
Abstract
BACKGROUND:
Recent research recommends physical exercise rather than rest following a mild traumatic brain injury (mTBI).
OBJECTIVE:
To determine the effect of physical exercise on persistent symptoms in people with mTBI.
METHODS:
A search of randomized controlled trials was conducted in CINAHL, Cochrane Library, EMBASE, MEDLINE, SportDiscus and Web of Science, from 2010 to January 2021. Studies were included if they described the effects of a physical exercise intervention in people with mTBI on persistent symptoms. Study quality, intervention reporting, and confidence in review findings were assessed with the CASP, TIDieR and GRADE respectively.
RESULTS:
11 eligible studies were identified for inclusion. Study interventions broadly comprised of two categories of physical exercise, i.e., aerobic (n = 8) and vestibular (n = 3). A meta-analysis (n = 3) revealed the aerobic exercise group improvement was significantly larger compared to the usual care group –0.39 (95% CI: –0.73 to –0.05, p = 0.03). Only three studies using vestibular exercise reported on persistent symptoms and yielded mixed results.
CONCLUSIONS:
This study demonstrated that the use of aerobic exercise is supported by mixed quality evidence and moderate certainty of evidence, yet there is limited evidence for the use of vestibular exercise for improving persistent symptoms in people with mTBI.
Introduction
The terminologies, ‘concussion’ and ‘mild traumatic brain injury’ (mTBI) are often used interchangeably, as they are both described as “an acute neurophysiological event related to blunt impact or other mechanical energy applied to the head, neck or body (with transmitting forces to the brain)” (Ontario Neurotrauma Foundation, 2018). The clinical manifestations of a traumatic brain injury (TBI) are attributed to the pattern and extent of damage from an external force with the severity of TBI categorized as being mild, moderate, or severe (Maas et al., 2017). Approximately 55.9-million people worldwide are estimated to suffer from a mTBI each year (Dewan et al., 2018). Although this represents 81% of all TBIs, this may still be an underrepresentation, as people with mTBI may not seek medical attention (Dewan et al., 2018).
Following a mTBI, an array of somatic, cognitive, physical, and behavioural symptoms may arise (McCrory et al., 2017). The most commonly reported symptoms in the first 12-weeks include headache, dizziness, poor attention, poor memory, irritability and depression (Levin et al., 2015). The extent of these symptoms is influenced by psychological and physiological factors (McCrory et al., 2017), complications of the TBI itself, past medical history and current comorbidities (Marshall et al., 2015). This collection of non-specific post-traumatic symptoms is commonly identified as Post-Concussion Syndrome (McIntyre et al., 2020), Post-Concussion Disorder (Ellis et al., 2015), or Persistent Symptoms (Makdissi et al., 2013). The use of these terms is ambiguous due to the complexities with, and inconsistent use of, diagnostic criteria, including experienced symptoms, their onset and duration (Dwyer, & Katz, 2018).
Most people with mTBI recover spontaneously but up to 30% (Babcock et al., 2013) of people continue to experience persistent symptoms beyond the expected timeframe of 10-days with children recovering slower (Makdissi et al., 2013; McCrory et al., 2017). Traditionally, a physical and cognitive rest period, as well as activity restriction, has been prescribed as treatment for people with mTBI (Leddy et al., 2012; McCrory, 2017) to ease discomfort, and to prevent repeated injury and exacerbation of symptoms (McCrory et al., 2013; McCrory, 2017), without consensus on optimal duration (Leddy et al., 2012; McCrory et al., 2013). There is evidence to suggest that prolonged rest can lead to secondary complications such as deconditioning, anxiety, depression, and irritability; all of which are commonly reported symptoms following a mTBI (Schneider et al., 2017). The latest consensus statement and guidelines recommend that following a brief rest period during the acute phase (24–48-hours) of recovery, people with mTBI should be encouraged to become gradually more active while staying below their cognitive and physical exacerbation threshold (McCrory et al., 2017; Ontario Neurotrauma Foundation, 2018).
