
Abstract
BACKGROUND:
A variety of acupuncture therapies have shown efficacy in Parkinson’s disease (PD).
OBJECTIVE:
To evaluate scalp acupuncture (SA) effects on motor and cerebral activity by using gait equipment and resting-state functional magnetic resonance imaging (rs-fMRI).
METHODS:
Twelve patients with PD received SA. They underwent the first functional-imaging scan after tactile stimulation and the second scan following needle removal. Gait test and local sensation assessment were performed immediately after each functional scan. Gait parameter differences between pre- and post-SA were analyzed using a paired t-test and altered brain areas in degree centrality (DC) and fractional amplitude of low-frequency fluctuation (fALFF) were identified between the two scans.
RESULTS:
Eight patients completed the experiment. Stride length, maximum ankle height, maximum ankle horizontal displacement, gait speed, and range of shank motion significantly increased post-treatment (P < 0.05). fALFF in left middle frontal gyrus and DC in left cerebellum (corrected) increased, while fALFF in left inferior parietal lobule (corrected) during SA decreased, compared with those in tactile stimulation. A positive correlation was observed between right limb swings and both fALFF areas.
CONCLUSIONS:
Differences in gait and brain analyses presented modulation to motor and brain activity in PD, thus, providing preliminary evidence for SA efficacy.
Keywords
Introduction
Gait dysfunction is a manifestation of movement disorders (Mirelman et al., 2019) and is a core feature of Parkinson’s disease (PD). Patients with PD exhibit decreased balance and flexibility in motor actions, which can lead to further deterioration in postural stability and falls (Hong et al., 2009; Lieberman et al., 2012). Dopaminergic drugs remain the mainstay of treatment for motor disturbances (Giugni & Okun, 2014). However, disease progression, drug side effects, and the development of poor response to medication underscore the need for alternative and complementary strategies for motor symptom management (Jankovic, 2005; Tran et al., 2018). Acupuncture is a promising therapeutic intervention that has proven to be effective for the treatment of neurological disorders (Jiang et al., 2018; Kluger et al., 2016; Lee et al., 2014; Schuler et al., 2005; Wong et al., 2003), including PD, due to its wide adaptability and lack of side effects. However, due to methodological pitfalls and lack of objective measurements, the efficacy of acupuncture and its neural mechanism remain unclear.
The Unified Parkinson’s Disease Rating Scale (UPDRS) III is commonly used to measure motor function in studies of PD, though it only provides subjective and approximate evaluations (Bloem et al., 2016). Since the development of wearable inertial measurement unit (IMU) devices, equipment-based gait analysis has gradually addressed this flaw, enabling consistent and repeatable measurements (Horak & Mancini, 2013) of gait parameters in digital form to characterize the actual gait (Schlachetzki et al., 2017), which can serve as an outcome index of the clinical efficacy of new therapies.
Regarding mechanism research, resting-state functional magnetic resonance imaging (rs-fMRI), a non-invasive tool, is used to investigate the neural activity of the brain and physiological mechanisms underlying acupuncture (Fox & Raichle, 2007; Li et al., 2018; Nierhaus et al., 2019; Park et al., 2009). It is considered to reflect local or global functional alterations in blood oxygen level-dependent (BOLD) responses, and the changes in BOLD signals are associated with spontaneous neuronal activity (Zuo et al., 2010). Several studies have demonstrated that PD presents with disrupted functional features at different levels, including regional homogeneity (Nguyen et al., 2021), fractional amplitude of low-frequency fluctuations (fALFF) (Lv et al., 2021), and degree centrality (DC) (Li et al., 2019). To date, several studies on cerebral imaging have contributed toward the knowledge of neural activity related to acupuncture stimulation. Yeo et al. (2014), using regions of interest analysis, reported that precentral gyrus and prefrontal cortex are activated by acupuncture and that motor symptoms improved in patients with PD. This improvement may be related to increased neural responses after acupuncture stimulation (Yeo et al., 2012). Li et al. (2018) also showed, using multiple MRI analyses of cerebral activities, that acupuncture could modulate the cerebello-thalamo-cortical circuit and alleviate PD tremors. These advances indeed illustrate that acupuncture can modulate brain activity as shown in functional imaging.
