
Abstract
BACKGROUND:
Ataxia is a clinical syndrome characterized by coordination problems and postural disorders.
OBJECTIVE:
This study aimed to examine the effects of functional trunk training on trunk control and upper limb functions in autosomal recessive hereditary ataxia.
METHODS:
Twenty patients were randomly divided into treatment and control groups. Both groups received trunk stabilization and balance exercises, and the treatment group received additional functional trunk training sessions (3 days/week for 8 weeks). The International Cooperative Ataxia Rating Scale, Trunk Impairment Scale, Modified Functional Reach Test, Nine-Hole Peg Test and Quick-Disabilities of the Arm Shoulder and Hand questionnaire were used for assessments.
RESULTS:
The treatment group showed an increase in the upper limb performance bilaterally, whereas increased performance was seen only in the dominant upper limb in the control group. While the functional reach improved in the anterior-posterior (AP) and medial-lateral (ML) directions in the treatment group, it was improved only in the AP direction in the control group. Also, the mean changes in outcomes were not significantly different between the groups except for modified functional reach test.
CONCLUSIONS:
Functional trunk training may be a more effective method to improve upper limb performance and dynamic trunk balance in autosomal recessive hereditary ataxia.
Introduction
Ataxia is a clinical syndrome with typical symptoms of coordination problems and postural disorders resulting from lesions of the cerebellum and its neural connections (Klockgether & Paulson, 2011). Autosomal recessive ataxias usually have onset in childhood. Friedreich’s ataxia (FA), ataxia telangiectasia (AT), ataxia with vitamin E deficiency, infantile-onset spinocerebellar ataxia, ataxia associated with coenzyme Q10 deficiency, mitochondrial recessive ataxia syndrome and Marinesco-Sjögren syndrome are most common autosomal recessive hereditary ataxias. An invariant manifestation of all of these disorders is progressive limb and trunk ataxia (Fogel & Perlman, 2007).
Trunk control maintains the upright position of the body and postural and corrective reactions during weight transfers. Proper proximal and distal extremity movements are key to ensuring connection between the shoulder and pelvis (Parlak & Yıldırım, 2015). Good trunk control is required to be able to perform many activities of daily living (ADL) such as climbing and descending stairs, walking, sitting, eating and writing. This means that we have to constantly control the position of the whole body to adapt to an ever-changing environment. Muscle strength, muscle endurance, and sensory-motor control are important factors for core stability. Core muscles stabilize the spine and trunk, allowing the head and extremities move freely and perform selective movements smoothly (Sæther & Jørgensen, 2011). Loss of trunk control is associated with impairment of balance, gait and arm and hand functions (Davies, 1990). Although the trunk is commonly affected in patients with neurological disorders, its importance is often neglected in rehabilitation programs (Ryerson, Byl, Brown, Wong, & Hidler, 2008).
Due to limb and trunk ataxia, affected patients experience body oscillations while sitting that become worse in different arm positions, and functional impairment such as difficulties with writing, buttoning clothes or picking up small objects (Ashizawa & Xia, 2016). It is known that degenerative cerebellar ataxias involve the trunk as well as the extremities, leading to changes in extremity motor functions (Ashizawa & Xia, 2016; Naeije, Rovai, Pandolfo, & De Tiège, 2021; Marianne Anke et al., 2011). Although there are many studies in the literature examining the effects of various trunk training exercises on trunk control and upper limb functioning in several disorders, a limited number of studies are available on children with hereditary ataxia, which is a very rare disease with autosomal recessive inheritance, affecting multiple body systems (Arı & Günel, 2017; Peeters, de Groot, & Geurts, 2018; Verheyden et al., 2009). The aim of the current study was to examine the effects of functional trunk training on trunk control and upper extremity functions in children with autosomal recessive hereditary ataxia.
Material and methods
Study design and participants
Twenty-five children who presented to Hasan Kalyoncu University Physiotherapy and Rehabilitation Center between September 2020 and October 2021 and were diagnosed with autosomal recessive hereditary ataxia by a pediatric geneticist were enrolled in the study. Children and their parents who agreed to participate in the study were included in the study after giving assent (for children) and signing informed consent (for parents). The study protocol was approved by the Ethics Committee of Hasan Kalyoncu University Institute of Health Sciences (Approval no. 2020/107).