Recent systematic reviews have found preliminary evidence for the effectiveness of physical exercise on improving persistent symptoms. However, these reviews were restricted to one type of exercise only (Lal et al., 2018; McIntyre et al., 2020), adolescents (Henke et al., 2020), sport-related injuries (Henke et al., 2020), interventions at least three weeks to three months post-injury (Lal et al., 2018; McIntyre et al., 2020), and included all types of study designs (Henke et al., 2020; Lal et al., 2018; McIntyre et al., 2020), thereby incorporating low level evidence due to including studies without a comparison group, increasing risk of bias. This systematic review aims to address these issues by reviewing the effect of any type of physical exercise on persistent symptoms in people who have experienced a mTBI, without limitations with regards to age, injury cause, or time since injury, while only including level 2 evidence from randomized controlled trials (RCTs).
Methods
This systematic review was completed and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021). The protocol is registered with PROSPERO, International Prospective Register for Systematic Reviews (CRD4201913703) (Centre for Reviews and Dissemination, n.d.).
Literature search and selection criteria
CINAHL, Cochrane Library, EMBASE, MEDLINE, SPORTDiscus, and Web of Science were searched using a combination of Medical Subject Headings and keywords for mTBI, concussion, post-concussion syndrome, exercise and RCTs. The search was restricted to the English language, human trials, and articles published between 2010 to the 13th of January 2021 to update the current literature. Reference lists of included studies and relevant reviews were searched for additional articles. The search strategy is detailed in Supplementary Table 1.
The study population included people diagnosed with a mTBI. Studies that referred to their study population as those having experienced a mTBI, mild-to-moderate TBI, concussion, or post-concussion syndrome were considered eligible for inclusion. Studies including people with only moderate or moderate-to-severe TBI and mixed populations were excluded. The study intervention type involved physical exercise interventions (e.g., cycling, running) regardless of delivery mode and setting, and the comparator intervention included usual care (e.g., educational, multidisciplinary therapy), or other physical intervention (e.g., stretching, relaxation). There were no limitations regarding the study population or intervention, to capture all studies that investigated exercise for people with a mTBI. The primary study outcome was experienced persistent symptoms, defined as any symptoms experienced following a mTBI. All other reported clinical outcomes were considered as secondary study outcomes.
Data were extracted using a pro-forma that included the following outcomes: study characteristics (sample size, setting); participants’ characteristics (age, time since injury, gender, cause of injury), intervention characteristics (type, key descriptors, intensity, time, frequency, duration); and reported outcomes (key findings, between-group means, 95% CIs, effect sizes). Data of all studies was extracted by author one. A second author independently checked for accuracy and extracted data from 20% of the included studies demonstrating an agreement of more than 80% (Shea et al., 2017).
A narrative synthesis was conducted for all data. Standard mean differences and 95% CIs were used to analyse continuous data. Due to the heterogeneity of the available data, a meta-analysis, performed using the Review Manager 5.3 software (Cochrane, 2014), was possible only to calculate the effect size of aerobic exercise using the change in persistent symptoms from immediately pre to post for aerobic exercise intervention compared to usual care.
Quality assessment
A risk of bias assessment was completed using a modified version of the Critical Appraisal Skills Program (CASP) (Critical Appraisal Skills Programme, 2018). Studies scoring≤3/6, 4/6, or ≥5/6 were judged of low, moderate, or high quality respectively. CASP items deemed as critical value included appropriateness of randomisation and blinding, whether groups were treated equally, whether participants were lost to follow-up, and the amount of detail provided for the population, intervention, and comparator. To assess the completeness of intervention reporting, the Template for Intervention Description and Replication (TIDieR) was used (Hoffmann et al., 2014). Quality of evidence was assessed using the Grade of Recommendation, Development and Evaluation (GRADE) tool based on risk of bias, inconsistency, indirectness, imprecision, and publication bias (GRADEpro GDT, 2020). Due to the heterogeneity of the available study data, analysis with GRADEpro GDT could only be undertaken for those studies that were included in the meta-analysis (GRADEpro GDT, 2020).
