
Abstract
BACKGROUND:
Assessing physical activity (PA) in people with multiple sclerosis (PwMS) is essential to follow-up the recommended PA level. The International Physical Activity Questionnaire (IPAQ) and the Incidental and Planned Exercise Questionnaire (IPEQ) have been widely used, but their validity has not been investigated previously in PwMS.
OBJECTIVE:
This study aimed to assess the convergent and criterion validity of the IPAQ and the IPEQ in PwMS.
METHODS:
50 PwMS were asked to wear an Actigraph for seven days and to fill the IPAQ and IPEQ. Sedentary, moderate (MPA), vigorous (VPA) and moderate to vigorous PA (MVPA) levels were recorded.
RESULTS:
Significant correlations were found between sitting time as reported by IPAQ and sedentary time as recorded by Actigraph (r = 0.41, p = 0.003), VPA by IPAQ and VPA as recorded by Actigraph (r = 0.46, p = 0.001), and MVPA by IPAQ and MVPA by Actigraph (r = 0.36, p = 0.011). IPEQ showed poor both criterion and convergent validity when compared to the Actigraph. Both IPAQ and IPEQ overestimate the intensities of PA for all the derived parameters.
CONCLUSIONS:
Findings of this study are important as they suggest that IPAQ in particular had convergent validity when compared to Actigraph data, but still had the problem of overestimating PA levels.
Keywords
Introduction
Interventions that target physical activity and exercise represent an important area of research in neurodegenerative diseases NDDs (Spielman, Little, & Klegeris, 2016). Studies indicate that lifestyle factors, including physical activity, may change the course of NDDs and impact the severity of motor and non-motor symptoms (White & Castellano, 2008). In people with multiple sclerosis (PwMS), regular exercise and physical activity can improve function and quality of life, as well as have other positive behavioural and health-related benefits (Latimer-Cheung, Pilutti, et al., 2013). For example, level of physical activity in PwMS correlated with the number of relapses, sleep impairment, quality of life, depression and anxiety (Latimer-Cheung, Pilutti, et al., 2013). On the other hand, many trials showed that engaging PwMS in physical activity and exercise programmes helped to decrease the affected symptoms, such as: sleep; coordination, cognitive function and depression (Aburub, Khalil, Al-Sharman, Alomari, & Khabour, 2017; Al-Sharman, Khalil, El-Salem, Aldughmi, & Aburub, 2019; Briken et al., 2014). Therefore, there has been growing attention toward evaluating and measuring physical activity as an outcome in research and practice involving PwMS.
Generally, it is of importance to assess different levels of physical activity accurately. This is because people are required to perform specific level of physical activity intensities per week. For example, the World Health Organisation recommended performing 150 minutes of moderate intensity physical activity per week or at least 75 minutes of vigorous intensity aerobic physical activity per week to improve and/or maintain general health (World Health Organization, 2010). Accordingly, people might be able to do the required amount of time spent in physical exercise, but might not be able to measure the intensity of exercise accurately. Additionally, healthcare providers and researchers will be in need to assess if people are performing exercise and physical activity that meet the recommendations. Similarly, PwMS who have mild to moderate disability are recommended to perform at least 30 minutes of moderate intensity aerobic activity two times per week and strengthening exercises for major muscle groups two times per week or to perform 30 minutes of moderate to vigorous PA per day (Latimer-Cheung, Ginis, et al., 2013). These exercises are often performed, and recommended, as part of self-management plans in PwMS (Latimer-Cheung, Ginis, et al., 2013). Being unsupervised while performing exercise might lead people to underestimate or overestimate their performance. Thus, it is crucial to check if current tools of physical activity measurements are valid and reliable in PwMS, and to choose the best outcome, where possible.
In PwMS, both subjective and objective measures of physical activity are widely used in healthcare research (Motl, McAuley, & Snook, 2005).
