
Abstract
BACKGROUND:
There are no recommendations for physical activity in amyotrophic lateral sclerosis (ALS) patients.
OBJECTIVE:
(i) To describe the prevalence and pattern of physical activity (PA) in ALS patients; (ii) to explore patients’ attitude towards PA; and (iii) to investigate the relationship between PA at home environment and the rate of functional decline.
METHODS:
96 ALS patients were followed for 6 months at 3-month intervals and assessed by site of disease onset, disease duration, diagnosis delay, functional status, muscle strength, fatigue and prevalence of PA.
RESULTS:
Over 70% of patients performed regular exercise and reported a positive effect of PA on functional status and mood. Regularly exercising individuals showed a higher ALSFRS-R bulbar score (11.0 vs 9.0, p = 0.011) and a lower decline of respiratory sub-score of ALSFRS-R compared to non-regularly exercising patients (0 vs 1.0, p = 0.026). Bulbar onset was a negative prognostic factor for regular exercise (odds ratio [OR]: 5.2, p = 0.004).
CONCLUSION:
The majority of ALS patients perform regular PA and find it positively influence their motor performance and mood. Bulbar disease onset, but not functional status, is a negative prognostic factor for regular exercise in ALS patients. Regular mild PA may result in a slower deterioration of functional status, especially the respiratory function.
Introduction
Amyotrophic lateral sclerosis (ALS) is an adult-onset progressive neurodegenerative disease without an effective treatment. Gradual degeneration of the motor neurons leads to progressive muscle weakness, functional deterioration and immobility.
The positive role of systematic physical activity in reducing body weight, the risk of cardiovascular diseases, stroke, diabetes, cancer as well as falls in the elderly has been well described (Warburton et al., 2006; Hernandez et al., 2010; Ruegsegger et al., 2018). It not only increases mobility, but also improves well-being (Dunn et al., 2001; Gowans et al., 2001). Physical activity has a positive effect on the emotional state, reduces the symptoms of anxiety and depression (World Health Organization, 2020). The role of physical activity in ALS is complex and the actual impact on the course of the disease has not yet been established, despite increasing body of scientific evidence (Pinto et. al., 2012; Bello-Haas, 2018). It is particularly important for patients who led an active lifestyle before the diagnosis of ALS, as well as for physiotherapists who should be able to propose optimal physical activity adjusted for the patient’s functional state (Bello-Haas, 2018). There are several publications reporting a positive association between a highly active life-style in the premorbid period and the risk of developing ALS (Beghi et al., 2010; Mattsson et al., 2012; Eaglehouse et al., 2016; Harwood et al., 2016; Huisman et al., 2013; Visser et al., 2018). It is possible that the physical activity together with a specific genetic profile or environmental factors may also contribute to the development of the disease (Huisman et al., 2013; Hamidou et al., 2014; Luna et al., 2017; Pupillo et al., 2014; Korner et al., 2019; Feddermann-Demont et al., 2017). In contrast, after the onset of ALS, several studies show a potential therapeutic role of holistic physiotherapy, including a beneficial effect of regular physical activity (PA) on the functional state (Drory et al., 2001; Pinto et al., 1999; Sanjak et al., 2010; Bello-Haas et al., 2007; Lunetta et al., 2016; Kitano et al., 2018), muscle strength (Cheah et al., 2009; Merico et al., 2018; Plowman et al., 2016) and respiratory function (Plowman et al., 2018). Preclinical studies showed positive effects of mild-to-moderate endurance training in mouse models of motor neuron disease (Veldink et al., 2003; Kirkinezos et al., 2003; Carreras et al., 2010).
Since the clinical effects of particular types of exercise and their neuroprotective role in ALS have not yet been established, there are no clear recommendations for physical therapy in patients with ALS (EFNS guidelines, 2012).
Beside exercises performed under the care of physiotherapist, patients exercise on their own at home environment. The regularity and intensity of exercise may vary among individuals, depending on the functional status, personal attitude towards physical activity (Baceviciene et al., 2019; Elsworth et al., 2009) and additional benefits including enjoyment and improved well-being (Dishman et al., 1985; Rimmer, 2005).