Generally, acupuncture needles are manually inserted into target points and elicit a type of physical response or sensation called deqi, which is characterized by soreness, numbness, heaviness, and fullness. Notably, deqi is a shapeless but strong stimulus that can arouse widespread cerebral activity. Therefore, it is difficult to distinguish between changes caused by acupuncture stimulation or the result of the acupuncture therapeutic effect. In fact, the differences between post-acupuncture cerebral networks are correlated with the intensity and duration of stimulation (Bai et al., 2010; Shukla et al., 2011). Tactile control, as part of acupuncture stimulation processing, can arouse a neural response in the brain network that is similar to acupuncture. In addition, wide response caused by needle insertion as a cofounding factor for regional functional evaluation of acupuncture effectiveness cannot be ignored (Chae et al., 2013).
Scalp acupuncture (SA), a type of modern acupuncture based on brain anatomy (Jiao, 1993), is a painless and mild stimulation technique using shallow needle insertion into the scalp without specific needle sensation. The therapeutic effects of SA have been shown to be significant (Hao & Hao, 2012) and SA has been used in the treatment of many movement disorders. To the best of our knowledge, only a few previous studies have adopted SA as an intervention for PD treatment. Most of these studies were of low quality, without appropriate controls and valid/powerful evaluating tools. None of the previous studies has combined a neuroimaging investigation with other clinical objective evaluation systems to assess the effectiveness of SA in improving the motor symptoms of PD.
This study aimed to assess the feasibility and efficacy of SA on improving the motor function of patients with PD. For this pilot study, a wearable IMU device was used to evaluate the effect of SA on gait in patients with PD. Then, we explored the cerebral functional changes in a resting state using fALFF to indicate regional spontaneous neural activity and using DC to identify regions that correlated to stimulation. Finally, we determined the correlation between functional brain activity and gait performances. Taken together, these measurements resolved the shortcomings of the methodology and outcome measures used by previous studies.
Materials and methods
Participants
Sample size was calculated (Python V3.8.7 software) and a convenience sample of 12 patients with PD was recruited for this pilot study. The study protocol followed the principles of the Declaration of Helsinki and was approved by the ethical committee of Zhejiang Hospital (2019 Clinical Review No. 5 K & 2021 Clinical Review No. 72 K).
The inclusion criteria were: (1) right-handed patients with mild-to-moderate (Hoehn and Yahr [H&Y] stage < 4) idiopathic PD diagnosed by a neurologist prior to study entry; (2) 40–85 years of age; (3) no cognitive impairment (tested by Mini-Mental State Examination (MMSE) > 10); (4) willing to complete motor evaluation (UPDRS III), gait testing, and fMRI scanning; (5) able to walk independently, on stable dopaminergic medication, and in a stable condition to volunteer for this treatment protocol; and (6) provided written informed consent.
The exclusion criteria were: (1) secondary or atypical Parkinsonism; (2) cognitive impairment (MMSE score < 10); (3) prior history of stroke, head trauma, or other neurological disorders; (4) history of heart disease, pacemaker, or implanted defibrillator; (5) any contraindications for fMRI; and (6) head motion rotating over 2° or translation over 2 mm in scanning or different degree of regional sensations between two interventions.
Experimental paradigm
This was a single-blinded and tactile-controlled study (Fig. 1A). Tactile stimulation was designed to control the effect of instantaneous sensation, a potential confounding factor, during needle insertion in acupuncture. Similar acupuncture processes were observed in previous investigations (Hui et al., 2005; Jung et al., 2015; Li et al., 2006). We intended to observe regional activity and global functional connectivity of brain by BOLD signals; thus, two fMRI scans were completed, rest1 (after tactile stimulation) and rest2 (after scalp acupuncture). Each patient underwent gait testing after two fMRI scans, gait1 and gait2. The participants were also asked to walk for 20 minutes before the needles were removed.