Results
Search results and study characteristics
A flowchart depicting the study selection process is presented in Fig. 1. Of the 11,083 citations retrieved in the systematic search, 96 studies were reviewed in full-text of which 11 met the inclusion criteria and reported the effect of an exercise intervention on persistent symptoms in people with mTBI (Bailey et al., 2019; Chan et al., 2018; Dobney et al., 2020; Kleffelgaard et al., 2019; Kurowski et al., 2017; Leddy et al., 2019; Maerlender et al., 2015; Micay et al., 2018; Reneker et al., 2017; Rytter et al., 2019; Schneider et al., 2014). Six studies reported on a population aged 18-years old or under (Bailey et al., 2019; Chan et al., 2018; Dobney et al., 2020; Kurowski et al., 2017; Leddy et al., 2019; Micay et al., 2018). Time since injury ranged from five days (Micay et al., 2018) to six months post-injury (Rytter et al., 2019), and one study did not specify (Maerlender et al., 2015). Cause of injury included sport-related injuries (Chan et al., 2018; Leddy et al., 2019; Maerlender et al., 2015; Micay et al., 2018; Reneker et al., 2017; Schneider et al., 2014), mixed aetiologies (Bailey et al., 2019; Kleffelgaard et al., 2019; Kurowski et al., 2017; Rytter et al., 2019), and one did not specify (Dobney et al., 2020). The sample size ranged from 15 (Micay et al., 2018) to 113 (Leddy et al., 2019) and the total number of participants included in this review was 467 (see Table 1, Study characteristics).
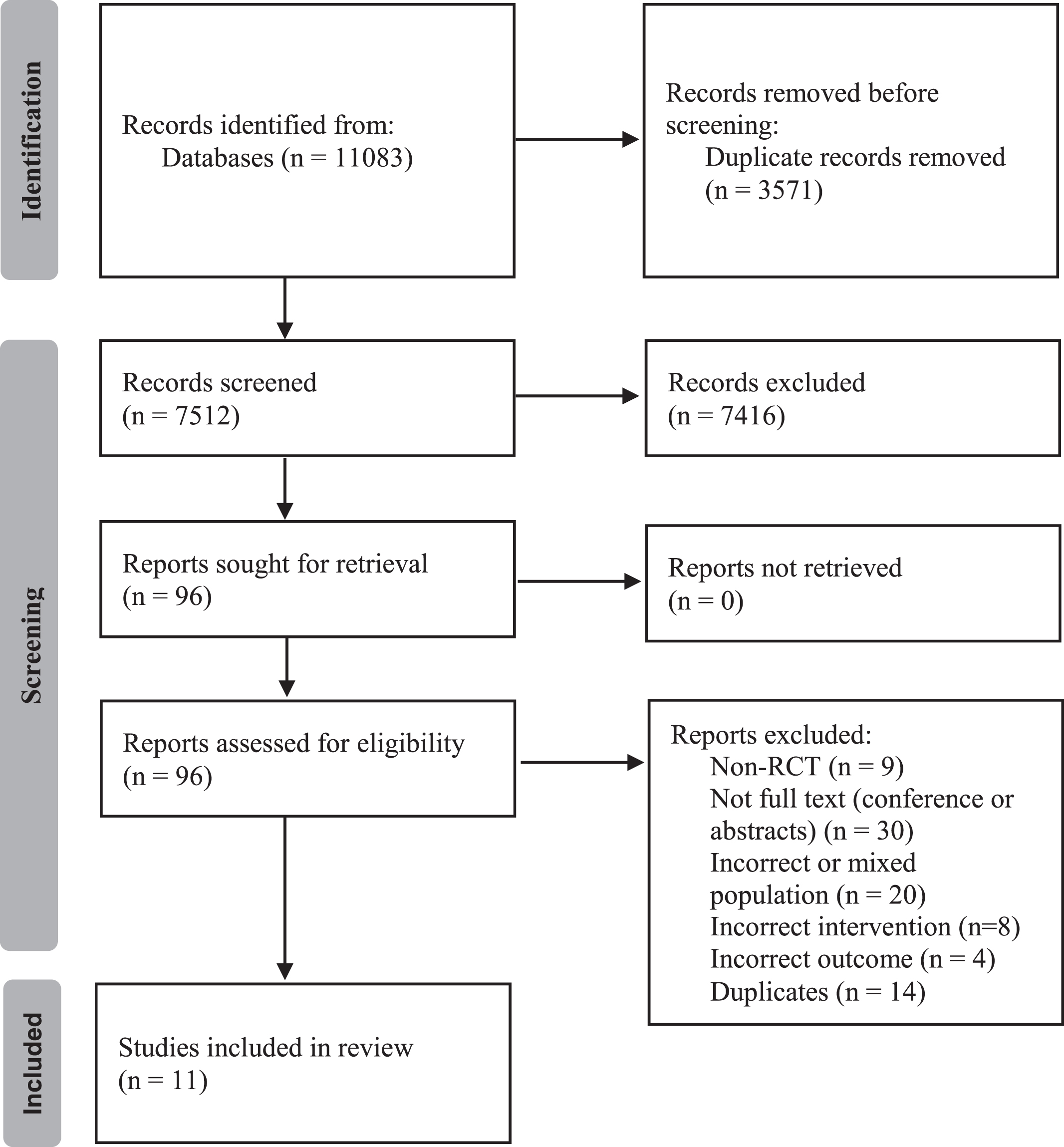
PRISMA flow diagram.