Children from 5 to 18 years of age who were at least able to sit independently and comprehend simple verbal commands, without any visual, speech or hearing problems that could impair communication, and their parents were included in the study. Patients who underwent surgery to lower and upper extremities within the previous 6 months, those with severe cognitive impairment, and those with unstable medical conditions were excluded.
A total of 5 patients, including 3 patients with an unstable medical condition and 2 patients who could not understand simple verbal commands, were excluded from the study. Twenty children eligible for the study were divided into two groups (n = 10 each) as treatment and control groups using the simple random method (coin flipping). Children in the control group received a routine rehabilitation program consisting of trunk stabilization and balance exercises. Treatment group received a structured rehabilitation program to activate the trunk muscles in accordance with the principles of the Bobath Neurodevelopmental Treatment (NDT) in addition to the routine rehabilitation program.
Physical and demographic characteristics of the patients were recorded at baseline. The International Cooperative Ataxia Rating Scale (ICARS) was used for the assessment of the severity of ataxia, the Trunk Impairment Scale (TIS) to evaluate static and dynamic sitting balance and trunk coordination, Modified Functional Reach Test (MFRT) for the assessment of trunk control, and Nine-Hole Peg Test (NHPT) and Quick Disabilities of the Arm Shoulder and Hand (Q-DASH) questionnaire for the assessment of upper limb functions in both groups at initial and final examinations. All assessments were performed under the same conditions for each patient and lasted for approximately 45 minutes. Final assessments were conducted at the end of the 8-week rehabilitation program.
Assessments
International cooperative ataxia rating scale (ICARS)
The ICARS is recommended as a reliable and valid tool for the assessment of patients with ataxia. It consists of 4 subscales including posture and gait disturbances, kinetic function, speech disorders and oculomotor disorders. Total possible scores range from 0 to 100. Higher scores indicate greater impairment. Objective assessment of coordination has been challenging due to inadequacy of the conventional scales used in the clinical setting and requirement for very expensive technological systems. ICARS is an objective test method which was developed to overcome these shortcomings and is widely used today for the assessment of patients with degenerative ataxias associated with different pathologies (Schoch et al., 2007).
Trunk impairment scale (TIS)
The TIS is a valid and reliable scale for the evaluation of trunk performance in cerebral palsy and neuromuscular disorders (Demir & Yıldırım, 2018). It is used to assess functional strength of the trunk, postural control and quality of body movements. The TIS consists of three subscales (static, dynamic and coordination) with a total of 17 items, including 3 items for static balance, 10 items for dynamic balance and 4 items for the coordination ability of the stabilizer muscles. The total TIS score ranges from 0 (minimal performance) to 23 (perfect performance). Higher scores indicate better trunk control (Verheyden et al., 2004).
Nine-hole peg test (NHPT)
The NHPT is commonly used in the clinical setting for the measurement of upper limb functions (hand, arm) and motor speed. It consists of 9 wooden pegs (diameter 9 mm) and a standard wooden board with 9 holes (diameter 10 mm). For the test, the patient is asked to take the pegs from the container one by one and place them into the holes on the board as quickly as possible and then remove the pegs from the holes one by one. The stopwatch is started from the moment the first peg is taken until the moment the last peg is put back in the container. The time elapsed between the placement and removal of the pegs is recorded in seconds (Cohen et al., 2001; Mathiowetz, Weber, Kashman, & Volland, 1985).
Quick disabilities of the arm, shoulder and hand (Q-DASH)
Q-DASH is a questionnaire that assesses limitations in activity and participation in all upper extremity problems. Reliability and validity of the Turkish version were demonstrated by Düger et al (Düger et al., 2006). Q-DASH consists of 11 questions that quantitatively assess the amount of difficulties an individual experiences when performing activities of daily living due to upper limb disability. Each item has 5 response options and scale scores are calculated from the item scores ranging from 0 to 100 (0 = no disability, 100 = completely disabled) (Angst, Schwyzer, Aeschlimann, Simmen, & Goldhahn, 2011; Ayhan, Ünal, & Yakut, 2010). Higher scores denote a greater level of disability.
Modified functional reach test (MFRT)
The modified functional reach test was developed by Lynch et al. to assess dynamic balance of the trunk. It measures the distance to reach forward and to the sides in sitting position without loss of balance (Lynch, Leahy, & Barker, 1998). The distance covered in each direction is recorded in centimeters.
Study interventions
The treatment group received routine trunk stabilization training for 2 days a week and functional trunk training once a week, and control group received routine trunk stabilization training for 3 days for a total of 8 weeks.