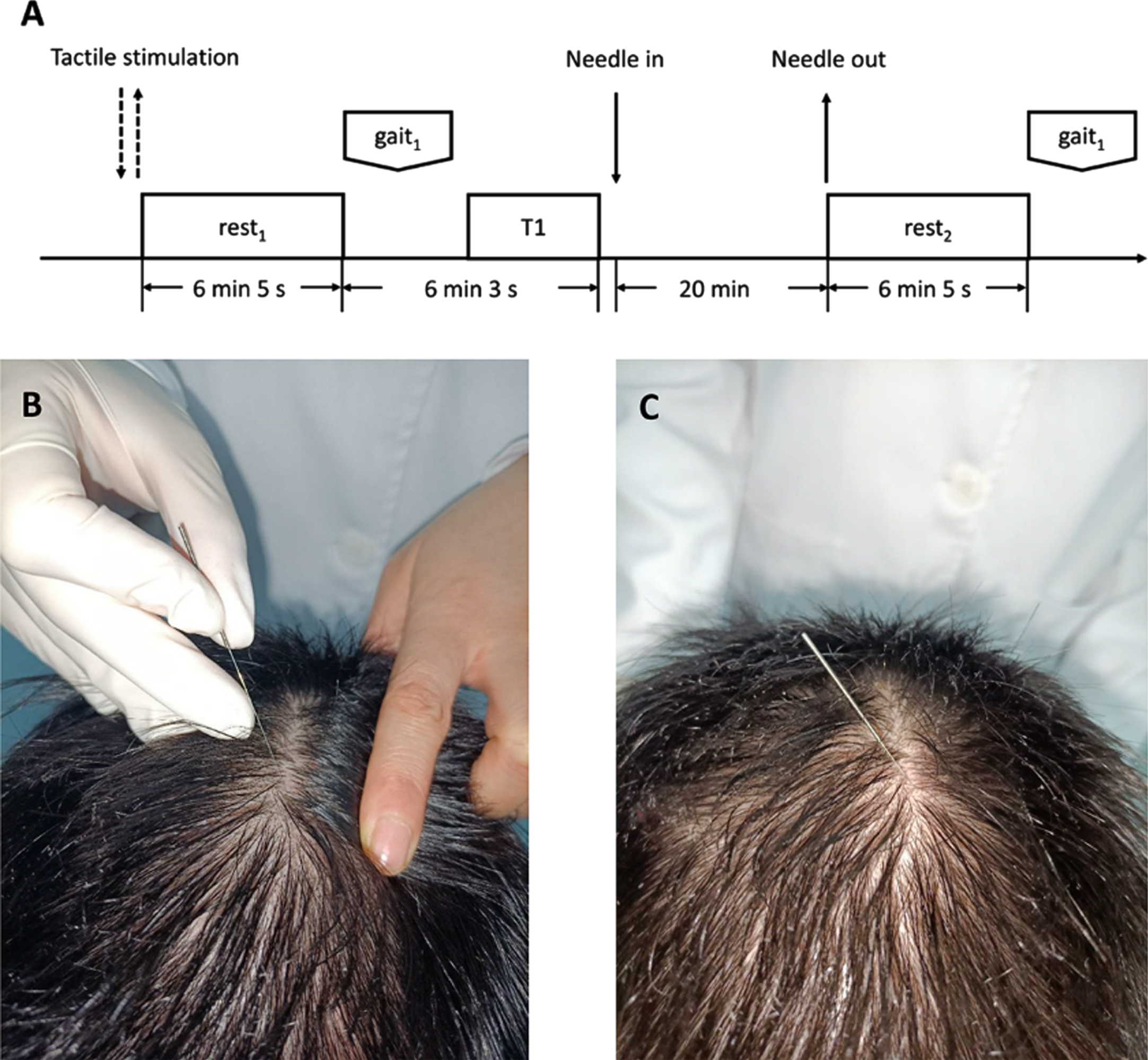
Study design. (A) Intervention paradigm (tactile stimulation and scalp acupuncture), functional-image scan (rest1 and rest2), structural-image scan (T1), gait testing (gait1 and gait2) and walk for 20 min; (B) Tactile stimulation time point; (C) Needle retaining of scalp acupuncture.
All the individuals accepted tactile stimulation before needle insertion (SA stimulation). The tactile sensation was relieved for approximately 3 seconds, at needle-inserting point, by consistent pricking without penetrating the skin (Fig. 1B). The needle and its angle to the scalp were the same as the following description.
Scalp acupuncture
SA was performed by an experienced acupuncturist. In the protocol, stainless steel needles were manually inserted into the upper one-fifth of the motor area, chorea-tremor controlled area, and balance area to a depth of 2.0–3.0 cm to alleviate motor symptoms according to traditional Chinese medicine documents. The locations of the primary acupoints are shown in Fig. 2.

(A) Motor area; (B) Chorea-tremor controlled area; (C) Balance area.
We selected single-use metallic acupuncture needles (0.25 mm×40 mm; Huanqiu brand, Suzhou, Jiangsu Province, China) made of stainless steel. The acupuncturist disinfected the skin of the selected upper point of the acupoint area, and swiftly inserted needles into the subcutis at a 15° angle. Next, the needle was pushed down into the scalp toward the direction of lower point until half of the needle was covered under the subcutis (Fig. 1 C). SA stimulation was bilateral and equivalent for each person, and no pain was induced if the needles were successfully inserted. In addition, as a part of treatment, patients were instructed to walk for approximately 20 min at normal speed on a set flat area.