Overall, physical activity questionnaires as subjective measure of physical activity, remain cheaper and in hand for most healthcare institutes. The International Physical Activity Questionnaire (IPAQ) is the most common used questionnaire to assess physical activity in the general population (Lee, Macfarlane, Lam, & Stewart, 2011). However, validity of the IPAQ in people with MS was assessed only in one study by comparing it with activity monitor data (Gosney, Scott, Snook, & Motl, 2007). In this later study, Gosney et al (2007) assessed the validity of the total score of IPAQ without assessing the validity of each level of physical activity including: sedentary; light; moderate; moderate to vigorous; vigorous and very vigorous physical activities. Only one study investigated validity of time spent in sedentary physical activity in PwMS using IPAQ, but did not explore validity of time spent in light, moderate, vigorous and moderate to vigorous physical activity (Motl, Sasaki, Cederberg, & Jeng, 2019). Although IPAQ scores for the different physical activity levels was not validated in MS yet, many studies depended on IPAQ as a tool of assessing levels of PA in PwMS (B. Sandroff et al., 2012). Similarly, the Incidental and Planned Exercise Questionnaire (IPEQ) has been widely used in other populations, and found to be valid and reliable tool for assessing physical activity (Merom et al., 2014). The IPEQ was used previously in one study in PwMS (Vister, Tijsma, Hoang, & Lord, 2017). As yet, its validity in this population is not established.
With the advances in technology, objective measures of physical activity, by mean of activity monitors, became an important method in managing and/or reducing sedentary lifestyle effects in the general population (Matthews, Hagströmer, Pober, & Bowles, 2012). Activity monitors are widely used in MS studies related to physiotherapy and general health research (Matthews et al., 2012). Although, the limitation of activity monitors that some monitors might not pick all the activities, such as stationary cycling, swimming or climbing stairs, data collected from physical activity monitors do not depend on memory and recall bias that could happen while using subjective questionnaires including the IPAQ and the IPEQ (Ekelund et al., 2006). Moreover, activity monitors such as Actigraphs have been validated for specific cut-points for different levels of physical activities, specifically in PwMS (B. M. Sandroff, Riskin, Agiovlasitis, & Motl, 2014). Therefore, this study aimed to assess the convergent and criterion validity of the self-administered, short form of the IPAQ and the IPEQ for measuring different levels of physical activity in a sample of PwMS using the activity monitor (Actigraph) as the criterion instrument. For the convergent validity, it was hypothesized that PA parameters recorded by the IPEQ and IPAQ would have moderate positive correlations with the corresponding PA parameters derived from the activity monitor. Additionally, for the criterion validity, it was hypothesized that PA parameters recorded by the IPEQ and IPAQ would agree with the corresponding PA parameters derived from the activity monitor.
Methodology
Study design and participants
The data for this study was obtained as part of baseline data of ongoing studies at Jordan University of Science and Technology (JUST). Overall, participants were recruited from the King Abdulla University Hospital (KAUH) in Irbid, Jordan, as well as from a database of JUST. Sequential MS patients attending routine neurology clinic appointments at KAUH between January 2019 and October 2019 were screened for eligibility by a neurology consultant. Eligible subjects were invited to participate in the study. Brochures and adverts about the study were also distributed. Participants who were willing to participate were also screened for eligibility by a neurology consultant. Inclusion criteria were: 1) neurologist-confirmed diagnosis of MS according to the revised McDonald criteria; 2) no exacerbation of symptoms 30 days prior to completing testing; 2) ability to walk independently with or without walking aid outdoor for at least 10 metres; 3) age ≥18 years; 4) capacity to give informed consent. Exclusion criteria were: 1) presence of other neurological disorders such as stroke; and 2) presence of severe cognitive deficits or behavioural disorders preventing participation. All participants gave written informed consent approved by the Institutional Research Committees of the Jordan University of Science and Technology (HK-20190037).
