. involuntarily bending to one side while walking back and forth, with their eyes closed. Among the PS patients, 19.6%sustained falls, whereas among the PD ones, with no concomitant PS, 9.7%only. The “veering gait” characterised 30.1%of the PS patients, and 10.1%among those were affected by the PD with concomitant PS. Gait assessment in the PS patients indicated reduced gait speed and stride length (Tramonti et al., 2017). This was associated with reduced functional capacity correlating with the severity of postural deformities. Kinematic data indicated that in the PS patients, a reduced joint range of motion was encountered in all lower limb joints, whereby in the case of captocormia such a reduction was established to have affected mainly the hip and knee joints only (Tramonti et al., 2017). Abnormal range of motion in the lower limbs and hips contributed to balance disorders which may well result in sustaining falls by the affected individuals.
Balance, balance training (Laessoe, Hoeck, Simonsen, Sinkjaer, & Voigt, 2007) and correct gait account for reducing overall exposure to falls risk (Osoba, Rao, Agrawal, & Lalwan, 2019). Apart from reducing the falls risk through postural, balance, and stretching exercises (preferably combined with BTX-A injections), training with the PS patients might well be extended to comprise practical (hands-on) instructions on how to get up again unassisted after sustaining an accidental fall, as the individuals remaining in 7/24 institutional care happened to be a minority. Patients affected by PS in PD, owing to the restricted range of motion in their trunks and accompanying deformities are also frequently characterised by reduced upper and lower limb muscle strength (Inkster, Eng, MacIntyre, & Stoessl, 2003; Roberts, 2015), which can make it far harder for them to cope with a post-fall situation, as compared to the individuals unaffected by PS.
Besides, the effects gained throughout therapeutic management often fade away after its conclusion, so in result the patient returns to the similar clinical variables as before to the actual intervention (Bartolo et al., 2010; Capecci et al., 2014), even in the case of surgical treatment (Todisco et al., 2019). An effective method, which may well be made use of by the therapists in instructing patients, is the Backward Chaining Method (BCM). In line with pertinent research, it is found to be much easier for the patients, compared to the conventional one. BCM entails mastering each successive step of getting back up again after an incidental fall before proceeding to the next one, so that the individuals affected by PS may keep on repeating any difficult component without being unduly discouraged or stressed out by it (Zak, Skalska & Szczerbinska, 2008; Leonhardt, Becker, Groß, & Mikolaiczak, 2020). Pursuit of therapeutic management with a PS patient should also take into account the appropriate timing for executing the exercises at issue, as the patients tend to be affected by the greatest stiffness in the morning hours, when this is not alleviated by the medications, as reported by Van de Rakt and Mccarthy-Grunwald (Van de Rakt, & Mccarthy-Grunwald, 2020).
Conclusion
High falls risk and its adverse consequences are associated with a reduced overall quality of life in the individuals affected by PS. One of the key identified risk factors consists in an inadequate trunk control, resultant primarily from a postural deformity in the form of lateral spine flexion. Individuals living on their own are therefore relocated to 24-hour care facilities homes, due to their fear of falling. Rehabilitation of the individuals at risk of PS or already affected by PS should be a comprehensively structured and integrated service, aimed at eliminating all identified risk factors for falls, and/or offering effective preventive measures to the individuals found at risk.
Optimally designed physical therapy for the PS patients should be made up of both typically therapeutic components, e.g. structured postural exercises aimed at sustaining a correct posture, whilst at the same time helping reduce the pain in the lumbar part of the spine, as well as the educational and preventive exercises, with a view to instructing the patient how to cope after a an incidental fall effectively, i.e. unassisted by any third party. As evidenced by current studies, clinical symptoms of PS often tend to recur within several months of completing the therapeutic management.
All patients should therefore pursue the appropriately structured exercise on their own, effectively retarding the recurrence of PS symptoms. Planning a training session with a PS patient should take into account his individual susceptibility to body stiffness, which tends to occur at different times of the day, so that all due exercising is actually pursued when it is at its lowest level.
Owing to overall scarcity of clinical studies on the large population samples of patients affected by PS, in conjunction with the still unclear origin of this disorder, further research is still required, with a view to identifying and developing the most effective therapeutic measures.
Conflict of interest
The authors have no conflict of interest to declare.
Funding
This research project was funded by the Minister of Science and Higher Education - “Regional Initiative of Excellence” - spanning the period 2019–2022; grant ref. no. 024/RID/ 2018/19; amount of financing allocated to the project: PLN 11 999 000.00.