The aims of the study were (i) to describe the prevalence and pattern of PA in ALS patients, (ii) to explore patients’ attitude towards PA, and (iii) to investigate the relationship between the regular exercises at home environment and the rate of functional decline since the disease onset.
Methods
Patients
Ninety-six patients (f = 51, m = 45) with clinically definite or probable ALS according to the revised El Escorial criteria (Brooks et al., 2000) were enrolled to the study. The data were collected between May 2013 and April 2017 at a single clinical ALS Center. Exclusion criteria included respiratory failure, parenteral feeding and cognitive impairment.
The data was collected at routine out-patient visits: at the baseline (VB) and after 3 months (visit 1, V1) and 6 months (visit 2, V2) from the baseline visit. At each visit, patients were interviewed about the prevalence of PA (regularity and length of physical exercises; prevalent patient’s position during the day: mainly in motion, sitting or lying), their personal attitude towards PA and a subjective efficacy (the perceived effect on the motor performance and mood) by using a short questionnaire (Fig. 1).
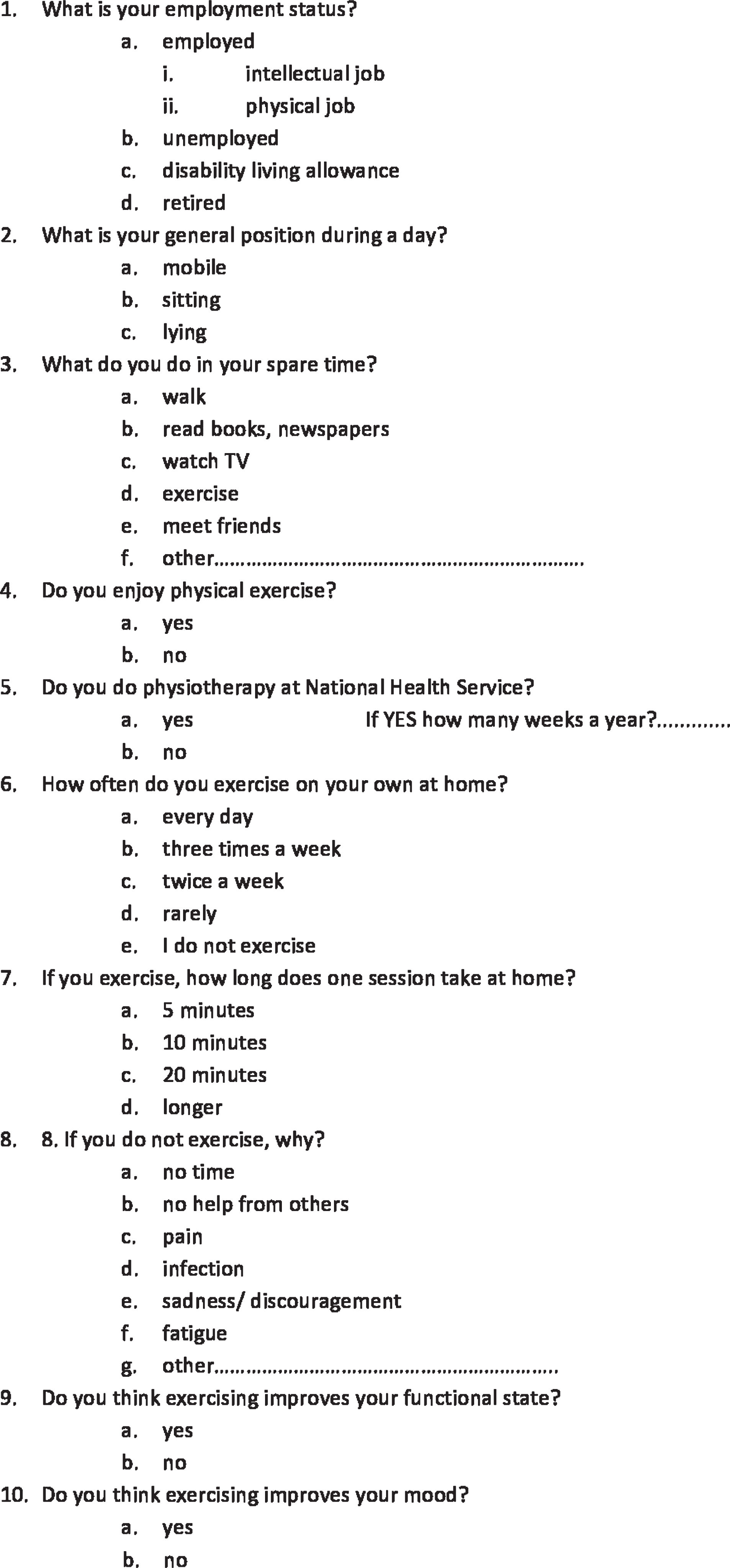
ALS patient’s physical activity questionnaire.