The rehabilitation program was structured as follows:
1-Trunk stabilization exercises
Bridging Unilateral limb extension in bridging position Arm and leg extension in crawling position Planks Trunk strengthening exercises Sit-ups Cross sit-ups Reverse sit-ups Lower abdomen strengthening exercise (the hundred exercises) Hip abduction in side lying and supine positions Hip extension in prone position
2-Trunk balance exercises
Weight transfer to left and right in sitting position Balance training in different extremity positions Balance training while sitting on balance discs Balance training on an exercise ball
3-Functional trunk training
Functional reaching with trunk elongation in different sitting positions (rider position, hip and knee extended 90 degrees, sitting with legs extended) Trunk control exercises with ball in sitting position Pelvic control in line with Bobath concept Strengthening of the abdominal muscles in the shortened position according to the Bobath concept Facilitation of trunk extension and elongation using rollers in prone position Functional activities with trunk extension on balance ball in prone position Trunk rotation
Examples of some exercises are shown in Fig. 1 below.
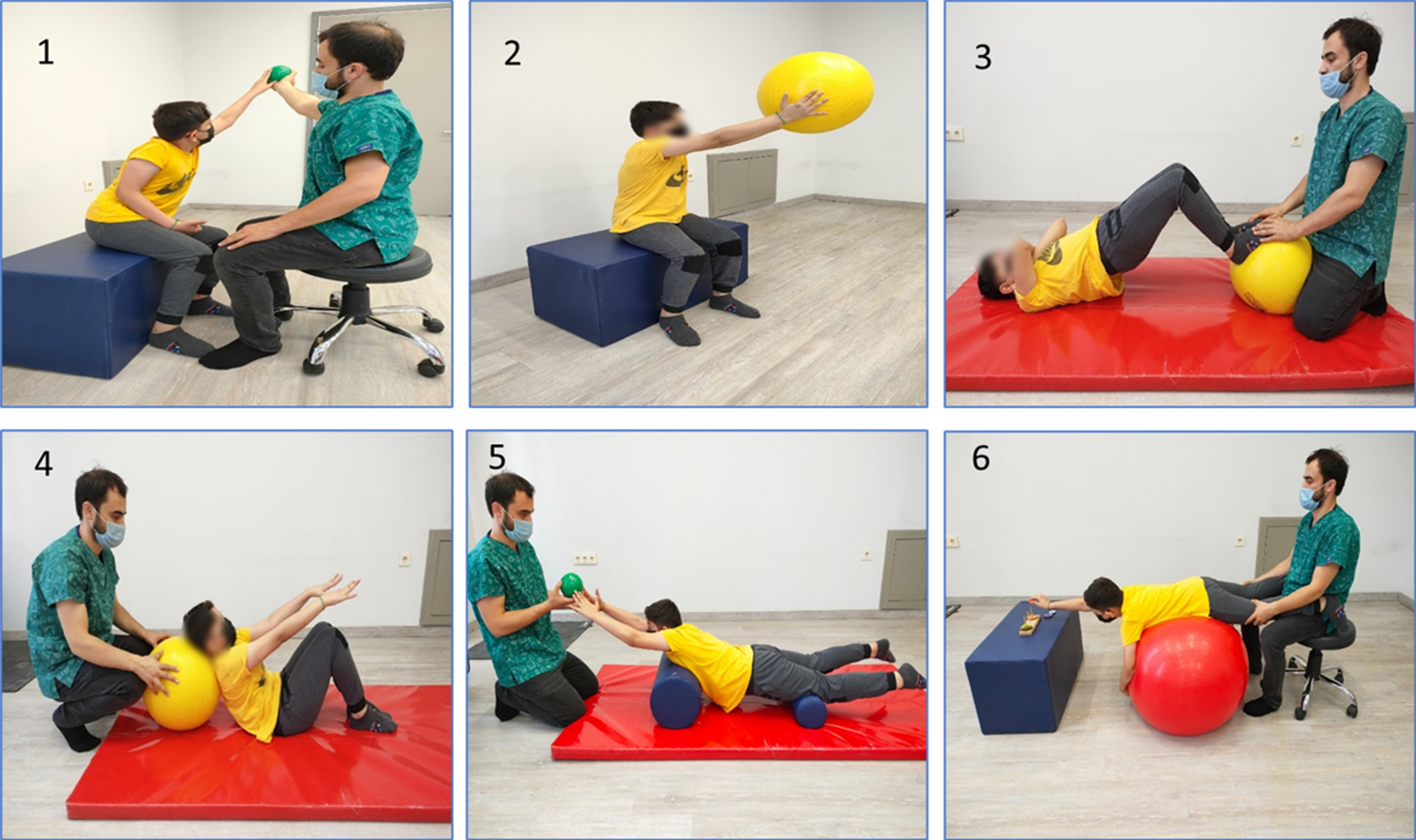
Some examples of functional trunk training exercises. 1. Functional reach exercises with diagonal patterns in different sitting positions (normal, rider and leg extended positions) 2. Bilateral upper extremity exercises with Swiss ball for trunk control 3. Pelvic control on the Swiss ball based on the Bobath concept 4. Strengthening of the abdominal muscles in the shortened position according to the Bobath concept 5. Facilitation of trunk extension and elongation using rollers in prone position 6. Functional reach exercises with hand activities on Swiss ball in prone position.