Apart from experiencing sensations during each scan, all individuals were asked to report regional needle sensations that came from tactile and SA by using the numerical rate scale: 0 = no; 1 = mild; 2 = moderate; 3 = strong sensation. To ensure the validity of SA and tactile controls, participants were excluded if they reported experiencing different levels of sensations between the two stimulations or if they experienced any regional sensations during the two functional imaging scans.
Gait evaluation
A wearable IMU device, designed and made by the School of Mechanical Engineering, Zhejiang University (Wang et al., 2019), was used for testing gait changes in patients with PD before and after acupuncture treatment (denoted as gait1 and gait2, respectively). The features of the gait system and related operational process have been reported previously (Wang et al., 2019). During the trial, two IMUs were worn on the ankle on the lateral side of each shank, and patients were then instructed to walk 20−40 m on the designated path (Fig. 3). The IMU obtained samples at a frequency of 100 Hz, and the collected data were saved on an SD card. A database algorithm system based on MATLAB (version R2014a, MathWorks, Portola Valley, CA, USA) was used to determine the gait parameters from the collected data. Given the influence of IMU position differences among participants and dependence on biomechanical parameters, we removed the height factor and normalized several gait parameters, as follows: (1) stride length (SL) was defined as the linear shift between two foot landing spots of a single foot divided by the height; (2) gait cycle duration (GD) was defined as the temporal continuance between two heel-strikes of a single foot; (3) gait speed (GS) was defined as SL divided by GD and divided by height; (4) swing phase (SP) was defined as the temporal continuance between heel-strike and toe-off of a single foot divided by GD; (5) maximum ankle height (MH) was defined as the maximum vertical displacement of the ankle divided by height in the GD period; (6) maximum ankle horizontal displacement (MHD) was defined as the maximum horizontal displacement of the ankle at maximum ankle height divided by height; (7) range of shank motion (RS) was defined as ambit integration of the angular velocity of the shank z-axis in the swing phase; (8) maximum ankle abduction (MAB) was defined as the maximum outward shift of the ankle vertical to the direction of SL divided by height during GD; and (9) maximum ankle adduction (MAD) was defined as the maximum inward shift of the ankle vertical to the direction of SL divided by height during GD. The tests were conducted immediately following rest1 and rest2.
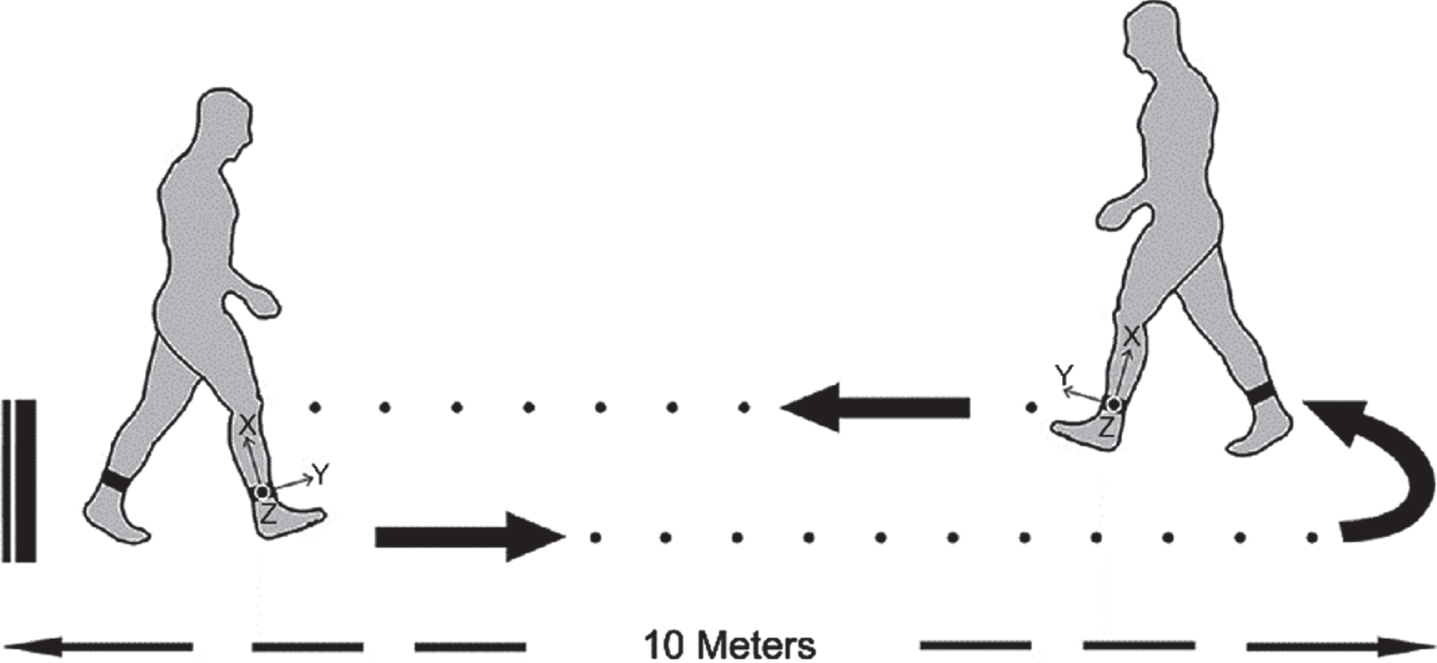
Inertial measurement unit device and walking path.