The analysis of clinical parameters included site of disease onset (weakness), disease duration (time from the onset of weakness to the baseline visit) and diagnostic delay (time from the onset of weakness to the diagnosis of ALS). All patients underwent (1) functional assessment with revised ALS Functional Rating Scale (ALSFRS-R) (Cedarbaum et al., 1997), (2) estimation of fatigue with Fatigue Severity Scale (FSS) (Krupp et al., 1989) and (3) muscle strength with (a) Medical Research Council (MRC) (Medical research council memorandum, 1976) and (b) Hand-Held Dynamometry (HDD) (Shefner, 2017).
Regular exercise at home environment (RE) was defined as performing exercises at least 2 times a week. The median decline in the functional scores every three months (ΔALSFRS-R; ΔMRC) was compared between the regularly exercising (RE) and non-exercising (non-RE) group, according to the patient’s declaration in the study questionnaire. The ΔALSFRS-R and ΔMRC were calculated as a difference between the measures on two successive visits, thus reflecting the functional decline over subsequent 3-month-periods.
Non-parametric tests (Mann-Whitney or Kruskal-Wallis tests as appropriate) were employed to perform comparisons between the groups for continuous variables, and the chi-squared test was used for the categorical variables. Spearman’s rank coefficient was applied to test for significant correlations and McNemar’s test to identify the changes in reported attitudes with the disease progression. We used regression models to identify the independent predictors of PA and RE between VB and V1 (a comparison between V1 and V2 was not feasible due to a limited number of patients not performing exercises in the later, n = 2). A p-value of 0.05 was considered for statistical significance. Analyses were performed in SPSS v27.0 software (IBM SPSS Statistics).
Ethical approval
The study was approved by the Ethics Committee (KB/170/2013) and was conducted in accordance with the guidelines of Good Clinical Practice. All patients signed an informed consent form prior to inclusion in the study.
Results
Cohort characterization
At the time of baseline visit (VB), the median age of patients was 61 (interquartile range [IQR], 51–70) with female to male ratio of 1.13. The median total ALSFRS-R and MRC score were 36.0 (IQR, 32.3–41) and 4.2 (IQR, 3.43–4.7), respectively. The ALSFRS-R and MRC did nod differ between the RE and non-RE groups. The median total ALSFRS-R score in the RE group was 35.5 (IQR, 30.0–41.0) and in the non-RE group it was 35.0 (IQR, 32.75–38.25). The median total MRC score was 4.15 (IQR, 3.56–4.66) and 3.9 (IQR, 3.31–4.57), respectively.
Of the 96 patients interviewed at VB, 46 completed the follow-up assessments at 3 months (V1) and 28 at 6 months (V2). Full patients’ characteristics are presented in Table 1.
Demographic and clinical characteristics of patients with amyotrophic lateral sclerosis
Demographic and clinical characteristics of patients with amyotrophic lateral sclerosis
IQR –interquartile range, M –male, F –female.