Two studies were rated low (Bailey et al., 2019; Maerlender et al., 2015), four medium (Chan et al., 2018; Dobney et al, 2020; Kleffelgaard et al., 2019; Kurowski et al., 2017) and five were rated as high (Leddy et al., 2019; Micay et al., 2018; Reneker et al., 2017; Rytter et al., 2019; Schneider et al., 2014) quality (see Table 1 for CASP score and Supplementary Table 2 for the full details of the CASP assessment).
Assessment of intervention reporting using the TIDieR checklist indicated that all studies provided a rationale for the intervention and outlined the intervention procedures. Most studies also appropriately described the mode of intervention delivery (9/11), where the intervention occurred (8/11) and intervention dosage (10/11). Only 3/11 studies provided sufficient information about the intervention provider (see Supplementary Table 3 for the full TIDieR assessment).
A summary of the key findings using the GRADE assessment for the studies included in the meta-analysis are provide in Table 3. Certainty of evidence for the effect of aerobic exercise intervention on persistent symptoms was moderate, and risk of bias was serious due to one study having inadequate blinding (Chan et al., 2018; Maerlender et al., 2015; Rytter et al., 2019).
Study characteristics
Study characteristics
Intervention characteristics
IG = Intervention group. CG = Control group
GRADE for aerobic exercise compared to usual care for people with mTBI. Authors: Chan et al. (2018); and Rytter et al. (2019)
CI: Confidence interval; SMD: Standardised mean difference. a. One study had inadequate blinding and follow-up of patients.
All 11 included studies reported on the effect of exercise on persistent symptoms. Five studies compared a physical exercise intervention, all involving aerobic exercise, to usual care (Chan et al., 2018; Dobney et al., 2020; Maerlender et al., 2015; Micay et al., 2018; Rytter et al., 2019). A total of six studies compared an exercise intervention to another physical intervention, of these three compared an aerobic exercise intervention to another physical intervention (Bailey et al., 2019; Kurowski et al., 2017; Leddy et al., 2019), and three compared a vestibular exercise intervention to another physical intervention (Kleffelgaard et al., 2019; Reneker et al., 2017; Schneider et al., 2014). Five of the 11 studies reported a positive effect on persistent symptoms in favour of the physical exercise intervention (Bailey et al., 2019; Kurowski et al., 2017; Leddy et al., 2019; Reneker et al., 2017; Rytter et al., 2019), five reported no significant between-group differences (Chan et al., 2018; Kleffelgaard et al., 2019; Maerlender et al., 2015; Micay et al., 2018; Schneider et al., 2014), and one provided descriptive data with no statistical analysis (Dobney et al., 2020). A summary of the intervention characteristics is provided in Table 2. A meta-analysis of three studies comparing physical exercise intervention, all aerobic exercise, to usual care (Chan et al., 2018; Maerlender et al., 2015; Rytter et al., 2019), was possible and is presented in Fig. 2.

Effects of aerobic exercise on persistent symptoms.