Physical activity by self-report
Self-reported physical activity was recorded using the short, self-administered version of the IPAQ. It has 7 items assessing physical activity during the last 7 days by questioning the weekly frequency (i.e. number of days in the last week) and daily intensity (i.e. number of hours per day) people spent in walking, performing moderate or vigorous levels of physical activities and sitting on weekdays and weekends. The respective frequency and duration values for vigorous, moderate and walking activities were first multiplied together. The resulting volumes of vigorous, moderate and sitting activities were then multiplied by 60 to estimate number of minutes spent in vigorous, moderate and sitting activities in the last week and then divided by 7 to calculate the average time in minutes per day performed in moderate and vigorous activities as well as in sitting. This conversion into minutes per day was performed to facilitate comparison with the other collected outcome measures. Accordingly, four PA indicators were used in the analysis derived from the IPAQ: moderate PA (MPA) (average minutes/day), vigorous PA (VPA) (average minutes/day), moderate to vigorous PA (MVPA) (average minutes/day) in which moderate and vigorous PA were summed and, sitting or sedentary (average minutes/day). Also, participants were categorised into sufficiently active (≥30 minutes of moderate to vigorous PA per day) or insufficiently active (<30 minutes of moderate to vigorous PA) using both Actigraph data and IPAQ and IPEQ scores according to the exercise guideline recommendations available for PwMS (Ronai, LaFontaine, & Bollinger, 2011). Overall, according to IPAQ instructions, vigorous activities are activities that make participants breathe much harder than normal and may include heavy lifting, digging, aerobics, or fast cycling for at least 10 minutes at a time. Moderate physical activities are activities that make participants breathe somewhat harder than normal and may include carrying light loads, bicycling at a regular pace, or playing tennis for at least 10 minutes at a time. Walking section include questions about walking at work and at home, walking to travel from place to place, and any other walking that a person might do solely for recreation, sport, exercise, or leisure.
In addition to the IPAQ, the Incidental and Planned Exercise Questionnaire (IPEQ) was used to record self-reported physical activity. The IPEQ covers thefrequency and duration of planned and inciden-tal physical activities and has high reported test-retest repeatability (intraclass correlation coefficient = 0.84) (Delbaere, Hauer, & Lord, 2010). The IPEQ contains ten items about time spent in physical activity per week in the past 3 months. The first six items consider planned exercises and planned walking in which planned exercise is defined as physical exercises aimed at improving and maintaining balance, strength, flexibility, and coordination. The last four items consider incidental exercise: The weekly frequency and the daily duration of walks to get to places, and average daily time spent doing outdoor and indoor activities such as gardening and house cleaning (Delbaere et al., 2010). Average weekly time spent on each IPEQ question was calculated by multiplying the weekly frequency with the daily duration using the median point for each response (i.e. one to two times a week equivalent to 15–30 min, which is 22.5 min) (Merom et al., 2014). One indicator of PA was derived from the IPEQ which is average minutes per day spent in MVPA. This was calculated by summing the minutes across all questions excluding the indoor chores question and then dividing the total by 7. The indoor chores question was excluded as according to the PA compendium an absolute MET value of 3 or less is assigned to these activities which is lower than the accepted cut-point for moderate intensity exercise (Ainsworth et al., 2000).
Criterion measurement of PA
Objective assessment of physical activity were collected using the Actigraph (ActiGraph; Pensacola, FL, USA), a valid and reliable tri-axial accelerator to monitor mobility in PwMS (Kos et al., 2007). Participants were instructed to wear the Actigraph around the waist for 7 days during all waking hours except while swimming or showering. Actigraph signals were sampled with 30 Hz. Activity was calculated for all axes for 10 second periods. Non-wear periods were excluded from the analysis. Only days with more than 10 hours wear time for 4 days were included in the analysis to assure quality of data (Colley, Gorber, & Tremblay, 2010). This data quality control method (i.e. at least 10 hours for 4 days) is essential to reduce the limitations when assessing different levels of physical activity including the low (LPA, < 591 counts per min), moderate (MPA, 591–6460 counts per min), moderate to vigorous (MVPA) and vigorous (VPA, more than 6460 counts per min) levels of physical activity. Data from Actigraph was downloaded and analysed using Actilife software (ActiGraph; Pensacola, FL, USA). Physical activity data was processed with Freedson adult algorithm (Freedson, Melanson, & Sirard, 1998), to obtain the average minutes per day spent in LPA, MPA, VPA, MVPA and sitting or sedentary.