MR images were acquired with a Siemens MAGNETOM Skyra 3.0 T (Siemens Healthcare, Erlangen, Germany) scanner at Zhejiang hospital, before, and after SA treatment. Both scans were scheduled within 5 min after the gait test. During data acquisition, all patients were fitted with foam pads to minimize head motion. Patients were instructed to close their eyes without thinking of anything but to avoid falling asleep. Earphones were used to reduce scanning noise. The scanning included two functional images (rest1 and rest2) and 3D T1 structural images. fMRI parameters were as follows: 32 axial slices, repetition time (TR) = 2,000 ms, echo time (TE) = 30 ms, slice thickness = 3.5 mm, flip angle (FA) = 90°, matrix = 64×64, field of view (FOV) = 224×224 mm2, and scan time of 6 min 5 s. The T1 structural image scanning parameters were as follows: 256 slices, TR = 2,530 ms, TE = 2.98 ms, slice thickness = 1.0 mm, FA = 7°, matrix = 256×256, FOV = 256×256 mm2, and scan time of 6 min 3 s.
MRI data preprocessing
The rs-fMRI data analysis toolkit (Jia et al., 2019) (RESTplus V1.21, http://www.restfmri.net/forum/RESTplusV1.2) and statistical parametric mapping (SPM12, https://www.fil.ion.ucl.ac.uk/spm) based on MATLAB (2014a) were used to analyze the collected data. Data preprocessing was performed as follows: (1) removal of 10 time points at the beginning of scanning to ensure the stability of the condition and adaptation of the patient; (2) slice-timing correction of different slices in the image (Poldrack et al., 2011); (3) realignment of scans across time to correct head movements; (4) spatial normalization to Montreal Neurological Institute (MNI) space and resampling to a voxel size of 3×3×3 mm3; (5) spatial smoothing to reduce the mismatch between individuals using a 6-mm full-width half-maximum Gaussian kernel (Mikl et al., 2008); (6) linear trend removal; (7) inclusion of Friston-24 head motion parameters (Friston et al., 1996), white matter signals, and cerebrospinal fluid signals in nuisance covariates regression; and (8) low-pass filtering in the range of 0.01−0.08 Hz (Friston et al., 2000).
fALFF computing
During data post-processing, at each voxel level, time courses were converted to frequency domains using the built-in fast Fourier transform function and obtained the power spectrum. The square-root was determined for each frequency. Subsequently, the mean square root value across a range from 0.01−0.08 Hz at single voxels was divided by the mean square root value across an entire frequency band from 0−0.25 Hz. The obtained ratio of the power spectrum was defined as fALFF (Zou et al., 2008).
DC computing
DC values were obtained by extracting the time series of each voxel using the RESTplus program. Pearson’s correlation coefficients (r) from one voxel to another time series in the brain mask were automatically calculated during the post-processing step, and the voxels were considered relative if r> 0.2. Thus, a whole-brain functional connectivity map was obtained for each participant. For normalization, Fisher’s r-to-z transformation was used to transform the voxel correlation centrality diagrams into a z-score diagram. To characterize the regional central roles (Zuo et al., 2012), the weighted DC of a single voxel was computed as the sum of its weighted connections with all other voxels.
Statistical analyses
Sample size calculation was done via power analysis using the Python V3.8.7 software (effect size 0.9, significant level 0.05, and statistical power 0.8). A sample size of 12 was deemed necessary for adequate power.
Patient demographics (such as sex, age, and PD duration) and clinical characteristics (MMSE, H&Y, and UPDRS III score) were compared pre- and post-treatment. Data are presented as means±standard deviations.