Aerobic exercise versus usual care: All five studies assessing the effect of a physical exercise intervention on persistent symptoms, when compared to usual care, used an aerobic exercise intervention (Chan et al., 2018; Dobney et al., 2020; Maerlender et al., 2015; Micay et al., 2018; Rytter et al., 2019). Only one study utilizing a 22-week aerobic and strength program reported significant improvement on the Rivermead score for the intervention group compared to the usual care group (p = 0.013, ES = 0.29) in an adult population of mixed aetiology who were greater than 10-days post-injury (Rytter et al., 2019).
Of the other four studies that did not find a significant effect of aerobic exercise intervention compared to usual care, two studies utilized a stationary cycling program (Maerlender et al., 2015; Micay et al., 2018). One studied a cohort aged 18-years or under who suffered a sports injury and received an 11-day intervention, initiated earlier than 10-days post-injury, and reported on the Post-Concussion Symptom Scale (Micay et al., 2018). The other studied a cohort of unreported ages, with unreported time since a sport-related injury, and an intervention of unreported duration, and reported on the Immediate Post-Concussion Assessment and Cognitive Test (Maerlender et al., 2015).
Finally, the last two studies utilized a treadmill or stationary bike based intervention in those aged 18-years or under beginning at least 10-days post-injury (Chan et al., 2018; Dobney et al., 2020). One study only reported descriptive data for aerobic exercise compared to a delayed start usual care group at the 2-week intervention stage, 4-weeks post-injury, suggesting improvements with exercise on the Post-Concussion Symptom Inventory with no statistical analysis performed (Dobney et al., 2020). The other second study assessed the effects of a 6-week intervention, however, failed to demonstrate an interaction effect of group by time on the Post-Concussion Symptom Scale (Chan et al., 2018).
Three of the five studies provided sufficient information to be included in a meta-analysis comparing aerobic exercise to usual care (Chan et al., 2018; Maerlender et al., 2015; Rytter et al., 2019). The results demonstrated a statistically significant improvement in persistent symptoms due to physical exercise intervention (SMD –0.39, 95% CI: –0.73 to –0.05, p = 0.03) when compared with usual care (Fig. 2). The other two studies were not included in the meta-analysis because they reported data only after a follow-up period (Micay et al., 2018) or did not report mean and SD results (Dobney et al., 2020).
Comparison 2: Physical exercise intervention versus other physical intervention
Aerobic exercise versus other physical intervention: Three studies compared the effect of aerobic exercise, on a bike (Kurowski et al., 2017), treadmill (Bailey et al., 2019) or multiple modes (Leddy et al., 2019) with another physical intervention such as stretching or walking, on persistent symptoms. All three studies were in a population aged 18-years or under, two began the intervention more than 10-days post-injury of mixed cause (Bailey et al., 2019; Kurowski et al., 2017) and one began the intervention within 10-days of a sport-related injury (Leddy et al., 2019). One study continued the intervention until symptom resolution and reported a significantly shorter time to symptom resolution for the aerobic exercise group (Leddy et al., 2019). Two studies conducted a 6-week intervention, with the aerobic exercise group in one study having a significantly greater improvement on the Post-Concussion Symptom Scale, however, only when data were adjusted for baseline levels of depression (Bailey et al., 2019). The other study reported significantly greater improvements in the aerobic exercise group for the Post-Concussion Symptom Inventory immediately post-intervention, however, data was only provided for a follow-up period by which the difference was no longer significant (Kurowski et al., 2017).
Vestibular exercise versus other physical intervention: Three studies assessed the effect of ves-tibular exercise interventions on persistent symptoms when compared to another physical intervention (Kleffelgaard et al., 2019; Reneker et al., 2017; Schneider et al., 2014), in a mixed age group who were more than 10-days post-injury. Two studies included only people recovering from a sport-related injury (Reneker et al., 2017; Schneider et al., 2014) and one study included people with mixed aetiologies (Kleffelgaard et al., 2019). One study reported a significant between-group difference in days to symptomatic recovery, as assessed by the Post-Concussion Symptom Scale after a 4-week program, favouring the vestibular intervention group compared to a subtherapeutic sham intervention group (median 13.5-days versus 17-days, HR = 1.99) (Reneker et al., 2017). Two studies incorporating an 8-week vestibular intervention did not report any significant differences between the vestibular exercise and comparison groups on either the Sports Concussion Assessment Tool (Schneider et al, 2014) or the Rivermead (Kleffelgaard et al., 2019).