Statistical analysis
Descriptive statistics were calculated for all variables. Data was checked for normality usinghistograms (Statistical Package for the Social Sciences (SPSS) version 21 (SPSS Inc., Chicago, IL, USA)). To investigate the convergent validity of the IPAQ and IPEQ, their correlations with Actigraph data were computed using Spearman’s correlation coefficients. A spearman correlation coefficient of ≥0.7 indicates strong correlation, 0.4 to 0.6 indicates moderate correlation, and 0.10 to 0.3 indicates weak correlation (Akoglu, 2018).
To investigate the criterion validity, Bland-Altman plots (Dewitte, Fierens, Stockl, & Thienpont, 2002) were generated for IPAQ sitting, IPAQ MPA, IPAQ VPA, IPAQ MVPA, and IPEQ MVPA and accordingly the 95% limits of agreement (LOA) were calculated to evaluate the agreement between the Actigraph derived measures and the IPAQ and IPEQ reported variables. We plotted the difference between the criterion (i.e. Actigraph) and self-reported measures against the average of the criterion and the self-reported measure for each variable. Furthermore, paired t test was conducted to examine if there is any systematic difference in the measurements. Linear regression was also conducted to evaluate objectively if there is proportional bias in the measurements using the difference score between the criterion (i.e. Actigraph) and the corresponding self-reported measure as the dependent variable and the mean score of the criterion (i.e. Actigraph) and the corresponding self-reported measure as the independent variable. In addition, agreement between participants meeting or not meeting the activity guideline for PwMS (i.e. a minimum of 30 minutes of MVPA per day to be regarded as sufficiently physically active), as determined by the two different methods, was assessed using the chi-square test. Sensitivity (ability of the IPAQ or IPEQ to identify not sufficiently active individuals) and specificity (ability of the IPAQ or IPEQ to identify sufficiently active individuals) for this measure were used to further assess their criterion validity. Statistical level was set at p < 0.05. SPSS Statistics version 25.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Results
The demographic characteristics of the participants are presented in Table 1. Data were collected from 50 participants (39 females, 11 males) with the mean (SD) of age was 36.7±10.04 years. Table 1 demonstrates the descriptive data obtained by the activity monitor (i.e. Actigraph) and self-reported PA from the IPAQ and the IPEQ. Overall, based on IPAQ data, 58% of participants reported no participation in vigorous- intensity PA. In total, 36% of participants according to IPAQ and 70% of participants according to IPEQ did not achieve the recommended amount of PA, as they reported MVPA for less than 30 minutes a day and therefore were regarded as insufficiently active. Regarding data derived from the Actigraph, 22% did not register PA at vigorous- intensity level and additionally, 74% of participants did not accumulate at least 30 min per day at MVPA intensity and therefore were regarded as insufficiently inactive (Table 2).
Demographic data and objective and self-reported PA variables
Demographic data and objective and self-reported PA variables
RRMS: Relapsing Remitting MS, EDSS: Expanded Disability Status Scale, PA: Physical activity, IPAQ: International Physical Activity Questionnaire- Short Form, IPEQ: Incidental and Planned Physical Activity Questionnaire
Number (%) of participants classified as being sufficiently active according to PA recommendations to MS individuals by self-report measures and Actigraph
*Chi-square test for proportions (p = 0.013). **Chi-square test for proportions (p = 0.94).