At the baseline visit, 70.8% (n = 68/96) of the entire group declared to exercise regularly (RE) at home environment. In particular, 60.3% of those patients performed exercise every day and 39.7% ≥2 times per week. Among the functional scores, only the bulbar subscore of ALSFRS-R differed significantly between the RE group and the non-RE group (11.0 [IQR, 9.25, 12.0] vs 9.00 [IQR, 3.5, 10.0], p = 0.011). A dominant body position (mobile, sitting, lying) during the day was related to the functional state (total ALSFRS-R: 39 (IQR, 33–43) vs 35 (IQR, 33.25–38.75) vs 30 (IQR, 24–35), H = 19.641, df = 2, p < 0.001; total MRC: 4.54 (IQR, 4.14–4.77) vs 3.87 (IQR, 3.32–4.6) vs 3.3 (IQR, 2.04–3.82), H = 24.79, df = 2, p < 0.001; total HHD: 26.41 (IQR, 21.04–34.48) vs 16.32 (IQR, 8.44–23.79) vs 9.99 (IQR, 2.89–17.5), H = 18.342, df = 2, p < 0.001, respectively) (Fig. 2a, 2b and 2c) but showed no relation to the prevalence of RE (RE, non-RE) (total ALSFRS-R: 35.5 (IQR, 30–41) vs 35.0 (IQR, 32.75–38.25), U = 763, p = 0.392; total MRC: 4.15 (IQR, 3.56–4.66) vs 3.90 (IQR, 3.31–4.57), U = 838.5, p = 0.829; total HHD: 21.24 (IQR, 10.01–31.27) vs 20.23 (IQR, 9.81–27.67, U = 292.5, p = 0.606) (Fig. 3).
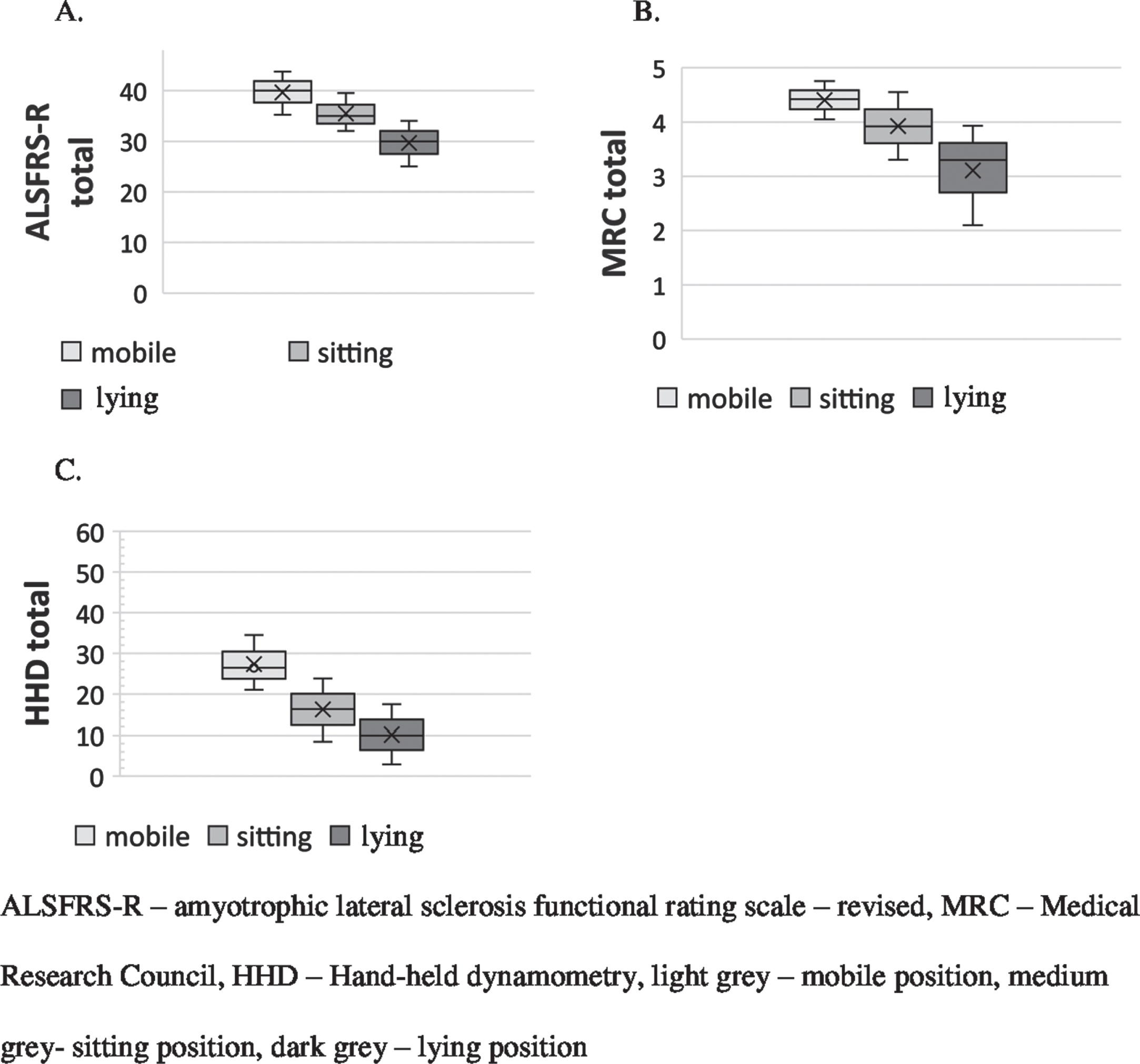
The relationship between the patients’ dominant body position during the day and the functional status (A) and muscle strength (B, C) at the baseline visit.