Gait analysis
Statistical Package for Social Sciences (SPSS) V23.0 (IBM Corp., Armonk, NY, USA) was used to analyze the sampled left- or right-side IMU-based gait parameters before and after SA, with a paired t-test or nonparametric t-test if the data were non-normally distributed. The significance level was set at P < 0.05.
fALFF and DC analysis
Statistical analysis of fALFF and DC was performed using RESTplus V1.21. We compared MRI data (rest1 and rest2) obtained pre- and post-SA for a given area using a paired t-test. Multiple comparison correction was executed based on the resultant T-maps with a minimal threshold cluster size of 10, connecting criteria (rmm) = 5 (with connected edges), and Gaussian random field theory (GRF) (voxel-wise P < 0.01, cluster-wise P < 0.05; two-tailed test).
Correlation analysis
We extracted the fALFF signals and DC maps within statistically significant clusters during pre-preparation. To investigate the relationship between the instant effects of SA and alterations in brain function, Pearson correlation analysis was performed to analyze the correlation between cerebral functional changes (according to mean signal values of fALFF and DC) in characterized regions and gait parameters. We also examined the possible connections between motor function and local metrics by calculating the Pearson correlation coefficients between the signal values of the characterized regions and UPDRS III scores.
Results
Patient demographics
Twelve right-handed patients with PD were included in the study. Four patients were excluded in subsequent analysis (two patients experienced different levels of sensations between the two interventions and two patient had head motion > 2°/2 mm). A total of eight participants (six men, two women) were included in the statistical analysis. The mean age of the patients was 71.50±7.65 years, mean body height 164.75±7.32 cm, mean body weight 61.70±7.28 kg, and mean PD duration was 10.50±8.14 years. Mean cognitive function score as assessed using the MMSE was 26.25±2.18. The mean score for the motor section of the UPDRS III was 57.62±7.78, and the mean H&Y staging was 2.87±0.23.
Gait results
The analysis indicated that stride length, maximum ankle height, maximum ankle horizontal displacement, gait speed, and range of shank motion significantly increased (P < 0.05) after the 20-min SA relative to values before the acupuncture intervention. These changes exhibited the same trends on both sides (Table 1).
Gait changes pre- and post-intervention
Gait changes pre- and post-intervention
Data are presented as means±standard deviations. *P < 0.05. SL, stride length; GD, gait cycle duration; SP, swing phase; GS, gait speed; MH, maximum ankle height; MHD, maximum ankle horizontal displacement; RS, range of shank motion; MAB, maximum ankle abduction; MAD, maximum ankle adduction.
Compared with pre-treatment (rest1), two clusters of fALFF values were substantially altered after SA treatment (rest2). We observed an increase in fALFF in the left middle frontal gyrus (T-value = 6.395) and a decrease in fALFF in the left inferior parietal lobule (T-value = –10.082). Details of the peak coordinates and cluster sizes are presented in Table 2 and Fig. 4.
Regions that exhibited increased and decreased fALFF and DC in patients after scalp acupuncture
Regions that exhibited increased and decreased fALFF and DC in patients after scalp acupuncture
fALFF, fractional amplitude of low-frequency fluctuation; DC, degree centrality; MNI, Montreal Neurological Institute.

Map of cerebral functional response to SA. Red and yellow: increased; blue: decreased fALFF activation after SA (rest2) compared with values before SA (rest1), with GRF threshold (voxel-wise P < 0.01, cluster-wise P < 0.05, and two-tailed testing). SA, scalp acupuncture; fALFF, fractional amplitude of low-frequency fluctuation; GRF, Gaussian random field.
Compared with pre-treatment values (rest1), DC values significantly increased in the left cerebellum (T-value = 10.438) of patients after SA treatment (rest2). The details of the peak coordinates and cluster sizes are presented in Table 2 and Fig. 5, respectively.

Map of cerebral functional response to SA. Red and yellow: increased; blue: decreased DC activation after SA (rest2) compared with values before SA (rest1), with GRF threshold (voxel-wise P < 0.01, cluster-wise P < 0.05, and two-tailed testing). SA, scalp acupuncture; DC, degree centrality; GRF, Gaussian random field.
The fALFF1 values (spherical area, MNI central coordinates: –27, 21, 51; radius, 6 mm) of rest1 and rest2 were positively correlated with Gait1 (r= 0.789, P = 0.019) and Gait2 (r= 0.751, P = 0.031), whereas fALFF2 values (spherical area, MNI central coordinates: –39, –39, 51; radius, 6 mm) at rest1 and rest2 were negatively correlated with Gait1 (r = –0.799, P = 0.017) and Gait2 (r = –0.854, P = 0.007). The data are presented in Fig. 6 and Table 3. No significant correlations were observed between other regions, gait, or clinical characteristics of patients with PD (P > 0.05).