Regarding convergent validity, Pearson correlation analysis showed that there is a significant correlation between sitting time as reported by IPAQ and sedentary time as recorded by Actigraph (r = 0.41, p = 0.003), VPA as reported by IPAQ and VPA as recorded by Actigraph (r = 0.46, p = 0.001), and MVPA as reported by IPAQ and MVPA as recorded by Actigraph (r = 0.36, p = 0.011) (Table 3).
Correlations (Spearman (r)) between Actigraphy and IPAQ and IPEQ variables
PA: Physical activity, IPAQ: International Physical Activity Questionnaire- Short Form, IPEQ: Incidental and Planned Physical Activity Questionnaire.
Regarding the criterion validity, significant differences were noted on paired t-test between the variables derived from the Actigraph and the corresponding variables recorded on IPAQ (p < 0.0001) (Table 1), which indicates the presence of systematic difference between the objectively recorded data and the self-reported variables. This is supported by the observation that the average score of the criterion and the self-reported measure can always predict the difference between the criterion and the self-reported measure (p < 0.001), which indicates a significant proportional bias in the variables obtained from the self-reported questionnaires (i.e. IPEQ and IPAQ) (Table 5). The calculated LOA were large for all variables obtained from the IPAQ or the IPEQ (Table 5). The Bland and Altman plots indicated that the IPAQ or the IPEQ variables are consistently smaller than the corresponding Actigraphy data at lower time values and vice versa (i.e. participants reported bigger IPAQ and IPEQ values thancorresponding Actigraphy data at higher times values) (Fig. 1). This applies to all physical activity intensities including sedentary time, moderate, vigorous, and moderate to vigorous physical activity levels.
Linear regression analysis examining the associations with the difference between Actigraph data and self-reported measures
PA: Physical activity, IPAQ: International Physical Activity Questionnaire- Short Form, IPEQ: Incidental and Planned Physical Activity Questionnaire.