The relationship between the dominant body position during the day and a prevalence of regular exercises at home environment.
Half of our cohort (50%) attended physical therapy under the care of physiotherapist at outpatient clinics in the public sector. There was a positive association between the participation in physiotherapy at the outpatient clinic and the prevalence of RE (chi2 =5.556, p = 0.018). A weak positive correlation was found between the reported length of exercises at home and the number of weeks since the initiation of the physical therapy at the outpatient clinic (rho = 0.360, p = 0.013).
In the non-RE group (n = 28, 29.2%), the most frequent reasons not to perform regular physical activity included a general discouragement (42.9%), fatigue (25.0%) and lack of willingness to exercise (17.9%). Further 10% of patients declared lack of knowledge of how to perform exercises, while no one indicated disliking physical training.
Among demographic (age, gender) and clinical parameters (site of onset, disease duration, diagnostic delay), multivariate logistic regression model revealed only the bulbar onset as a negative predicting factor for regular exercises at home (odds ratio [OR]: 5.2, 95% confidence interval [CI] 1.71–15.94; p = 0.004); the shorter disease duration and bulbar onset were found as independent negative predictors for attendance to physical therapy at the outpatient clinic (OR: 1.1, 95% CI 1.00–1.15; p = 0.045 and OR: 3.0, 95% CI 1.07–8.42; p = 0.037, respectively).
At baseline interview, 74.0% of patients declared that the regular PA had a beneficial influence on their functional performance and 79.2% –on their mood. There was a higher percentage of positive answers among patients from the RE group considering the functional performance (85.3% vs 46.4%, p < 0.05) and mood (88.2% vs 57.1%, p < 0.05) as compared to the non-RE group. There was no relationship between the above attitudes and the ALSFRS and MRC scores. In addition, these attitudes did not change at follow-up visits (V1 and V2).
Effect of exercise at home environment on motor performance in ALS patients
The median decline in total ALSFRS for the entire study group (n = 45) between the VB and V1 was 2.0 (IQR, 1.0–5.25), and between V1 and V2 (n = 28) 2.0 (IQR, 1.0–5.0). The median decline in MRC score (n = 45) between the VB and V1 was 0.22 (IQR, 0.04–0.52), and between V1 and V2 (n = 28) 0.39 (IQR, 0.17–0.67). The median decline in HHD score (n = 23) between the VB and V1 was 3.56 (IQR, 0.32–6.95), and between V1 and V2 (n = 16) 3.19 (IQR, 0.17–6.54).
After adjustment for gender, age, site of onset, disease duration and diagnosis delay, there was a lower median decline in respiratory sub-score of ALSFRS-R in the RE group compared to the non-RE individuals between VB and V1 (Table 2). In addition, in the entire group of patients, interviewed at V1 and V2, there were inverse correlations between the length of the exercises in the last three months and the decline rate of total ALSFRS-R or MRC score during that period (for full details see Table 3).