Statistical analyses were performed using SPSS (Statistical Package for the Social Sciences) version 22.0 (IBM, Armonk, NY, USA). For descriptive analysis of the study data, continuous variables were expressed as arithmetic mean and standard deviation (X±SD), and frequency values were calculated as percentage (%) for categorical variables. The Kolmogorov-Smirnov test was used to check the normality of data distribution. Mann-Whitney U test was employed for comparison of non-normally distributed data between the groups and Wilcoxon signed-rank test for comparison of pre/post-treatment data within a group. A p value less than 0.05 was considered statistically significant. The power of the study was found to be 87% for d > 1.00, based on the AP functional reach data.
Results
There were 10 patients each in the treatment group (5 girls and 5 boys) and control group (6 girls and 4 boys). Among 16 families participating in the study, 9 families had sibling history of ataxia. The dominant side was the right side in all patients. None of the children discontinued the training program during the study. Of the children, 5 had Friedreich’s ataxia, 8 had ataxia telangiectasia, 2 had ataxia associated with coenzyme Q10 deficiency, 2 had Charlevoix-Saguenay spastic ataxia, 1 had CONDSIAS (stress-induced childhood-onset neurodegeneration with variable ataxia and seizures), 1 had mitochondrial complex III deficiency-related ataxia and CALFAN (low γ-glutamyl-transferase cholestasis, acute liver failure, and neurodegeneration) syndrome.
The study groups showed a homogeneous distribution in terms of age, height, body weight and body mass index (BMI), with no significant difference between the groups (p > 0.05). (Table 1)
Physical characteristics of the study sample
Physical characteristics of the study sample
*p < 0.05, Abbreviations; BMI: Body mass index, X±SD: Mean±Standard deviation, min: minimum, max: maximum, kg: kilogram, m2: square meter.
Significant changes were found in ICARST (total score), ICARS1 (posture and gait disturbances) and ICARS2 (kinetic function) scores in the treatment group, and ICARST and ICARS2 scores in the control group (p < 0.05). There were no significant differences in ICARS3 (speech disorders) and ICARS4 (oculomotor disturbances) scores in both groups (p > 0.05). The mean changes in ICARST, ICARS1, ICARS2, ICARS3 and ICARS4 were similar between the groups (p > 0.05). (Table 2)
Comparison of the ICARS scores within- and between groups
*p < 0.05, Abbreviations; Pre-t: Pre-test, Post-t: Post-test, ICARST: International Cooperative Ataxia Rating Scale Total Score, ICARS1: Posture and Gait Disturbances, ICARS2: Kinetic Function, ICARS3: Speech Disorders, ICARS4: Oculomotor Disorders.
Significant changes were found in TIST (total score), TIS1 (static sitting balance) and TIS2 (dynamic sitting balance) scores within the treatment group and TIST and TIS2 scores within the control group (p < 0.05). However, the mean changes in TIST, TIS1, TIS2 and TIS3 were similar between the groups (p > 0.05). Significant differences were found in AP (anterior-posterior) and ML (medial-lateral) measurements in the treatment group and only in AP measurement in the control group (p < 0.05). The mean changes in the AP and ML scores were greater in the treatment group compared to the control group (p < 0.05). (Table 3)
Comparison of the TIS and MFRT scores within- and between groups
*p < 0.05, Abbreviations; Pre-t: Pre-test, Post-t: Post-test, TIST: Trunk Impairment Scale Total Score, TIS1: Static sitting balance, TIS2: Dynamic sitting balance, TIS3: Coordination, MFRT: Modified Functional Reach Test, AP: Anterior-posterior, ML: Medial-lateral, cm: centimeter.