Limits of agreements and their 95% confidence interval derived from Bland and Altman analysis
PA: Physical activity, IPAQ: International Physical Activity Questionnaire-Short Form, IPEQ: Incidental and Planned Physical Activity Questionnaire.
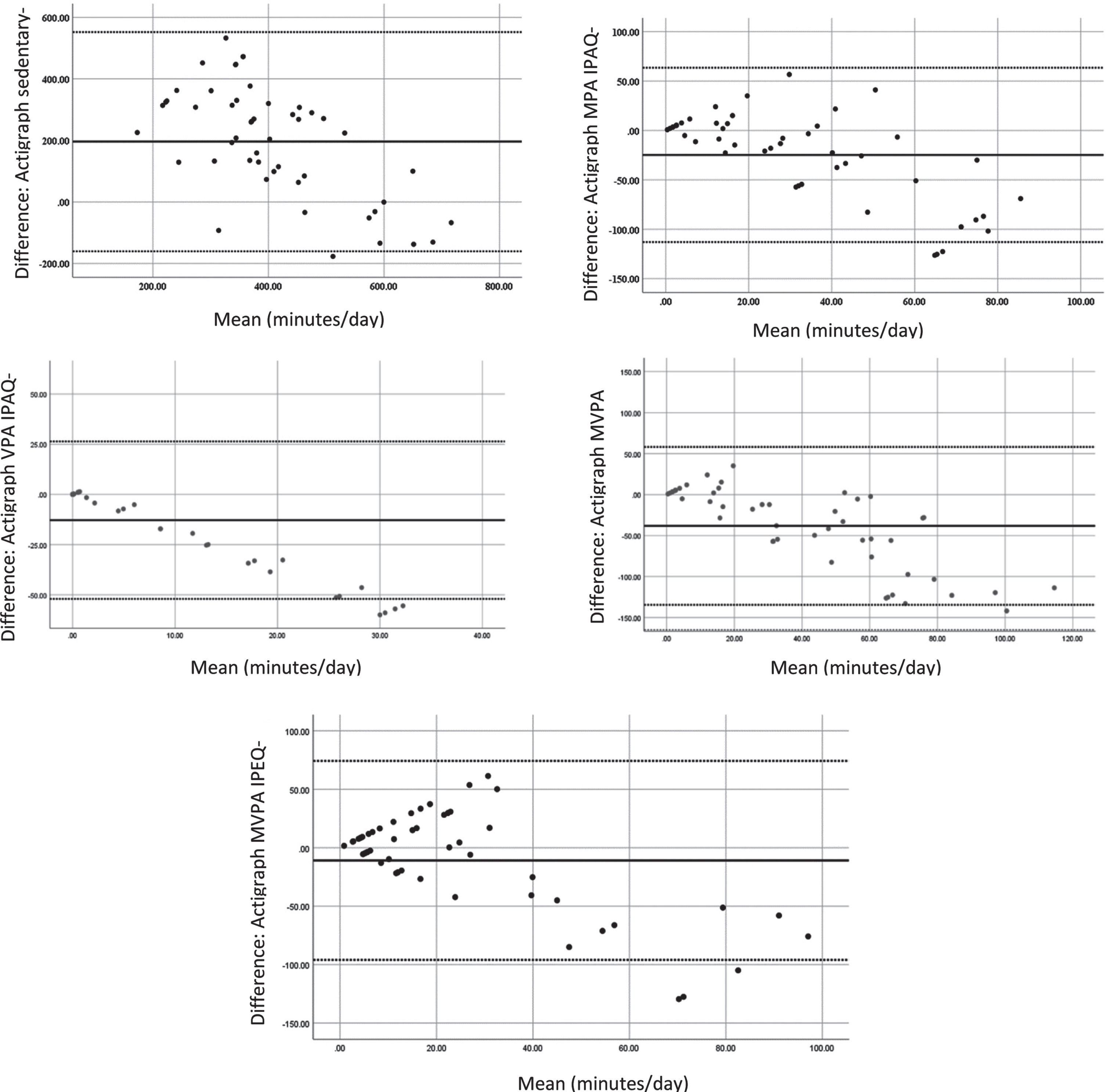
Bland Altman plots of physical activity parameters measured by Actigraphy and by IPAQ and IPEQ. Solid line indicated the mean of difference, and the dotted line indicated 95% limits of agreement.
Overall, the sensitivity of IPAQ to capture insufficiently active MS participants was 92.3%, whereas the specificity of the IPAQ to capture the sufficiently active people as determined by the Actigraph was 45.94%. However, the sensitivity of IPEQ to capture insufficiently active MS participants was 30.7%, whereas the specificity of the IPEQ to capture the sufficiently active people as determined by the Actigraph was 70% (Table 2).
Although many studies have used IPAQ and tested its validity in different populations, this is the first study that investigate validity of IPAQ and IPEQ when compared to Actigraphy in PwMS. Results of this study showed that there are correlations between IPAQ sitting with Actigraphy sedentary measurement, vigorous PA in IPAQ with vigorous PA in Actigraphy, and moderate to vigorous PA in IPAQ with moderate to vigorous PA in Actigraphy,indicating that IPAQ has convergent validity for assessing PA in PwMS. These findings are similar to previous published findings that assessed validity of IPAQ in other populations. For example, IPAQ was found to be valid tool to asses PA in the general population in 12 different countries with high concurrent and construct validity in adults (Craig et al., 2003). Moreover, IPAQ was found to be valid tool to assess PA in people with neurological disorders such as cerebral palsy (Lavelle et al., 2020). IPAQ version used in this study, Arabic version of IPAQ, was also previously validated in the general population (Helou et al., 2018).