Secondary study results: Other clinical measures
Included studies reported on a range of secondary measures, including physical and psychological performance, quality of life, medical clearance, and other secondary outcomes.
Physical performance
One study measured the effect of an 8-week group-based vestibular exercise program compared to usual care, and demonstrated a significant between-group difference in favour of the vestibular group on the High-Level Mobility Assessment Tool (mean difference: 3.7, 95% CI: 1.4 to 6.0, p = 0.002), however, did not find any significant between-group difference on the Balance Error Scoring System (Kleffelgaard et al., 2019).
Psychological performance
One study comparing the effects of a combined aerobic exercise, strength and psychoeducation intervention with usual care found a significant mean difference on the Major Depression Inventory at the 6-month follow-up period (p = 0.008, ES = 0.40) in favour of the intervention group (Rytter et al., 2019), whereas, another study comparing the effect of an aerobic exercise program with usual care did not find any between-group differences for psychological outcomes (Chan et al., 2018). Comparing a vestibular exercise program to usual care, one study (8-weeks/2x weekly), reported no between-group difference on the Hospital Anxiety Depression Scale at post-intervention and follow-up (Kleffelgaard et al., 2019).
Quality of life
One study compared a 22-week aerobic and muscle strength program to usual care and found significant improvement on domains of the Short Form Survey post-intervention and at the 6-month follow-up (p < 0.05) in favour of the aerobic exercise group (Rytter et al., 2019). Another study comparing a submaximal aerobic exercise to a usual care intervention over 6-weeks did not report any between-group differences on the Pediatric Quality of Life Multidimensional Fatigue Scale (Chan et al., 2018).
Medical clearance
One study comparing an aerobic exercise intervention to usual care reported no significant difference for Time to Medical Clearance for Return-to-Play (p = 0.87) (Micay et al., 2018). Two studies compared vestibular exercise interventions to another physical intervention (Reneker et al., 2017; Schneider et al., 2014), of which the first study reported time to medical clearance was 10.5 days sooner in the vestibular exercise group (median 15.5-days) compared to the sham intervention group (median 26-days, log-rank=0.18) (Reneker et al., 2017). The second study reported that the vestibular exercise group was 3.91 (95% CI: 1.34 to 11.34) times more likely to be medically cleared within 8-weeks compared to a stretching exercise group (Schneider et al., 2014).
Other secondary outcomes
An 8-week group-based vestibular exercise program found dizziness significantly improved on the Dizziness Handicap Inventory (mean difference: –8.7, 95% CI: –16 to –0.9, p = 0.03) but not on the Vertigo Symptom Scale, when compared to usual care (Kleffelgaard et al., 2019). A study comparing a 22-week aerobic and strength program to usual care reported significant improvements on some domains on the Multidimensional Fatigue Inventory and Headache Impact Test, post-intervention and at the 6-month follow-up period (p < 0.05) (Rytter et al., 2019). Lastly, a study comparing a vestibular exercise program (8-weeks/1x weekly) to a stretching intervention did not detail the between-group difference for outcomes of dizziness, vestibulo-ocular reflex, cervical proprioception, and cervical strength (Schneider et al., 2014).
Discussion
This study aimed to determine the effect of physical exercise on persistent symptoms in people with mTBI. Physical exercise interventions in the included studies were broadly considered as aerobic or vestibular. A meta-analysis of three studies demonstrated that aerobic exercise interventions significantly improved persistent symptoms in people with mTBI compared to usual care. A narrative analysis revealed limited evidence for the efficacy of vestibular interventions for improving persistent symptoms. Effects of aerobic and vestibular interventions on secondary clinical outcomes were unclear due to the heterogeneity of the outcome measures used.