Scatter plots of fALFF and right shank gait parameters. (A) A significant correlation is observed between swing phase and fALFF in the left middle frontal gyrus (Pearson correlation, P = 0.019 for rest1, P = 0.031 for rest2). (B) A significant correlation is observed between swing phase and fALFF in the left inferior parietal lobule (Pearson correlation, P = 0.017 for rest1, P = 0.007 for rest2). fALFF, fractional amplitude of low-frequency fluctuation; fALFF1, fALFF in the left middle frontal gyrus; fALFF2, fALFF in the left inferior parietal lobule; Gait1, swing phase of the right shank before treatment; Gait2, swing phase of the right shank after treatment.
Correlations between local metrics and gait/clinical characteristics
*P < 0.05; fALFF, fractional amplitude of low-frequency fluctuation; fALFF1, fALFF in the left middle frontal gyrus; fALFF2, fALFF in the left inferior parietal lobules; DC, degree centrality; UPDRS III, Motor section of Unified Parkinson’s Disease Rating Scale.
In this study, we investigated the immediate effects of SA in patients with PD using a wearable IMU device and functional MRI. We observed that acute SA significantly improved partial gait parameters of both limbs in patients with PD. In addition, compared to tactile stimulation, SA revealed increased low-frequency oscillation responses (fALFF) in the left middle frontal gyrus and connectivity (DC) in the left cerebellum and a decreased fALFF in the left inferior parietal lobule during needle retention. Furthermore, gait parameters of the swing phase in the right limb were positively correlated with fALFF signals in the left middle frontal gyrus and left inferior parietal lobule. Collectively, since there was no difference in local feeling caused by tactile stimulation and needle stimulation, our findings indicate that SA improved motor symptoms of patients with PD and provided mechanistic evidence for the relationship between brain activity and the instant effects of acupuncture.
Motor dysfunction is the most evident characteristic of PD and is a prerequisite for diagnosis (Hallett, 2011; Hughes et al., 1992). Gait disturbances, one of the most visible and severe motor symptoms characterized by decreased stride and speed, can lead to a decline in mobility (Mak, 2013). Moreover, a deficit in balance control is the main risk factor for falls (Dibble et al., 2009; Muslimovic et al., 2008). Given the side effects of conventional drug treatments, acupuncture has emerged as a popular alternative therapy (Jiao, 1993). SA, a combination of traditional Chinese acupuncture and western medicine, has been applied to the cerebral cortex and is known to affect the central nervous system. Scalp needling may be valuable for the treatment of motor dysfunction caused by nervous system diseases, such as stroke (Wang et al., 2017).
The efficacy of traditional acupuncture for the treatment of PD varies, predominantly due to the use of subjective evaluations. To ensure more objective assessments, IMU devices are increasingly being used for gait measurements (Rodriguez-Molinero et al., 2015). In this study (Wang et al., 2019), each patient was instructed to perform a walking trial after tactile stimulation and SA and the data acquired by IMU were divided into 10 motor parameters, which reflected gait characteristics. Our results suggested that bilateral stride, gait speed, ankle height, ankle horizontal displacement, and range of shank motion improved after SA, which reflected improvements in lower limb stepping and flexibility. These data suggest positive effects of SA that enable patients with PD to walk more normally.
To elucidate the possible mechanisms of SA, we analyzed the resting-state function of the brain using different methods (Fox & Raichle, 2007). The fALFF, an improved analysis method, reflects the degree of spontaneous brain activity. The peak point in the left middle frontal gyrus exhibited an increase in the fALFF, while the frontal lobe, dorsolateral prefrontal cortex, superior frontal gyrus, and Brodmann area (BA) 8, 9, and 10 were also involved in signal enhancement. The peak point in the left inferior parietal lobule region exhibited decreased fALFF in addition to related areas, such as the precentral gyrus, postcentral gyrus, frontal lobe, parietal lobe, and BA 1, 2, 3, 4, and 6 of the left cerebrum. These findings indicated that fALFF signal changes encompassed almost the entire left frontal lobe (Maidan et al., 2016), which is strongly involved in the control of walking (Catani, 2019). The motor area of the cerebral cortex, located in the frontal lobe, cross-regulates physical activity, and is associated with the precentral gyrus, which coordinates muscle activity (Catani, 2019; Chouinard & Paus, 2006). The premotor cortex serves as the cortical center of the extrapyramidal system and is associated with coupled motion and abnormal postural regulation. In contrast to symptoms of general cerebellar lesions, the gait of patients with PD is classified as frontal ataxia, underscored by short steps, clumsiness, and a tendency to fall backwards (Thompson, 2012).