Our study has also revealed that the IPEQ has Poor convergent validity to assess PA in PwMS. Although previous studies showed that the IPEQ is a valid and reliable tool when compared with accelerometery in older adults (Delbaere et al., 2010), the current study contradict these findings. The IPEQ was used in one study in PwMS (Vister et al., 2017) without assessing its validity in this population. Thus, this study is the first study that assessed validity of IPEQ in PwMS. IPAQ but not IPEQ might be a cheap and a valid tool to assess PA where Actigraphy are not available / not feasible to be used.
However, when assessing criterion validity, proportional bias between IPAQ and Actigraphy in term of moderate, vigorous, moderate to vigorous PA and sedentary PA in PwMS. These results indicate overestimating PA levels in IPAQ when compared to the Actigraph data, particularly at larger values. In consistent with that, the IPAQ showed high sensitivity level, but very poor specificity level in this study. In other words, when classifying people into sufficiently active and insufficiently active (sufficiently active ≥30 minutes moderate to vigorous PA, insufficiently active < 30 minutes of moderate to vigorous physical activity), IPAQ was accurate in identifying people who are active (sensitive: true positive), but not accurate in term of classifying people as active while they are sedentary in Actigraphy (not specific: false negative). Similarly, IPEQ, had low sensitivity and relatively low specificity too.
Within the realm of criterion validity for IPAQ and IPEQ, a similar finding was reported in a study that assessed validity of IPAQ in people with Chronic Fatigue Syndrome when compared with daily PA diary (Meeus, Van Eupen, Willems, Kos, & Nijs, 2011). In both populations, MS and Chronic Fatigue Syndrome, the IPAQ and IPEQ might augment (ove-restimate) PA level as it depends on memory. Polls et al. (1996) advised that assessments that demands on self-report are not accurate in patients with memory difficulties. Because PwMS might have memory problems, self-reported PA questionnaires might have some recall bias (Pols, Peeters, Kemper, & Collette, 1996). Additionally, PwMS might have difficulties in estimating number of minutes spent in each activity category per day, due to the fluctuating nature of their symptoms during the week or even the day (Powell, Liossi, Schlotz, & Moss-Morris, 2017). The description of moderate- intensity and vigorous- intensity PA in both IPAQ and IPEQ and howindividuals may perceive them may add to this bias of over estimating PA when using these self-reported questionnaires. Therefore, results of the current study suggest that IPAQ and IPEQ need to be considered with caution in research that involves follow up sessions to assess PA in PwMS.
This study is not without any limitations. For example, the sample needs to be larger in size, with different disease severities included. Also, reliability of the IPAQ and IPEQ in PwMS was not addressed. Therefore, future studies are recommended to address validity and reliability of IPAQ and IPEQ in PwMS. Additionally, we do not have information about physical activity in people who did not wear the Actigraph according to the study requirements. Furthermore, the low EDSS of the participants limit the external validity of the study.
Conclusion
Findings of this study are important as they suggest that IPAQ in particular had convergent validity when compared to Actigraph data, but still had the problem of overestimating PA levels. Thus, researchers need to use self-reported measures such as IPAQ and IPEQ with caution if they are going to depend on it as the main outcome measure for PA.
Footnotes
Acknowledgments
The authors would like to acknowledge all participants of the study. Acknowledgement for funding support is given to Jordan University of Science and Technology (grant number: HK-20190037).
Author contributions
Hanan Khalil: conceptualization; data collection; formal analysis; funding acquisition; investigation; methodology; project administration; supervision; writing- original draft; writing - review and editing. Aseel Aburub: conceptualization, formal analysis; writing- original draft; writing - review and editing. Saddam F. Kanaan: conceptualization, formal analysis; writing- original draft, review and editing. Elham AlSharman: data collection; writing- original draft, review and editing. Shada Khazaaleh: data collection; writing- original draft, reviewand editing. Majdi Al Qawasmi: data collection; writing- original draft, review and editing. Khalid El-Salem: data collection; writing- original draft, review and editing.
Conflict of interest
The authors report no conflict of interest.