Signs and symptoms following a mTBI may vary considerably between individuals due to biomechanical, pathophysiological and neurobehavioural factors (Kirkwood et al., 2006; McIntyre et al., 2020). However, symptom characteristics can be sub-typed into physiological, vestibulo-ocular and cervicogenic post-concussion disorder (Ellis et al., 2015; Ellis et al., 2016).
The proposed pathophysiology of physiological post-concussion disorder are the alterations in cerebral blood flow and metabolism (Ellis et al., 2016; Leddy et al., 2013), resulting in symptoms such as headache, dizziness, nausea, fatigue, light and sound sensitivity, irritability and symptoms exacerbated by physical or cognitive exertion (Ellis et al., 2015; Ellis et al., 2016). Aerobic exercise stimulates the autonomic nervous system through increased cardiac output, cerebral blood flow, cerebral metabolism and neuroplasticity, which improves symptoms and exercise tolerance (Leddy et al., 2013; Tan et al., 2014). Three studies in our review assessing the effects of aerobic exercise versus usual care were conducted in people aged 18-years or under (Chan et al., 2018; Dobney et al., 2020; Micay et al., 2018), two of which were in sporting related injuries (Chan et al., 2018; Micay et al., 2018) and two started the intervention at least 10-days post-injury (Chan et al., 2018; Dobney et al., 2020). None of the three studies demonstrated any beneficial effect of aerobic exercise on symptom recovery. Three studies comparing aerobic exercise to other physical interventions in people 18-years or younger all found that the aerobic intervention was statistically beneficial compared to light exercise involving mostly stretching (Bailey et al., 2019; Kurowski et al., 2017; Leddy et al., 2019) but these were not significant either in time to symptom resolution (Leddy et al., 2019), when adjusted for depression (Bailey et al., 2019) or did not maintain a significant effect as early as one week post-intervention (Kurowski et al., 2017). In our review, all aerobic exercise interventions used either subthreshold (exercising below symptom exacerbation) or submaximal (exercising to a percentage of the age-predicted maximum heart rate) intensity with treadmill running and stationary cycling being the most common modalities. Undertaking aerobic exercise at a subthreshold or submaximal intensity stresses physiological systems within the body’s autoregulatory capabilities to gradually restore autonomic control to normal so people with mTBI can experience the benefits of aerobic exercise without the exacerbation of symptoms (Ellis et al., 2016; Kleffelgaard et al., 2019). Aerobic exercise intervention programs of studies that reported improvement in persistent symptoms were generally of greater intensity (80% of subthreshold heart rate) and longer duration (≥6-weeks). This is supported by literature that reported improvements from aerobic exercise are seen 6 to 8-weeks after training (McArdle et al., 2014; McIntyre et al., 2020) and that too light of an aerobic intensity may lead to no improvements (Garber et al., 2011). This appears to be confirmed by the relative success of aerobic exercise when compared to light exercise interventions in the short-term from our results. High intensity may exacerbate symptoms especially within 3-days post-injury, however, the included studies that engaged in early exercise in our review did not demonstrate worsening symptoms, as no studies implemented a vigorous aerobic exercise intervention (Gurley et al., 2013; Lishchynsky et al., 2019; Majerske et al., 2008).
The proposed pathophysiology of vestibulo-ocular post-concussion disorder is dysfunction of the vestibulo-ocular system, and for cervicogenic post-concussion disorder, muscle trauma, inflammation, and dysfunction of the cervical spine proprioception, resulting in an array of vestibular and cervical symptoms that tend to overlap (Ellis et al., 2015; Ellis, 2016). Of the three studies applying a vestibular exercise intervention (Kleffelgaard et al., 2019; Reneker et al., 2017; Schneider et al., 2014), only one demonstrated a significant effect of the intervention after 4-weeks (Reneker et al., 2017) with the other two studies showing no difference between the intervention and control group after 8-weeks (Kleffelgaard et al., 2019; Schneider et al., 2014). All three vestibular interventions were initiated at least 10-days post-injury (Kleffelgaard et al., 2019; Reneker et al., 2017; Schneider et al., 2014). The vestibular interventions included a combination of canalith repositioning manoeuvres, habituation, gaze stabilisation, adaptation, substitution, balance and mobility exercises, which reintegrate and restore the somatosensory visual and vestibular systems (Ellis et al., 2016). The gold standard for vestibular rehabilitation is identifying functional limitations and subsequent prescription of an individualized program (Herdman et al., 2014) with the addition of manual therapy for the treatment of cervical pain and cervicogenic headaches being of additional benefit (Schneider et al., 2017), which was utilized in two of three studies that implemented a vestibular exercise intervention. Due to the small number of studies and variations in vestibular exercise intervention approaches, conclusions about the optimal intervention dosage and frequency could not be drawn.