Locomotion in humans is associated with visual function (Davidsdottir et al., 2005). Initially, the relevant environment is visually sensed, and the information is transmitted to the cerebral cortex to generate motion perception and, ultimately, motor behavior (Pakan et al., 2018). Although there was no obvious activation of the visual center in the current study, alterations in the cortical lateral visual center of the middle frontal gyrus or frontal lobe may be considered useful for gazing and motor commands, which is consistent with previous research (Caminiti et al., 1996).
DC reflects the quantifiable centrality measure between a voxel-based region and the global brain network. In our analysis, the cerebellar region exhibited increased DC after SA (Caligiore et al., 2017). The cerebellum and basal ganglia are key structures that modulate human movement, cognition, and behavior, and are densely interconnected. The main factor in PD is pathological changes in neurons projecting from the substantia nigra to the striatum (Wu & Hallett, 2013). Recent studies have demonstrated that the cerebellum and basal ganglia have reciprocal anatomical connections (Wu & Hallett, 2013). The cerebellum has di-synaptic projections to the striatum via the thalamus and may influence information integration in the basal ganglia, thus, impacting movement (Lee et al., 2000; Simioni et al., 2016; Yu et al., 2007). It has been suggested that the cerebellum plays a compensatory role for basal ganglia dysfunction in PD, which alters motor function in patients.
In this study, we excluded a confounding factor by setting tactile control to maximize brain activity from acupuncture efficacy. The selected acupuncture sites targeted the projection of the precentral gyrus and cerebellum on the scalp (Hao & Hao, 2012). Notably, corresponding cortical function was activated after treatment. This suggests that even if the intervention does not reach brain tissue, it may still exert therapeutic effects similar to those induced by targeting the cortex. We also observed a positive correlation between the right swing phase and fALFF changes in the middle frontal gyrus and left inferior parietal lobule. These two activated functional areas share the common feature of being visually related, and visual perception is associated with motor balance (Bronstein et al., 1990). The frontal lobe, parietal lobe motor area, and visual coordination area of the cerebellum may exert feedback effects on motion (Bronstein et al., 1990; Caminiti et al., 1996), indicating that appropriate visual perception may improve spatial positioning disorders (Song et al., 2015). Indeed, direct visual stimulation enhances motor and balance functions in patients with PD. The swing phase provides an objective measure of gait stability, whereby an increased swing phase indicates increased trunk coordination (Bruijn & van Dieen, 2018), which has significant implications for gait. This study reports that SA activated the frontal and parietal lobes, and this activation also promoted motor function, especially balance, in the patients. However, we did not observe a significant correlation between any gait parameter in the left limb and activated brain regions. The inconsistent effects between the left and right sides may be attributed to two reasons: the patients were right-handed, and most had severe motor symptoms on the right side. Nevertheless, we were unable to elucidate the mechanisms underlying this phenomenon in this study.
This preliminary study has several limitations. First, due to the small sample size and large data dispersion, we could not identify false positives in the results. Second, to determine whether the one-sided correlation was caused by physiological right-handedness or acupuncture stimulation, an appropriate control group would be required. Thus, in the future, it is necessary to conduct a study with a larger sample size and to include a control (sham-acupuncture or no-treatment) group to clarify the effectiveness of SA.
Conclusion
This study demonstrated that SA had immediate positive effects on movement disorders, especially gait dysfunction, in patients with PD. The potential mechanism may involve activation of the frontal lobe, parietal lobe, and cerebellum after SA, and modulation of these regions may contribute to enhancement of motor ability in patients with PD.
Footnotes
Acknowledgments
The authors thank all the participants for joining this study.
Conflict of interest
None to report.
Funding
This research was supported by the Key Research Project of Traditional Chinese Medicine in Zhejiang Province (No. 2020ZZ001) and the Construction Plan for the Inheritance Studio of Xiaoqing Jin Famous Chinese Medicine Experts in Zhejiang Province (No. GZS2021011).
Author Contributions
Yingying Sun: Investigation, Writing-review, editing. Lihong Li: Data curation, Writing- Original draft. Yao Chen: Software, Validation. Lei Wang: Software, Validation. Lihao Zhai: Visualization, Investigation. Jili Sheng: Data curation. Tao Liu: Supervision. Xiaoqing Jin: Conceptualization, Methodology, Project administration, and Funding acquisition.