Comparison of the functional deterioration between the patients with amyotrophic lateral sclerosis who did and who did not exercise regularly at home environment
Comparison of the functional deterioration between the patients with amyotrophic lateral sclerosis who did and who did not exercise regularly at home environment
adj –adjusted for age, gender, site of onset (bulbar vs limb), diagnosis delay, RE –regular exercise, non-RE –without regular exercise, ALSFRR-R –Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised, MRC –Medical Research Council, UE –upper extremities, LE –lower extremities, Δ (delta) –difference between the measures on the two successive visits, VB –baseline visit, V1 –visit in 3 month, IQR –interquartile range.
Relationship between the length of exercises and the functional deterioration in patients with amyotrophic lateral sclerosis
*p < 0.05, ** p < 0.001. ALSFRS-R –Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised, MRC –Medical Research Council, UE –upper extremities, LE –lower extremities, Δ (delta) –difference between the measures on the two successive visits, VB –baseline visit, V1 –visit in 3 month, V2 –visit in 6 month.
The physical activity of patients with ALS is usually analysed before the onset of disease as a potential risk factor for the development of motor impairment (Visser et al., 2018; Korner et al., 2019). Previous large studies did not show relations between the premorbid physical activity or its intensity and the site of ALS onset (Visser et al., 2018; Korner et al., 2019). Based on the analysis of a declared physical activity after the diagnosis, we have shown that the regular physical exercise is frequent in ALS patients and not related to the general functional status and muscle strength at baseline. We have also found the bulbar onset to be a negative prognostic factor for regular exercise in individuals with ALS. Among possible explanations there is initial sparing of limb muscles, handicapping dysarthria preventing from social contacts and a rapid course of disease with fast development of respiratory involvement (Chio et al., 2002; Testa et al., 2004; Moura et al., 2015; del Aguila et al., 2003; Creemers et al., 2015). Since in the course of the disease, a vast majority of bulbar-onset patients eventually develop limb muscles paresis, it is important to design an individual exercise program adjusted for the functional deterioration and needs of this group of patients.
Our results also show that the willingness to start an exercise program goes beyond the functional status of the patient and includes a personal perception of PA’s impact on the physical performance and mood. Since the physical activity might be related to the QoL (Dunn et al., 2001; Gowans et al., 2001), the personal impression of physical rehabilitation as a beneficial measure might therefore have an influence on ALS patients’ well-being in the course of the disease. Indeed, the majority of our patients perceived exercise as beneficial and home exercising≥2 times a week was more frequent in this group of patients. However, although as many as 75% /79% of patients reported a positive impact of physical therapy on functional performance/mood, at the same time 70% declared to exercise at home on routine bases, and only 39% ≥2 times a week.
The major causes reported by the patients for refraining from regular physical activity included discouragement and fatigue. As a reduced physical activity per se may be related to a decreased mood (Knight, 2012; Abersch et al., 2002; McDonald, 2002), the combination of discouragement and reduced activity may create a ‘vicious circle’ likely to further impair the patient’s wellbeing. It might be even stronger in case of rapid disease progression, which independently contributes to a decreased well-being (Vazquez Medrano et al., 2020). Considering that between 5 and 10% of patients who reported PA to be beneficial did not exercise, and nearly 30% exercised only < 2 per week, there is still a large group of ALS patients that could be encouraged to take up/increase physical activity.
A gradual decrease in ALSFRS-R score and the deterioration of the muscle strength results in postural instability (Krieg et al., 2019), risk of falls (Schell et al., 2019) and patients’ progressive immobilisation (Jette et al., 1999; Sinaki et al., 1978; Bello-Haas et al., 1998; Kloos et al., 2004; Pupillo et al., 2015) leading individuals to change their daily position from mobile, through sitting, into lying. Interestingly, the patients’ position during the day showed no relation to the prevalence of regular exercises.