In our review, time since injury ranged from less than a week to greater than 6-months. Only two studies (Leddy et al., 2019; Micay et al, 2018) started an intervention within 10-days post-injury, both were in participants aged 18-years and under with a sport-related injury and used an aerobic intervention with one reporting greater improvement than the control group (Leddy et al., 2019). Time since injury is an important factor to consider when prescribing exercise, as adults are expected to recover within 2-weeks and children within 4-weeks (McCrory et al., 2017). Additionally, individuals who do not receive intervention for persistent symptoms within the first 3-months are at risk of developing chronic symptoms, maladaptive coping strategies and mood disorders (Mayer et al., 2015; Rytter et al., 2019; Schneider et al, 2017), which may require additional interventions to address these comorbidities and secondary problems (Rabinowitz et al., 2014). Another factor that may influence exercise prescription is the cause of injury. Six studies in the review included sport injuries (Chan et al., 2018; Leddy et al., 2019; Maerlender et al., 2015; Micay et al., 2018; Reneker et al., 2017; Schneider et al., 2014), four using aerobic exercise (Chan et al.,, 2018; Leddy et al., 2019; Maerlender et al., 2015; Micay et al., 2018) and two utilizing vestibular exercise (Reneker et al., 2017; Schneider et al., 2014). Sport-related injuries typically exhibit less physical and psychological trauma compared to other causes of mTBI such as vehicular accidents, falls or assaults (Rabinowitz et al., 2014), and therefore are expected to recover faster.
The studies in the review were rated as medium to high, except for two studies, indicating the individual RCTs are of good quality. When the results were pooled together for a narrative GRADE assessment, there was moderate certainty of evidence for aerobic exercise compared to usual care for improving persistent symptoms.
The main strength of this systematic review is the systematic and transparent method used for the identification of eligible research studies, and appraisal of study quality and reporting, as well as evidence certainty rating. Another strength of this review is the fact that it included RCTs only and did not limit by demographic characteristics. Since the initiation of this review, four other reviews were published (Baker et al., 2021; Langevin et al., 2020; Powell et al., 2020; Shen et al., 2021). Whilst these reviews agreed with our findings that aerobic exercise can improve persistent symptoms (Baker et al., 2021; Langevin et al., 2020; Powell et al., 2020; Shen et al., 2021), all reviews included sport-related concussions and aerobic exercise (Baker et al., 2021; Langevin et al., 2020; Powell et al., 2020; Shen et al., 2021) and one included all study designs (Baker et al., 2021).
Some limitations should be considered too. Firstly, due to the lack of a widely accepted definition of mTBI, study populations were defined differently in all studies, which may have confounded the results. MTBI presents with a wide variation of symptoms and treatments should be targeted specifically to the individual symptoms. Secondly, studies generally had small sample sizes and effect sizes, however, this issue was partially addressed by the conduct of a meta-analysis for the effect of aerobic exercise on persistent symptoms. Thirdly, the heterogeneity of the outcome measures used hindered the completion of a meta-analysis for vestibular exercise on persistent symptoms. Lastly, intervention characteristics varied across studies making it difficult to draw conclusions with regards to optimal exercise prescription.
Conclusion
The results of the meta-analysis are in favour of the aerobic exercise intervention compared to usual care, yet there is limited evidence for the use of vestibular exercise for improving persistent symptoms in people with mTBI. Future studies should target the intervention to be specific to the characteristics of the mTBI such as the type of disorder, cause of injury and age of the individual. Lastly, more robust study methodologies and the establishment of a consistent outcome measure for reporting persistent symptoms are needed to reduce risk of bias.
Conflict of interest
None to report.
Funding
This study has received no external funding.