Significant differences were found in the NHPT completion time for the right and left hands and Q-DASH score in the treatment group (p < 0.05). The NHPT completion time for the right hand as well as Q- DASH score improved in the control group (p < 0.05). The mean changes in NHPT and Q-DASH were similar between the groups (p > 0.05). (Table 4)
Comparison of the Q-DASH and NHPT scores within- and between groups
*p < 0.05, Abbreviations; Pre-t: Pre-test, Post-t: Post-test, NHPT: Nine-Hole Peg Test, Q-DASH: Quick Disabilities of the Arm Shoulder and Hand, cm: centimeter, sec: second.
Our study highlights the importance of trunk control training in patients with autosomal recessive cerebellar ataxia and this is relevant considering the effect of trunk control on upper limb functionality. Eight weeks of functional trunk training and routine stabilization training provided improvements in trunk control and upper limb functions. Thus, it is possible to improve dynamic balance of the trunk in AP and ML directions, static balance as well as motor performance of the non-dominant hand through functional trunk training.
Although the training programs used in our study produced a similar improvement in ICARST, ICARS1 improved only in the treatment group, which may be related to the higher number of patients with the ability to walk independently and lower level of oculomotor involvement in the treatment group. Many studies have shown that oculomotor disorders affect many aspects of gait kinematics such as gait speed, cadence, stride length, duration of stance phase, the position of the extremity in swing phase and upper trunk stability (Cromwell, Newton, & Forrest, 2002; Wuehr et al., 2013). Comparable effects of both training programs on kinetic function (ICARS2) as observed in the present study may be related to the goal of our rehabilitation program, which focused only on the trunk. The ICARS2 subscale primarily assesses rhythmic movements of upper and lower extremities and coordination. This may also be due to the fact that our functional trunk training program involved diagonal pattern training and did not include coordination exercises specifically designed for upper extremities. The lack of improvement in ICARS3 and ICARS4 scores in both groups may be related to the absence of tailored exercises for speech and oculomotor disorders in our training programs. Previous studies on the outcomes of several trunk training exercises in ataxic patients with multiple sclerosis (MS) reported similar changes in ICARS scores, which are consistent with our findings (Salcı et al.,2017; Keser, Kirdi, Meric, Kurne, & Karabudak, 2013). In a study investigating the effectiveness of a rehabilitation program that focused on general physical condition, specific physical condition and functional training, all ICARS subscales improved except for oculomotor disorders (Jorge-Rodríguez, Fernández-Martínez, Pérez, Peralta-Flores, & Bergado, 2013).
In our study, although TIST and TIS2 scores improved in both groups, mean changes in these parameters were similar. The improvement of TIS1 scores only in the treatment group despite similar improvements in TIST scores in both groups may be attributed to more severe trunk involvement in the treatment group versus control group. On the other hand, the lack of any changes in TIS3 score in both groups may be associated with the absence of coordination-specific exercises in our rehabilitation programs. In line with our results, the trunk exercise program applied to stroke patients was found to improve TIS2 and TIST scores but not TIS3 scores (Kılınç et al., 2016). It was formerly reported that trunk exercises are particularly effective for improvement of TIS2 subscale scores in stroke patients (Alhwoaimel et al., 2018). In a study by Keser et al. (Keser, Kirdi, Meric, Kurne, & Karabudak, 2013) comparing a routine neurorehabilitation program with trunk exercises based on the Bobath concept in MS patients, improvements were observed in both TIST and all subscale scores. However, there was no substantial difference between the two treatment approaches.
The treatment group showed improvements in the mean changes in AP and ML scores. Improved functional reach in the treatment group may be explained by the inclusion of functional multidirectional reach movements in the functional trunk training. It has been reported that NDT-based trunk training approach is more effective that the conservative rehabilitation approach in improving postural control and functional reach in sitting position in children with cerebral palsy (Ramya, Kumari, & Madh, 2013). In a study by Kılınç et al. (Kılınç et al., 2016) examining the effectiveness of Bobath-based trunk training for trunk control, an improvement was observed in the functional reach distances of the patients at the end of the treatment. In another study investigating the effects of different trunk exercises on ataxia in MS patients, increased functional reach distances were seen in the groups receiving lumbar stabilization and task-oriented exercise training (Salcı et al., 2017). In the aforementioned studies, dynamic trunk balance was evaluated only in the AP direction. In contrast, trunk balance was assessed in both ML and AP directions in the current study, which is an important addition to literature data.