In our group, the regular physical activity resulted in a slower decline of respiratory subscale of ALSFRS-R after 3 months. The difference was not statistically significant at 6 months, but the result might be due to a small group of patients who attended the V2 follow-up visit and declared no regular PA. Our results confirm previous reports, which showed that PA defined as additional exercises beside the activities of daily living could slow down the functional deterioration in ALS patients (Dory et al., 2001; Clawson et al., 2018; Braga et al., 2018; Dal Bello-Haas et al., 2013). Clawson et al. reported that the resistance, endurance and stretching or range of motion exercises did not negatively influence the functional status of patients with ALS (Clawson et al., 2018). Braga et al. showed that a 6-month program of aerobic exercise performed twice a week slowed down the decline of ALSFRS-R in patients with ALS (n = 24) (Braga et al., 2018). In the course of a 12-month exercise program (n = 14), Drory et al. showed a slower decline in ALSFRS-R after 3 and 6 months of the treatment as compared to the control group (Drory et al., 2001). Similarly, Dal Bello et al. reported higher results of functional scale in stretching/resistance exercise group compared to the stretching group alone (Dal Bello-Haas et al., 2013).
To date there are no reports on the preferred location of the physiotherapy among ALS patients: at specialised out-patient clinics or at home. Only half of our patients exercised in outpatient clinics, but the participation in the supervised training was associated to a higher prevalence of independent physical activity at home. It seems that a referral to the out-patient physical therapy could increase the exercise frequency among ALS patients. Further studies are needed to compare the patients’ satisfaction with physical activity depending on its localization and the impact on the overall well-being.
In our study, even patients exercising regularly in unsupervised home-based training showed less deterioration in the respiratory subscale of ALSFRS-R as compared to patients not exercising in the first three months of observation. Since we did not stratify patients according to disease progression rate, it cannot be excluded that a more aggressive disease course resulted in a lower PA. However, the benefits of unsupervised home training had been previously described by Kitano et al., who reported that patients who exercised at home had even higher respiratory subscale of ALSFRS-R score compared to patients who underwent supervised training (Kitano et al., 2018). In another study, Lunetta et al. reported no difference in ALSFRS-R scores between patients who underwent a 6-month passive stretching exercises at home training and those strictly supervised by the care center (Lunetta et al., 2016). In the study by Braga et al., home exercises subjected to tele-rehabilitation supervision were reported feasible by patients and their caregivers, providing a good compliance (Braga et al., 2018). In our opinion, home exercises can be an interesting solution to the difficulties associated with commuting to rehabilitation centres. In the fast developing telemedicine era (Pinto et al., 2020) the patients can also benefit from remote supervision of a physiotherapist.
In our observation between further consecutive visits, the time of home-based exercise was inversely corelated to ALSFRS-R and MRC deterioration. Patients with greater functional decline spent less time on their own set of exercises. It may be due to worsening of symptoms, fatigue and increasing breathing difficulties and should be considered when planning a long-term exercise program. Our results add to previous reports showing that the more disabled MND patients undertook less activity of daily living (Mioshi et al., 2012).
Limitation
Similarly to other longitudinal studies performed in patients with ALS, the main limitation was a high drop-out rate. However, except for the number of individuals with bulbar onset, the clinical characteristics of the patients did not substantially differ between the visits (Table 1).
Conclusion
The vast majority of ALS patients perform regular physical exercises and find them positively influence their motor performance and mood. Bulbar disease onset, but not functional status, is a negative prognostic factor for regular exercise in individuals with ALS. Regular mild physical activity may result in a slower deterioration of functional status, especially the respiratory function. A referral to out-patient training programs may increase the frequency of physical activity at home.
Footnotes
Acknowledgments
The authors wish to thank the patients and their families for active participation in the study. This work was funded by the JPND (NEEDSinALS; www.NEEDSinALS.com). This is an EU Joint Programme –Neurodegenerative Disease Research (JPND; 01ED1405) project. The project is supported through the following organizations under the aegis of JPND –![]() , e.g. Germany, Bundesministerium für Bildung und Forschung (BMBF, FKZ), Sweden, Vetenskapr å det Sverige, and Poland, Narodowe Centrum Badan i Rozwoju (NCBR).
, e.g. Germany, Bundesministerium für Bildung und Forschung (BMBF, FKZ), Sweden, Vetenskapr å det Sverige, and Poland, Narodowe Centrum Badan i Rozwoju (NCBR).
Conflict of interest
The authors report no conflict of interest.