Trunk control is considered as a prerequisite for upper limb and hand functions (Gillen, Boiangiu, Neuman, Reinstein, & Schaap, 2007). Upper limb performance is related to physical parameters such as age and sex. Compared to healthy children of the same age, the time to complete NHPT was approximately 3 times longer in ataxic children in our study (Wang, Bohannon, Kapellusch, Garg, & Gershon, 2015). While upper limb performance improved bilaterally in the treatment group receiving functional trunk training, improved performance was seen only in the dominant upper limb (right hand) in the control group. We think that the observed improvement of limb performance bilaterally in the treatment group may be related to the inclusion of multidirectional reach movements and exercises that facilitate performance of ADL in the functional trunk training program. There are a number of hypotheses in the literature about the motor control of the dominant and non-dominant hand. These hypotheses suggest that the dominant hand has a higher capacity to process neural feedback and is more effective in segmental control than the non-dominant hand. During activity, the dominant hand is less affected by the torque forces outside the joint where the movement occurs. In addition, the dominant hand has a greater percentage of fatigue-resistant type I muscle fibers than the non-dominant hand. However, motor skills of the non-dominant hand can be improved through various trainings (Heuer, 2007; Shalabi, 2020). The lack of improvement in the performance of the left (non-dominant) hand might be explained by neurological factors discussed above. Similarly, task-oriented exercise training did not improve the performance of the non-dominant hand in children with athetoid cerebral palsy (Naz, Shabbir, & Arshad, 2021). In a case series study in children with congenital upper extremity motor deficits, virtual reality training improved the performance of the dominant hand to a greater extent compared to the non-dominant hand (Wille et al., 2009). We believe that clinicians should include non-dominant extremity-specific exercises in their training programs in order to achieve improvement in non-dominant hand performance.
It was reported that the DASH tool which is frequently used in orthopedic injuries can also be used in neuromuscular disorders (Torres, Moxley, & Griggs, 1983; Kılınç, Yildirim, & Kayihan, 2013). Q-DASH was used in our study to evaluate the functional status of upper extremities. At the end of the intervention, an improvement was noted in Q-DASH scores in both groups in the present study but the mean change was not different between the groups. There are some studies in the literature that demonstrated the impact of the NDT approach on upper limb functions in children (Acar, Altun, Yurdalan, & Polat, 2016). Improved upper limb functionality was reported in a study examining the effects of NDT in children with cerebral palsy (Tekin, Kavlak, Cavlak, & Altug, 2018). Bobath-based trunk training was shown to provide an improvement in upper limb functions in a number of neurological diseases including stroke and MS. However, in line with our findings, Bobath-based trunk exercises were not found to be superior over conventional training (Keser, Kirdi, Meric, Kurne, & Karabudak, 2013; Kılınç et al., 2016).
Study limitations
The activation of core muscles and physical parameters such as strength and endurance might have been evaluated to better demonstrate the improvement in trunk control. Our study included patients who were able to sit independently and walk with or without assistance. Since some of the patients were unable to stand independently, functional reach test was performed in sitting position for all subjects. We might have better analyzed improvement in patients if we could construct a homogeneous study group by recruiting patients with the same level of mobility, instead of a mixed population. Assessments and treatment approaches could be tailored to individual patient needs and this might have produced more effective outcomes in a patient population with a rare disease.
Conclusion
Functional trunk training can be used as a supportive treatment method to improve trunk control and upper extremity functionality in patients with hereditary ataxia with multisystem involvement. Functional trunk training can be preferred to improve the static and dynamic balance of the trunk. In addition to the dominant hand, motor performance of the non-dominant hand can also be improved with functional trunk training.
Footnotes
Acknowledgments
The authors wish to thank physiotherapist Deniz Pala, Tuba Gün and Esranur Narin for their contribution.
Author contributions
S.Y: Conception and design, writing, editing and final approval of the manuscript, drafting the manuscript. S.U: Critical review of the manuscript. H.M.A: Data collection, diagnosis of the participants. P.P.Y: Data collection, critical review of the manuscript. YY: Statistical analysis of data.
Conflict of interest
The authors declare no potential conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.