
Abstract
BACKGROUND:
Acupuncture has been used to treat patients with post-stroke neurological dysfunction.
OBJECTIVE:
The purpose of our observational study was to observe the long-term efficacy of acupuncture and investigate whether the acupuncture treatment could short the recovery time of patients with post-stroke dysphagia.
METHODS:
Medical records were reviewed to select patients who met the inclusion criteria for post-stroke dysphagia. Exposure factor was defined as received acupuncture during inpatient. Clinical data were obtained at the 6-month follow-up. The primary outcome was the time to improve the score of Food Intake Level Scale (FILS, 0–10) by 3 grades. Cox regression models were used to assess the relationship between acupuncture and recovery of dysphagia.
RESULTS:
In acupuncture group, the median time to achieve clinical improvement of dysphagia was 97 days (95% CI, 93–124) compared with 119 days (95% CI, 108–145) in control group, with a statistically significant difference between the two groups (HR = 1.48; 95% CI 1.14–1.92; P = 0.003). At 6 months, 78 patients (60.5%) in acupuncture group reached excellent function and 61 patients (47.3%) in control group (RR = 1.28; 95% CI, 1.02–1.62; P = 0.045). 106 patients (82.2%) in acupuncture group achieved favorable function and 91 patients (70.5%) in control group (RR = 1.17; 95% CI, 1.02–1.35; P = 0.039). The outcome of adjusted multivariable Cox regression models showed that there was a difference in the recovery time of dysphagia between groups, HR = 1.79, 95% CI 1.34–2.39. The rates of adverse events were similar in both groups.
CONCLUSIONS:
Acupuncture can promote the recovery of post-stroke dysphagia, and has a better long-term efficacy. Besides, it can reduce the degree of disability and improve the quality of life.
Introduction
Dysphagia is a common complication after stroke, with an incidence rate of 37–78% (Martino et al., 2005). It may cause adverse consequences such as pneumonia, asphyxia, dehydration and malnutrition, which seriously affect the life quality of patients and even can be life-threatening (Arnold et al., 2016). The treatment of post-stroke dysphagia includes swallowing training, biofeedback, breathing training, repetitive transcranial magnetic stimulation, neuromuscular electrical stimulation, or surgery (Winstein et al., 2016), but the long-term effect is limited.
In China, acupuncture has been practiced to treat patients with post-stroke neurological dysfunction. “Hand and foot acupuncture with twelve needles” includes the acupoints Hegu, Quchi, Neiguan, Yanglingquan, Zusanli and Sanyinjiao; according to Traditional Chinese Medicine theory, acupuncture at these points can pass through the meridians, regulating qi and blood. It can effectively reduce the lesion excitability of the contralateral primary motor cortex and improve the excitability imbalance in the bilateral cortex in patients with ischemic stroke (Fang et al., 2021).
Many studies have shown that acupuncture could facilitate functional recovery in patients with post-stroke dysphagia and improve their life quality (Zhang et al., 2014). The meta-analysis included 39 studies (Lu et al., 2021) showed the effective rate was significantly higher in the acupuncture group than in the control group (RR = 1.23; 95% CI:1.19–1.27; P < 0.001), indicating that acupuncture can treat dysphagia. However, there was opposite conclusions (Hopwood et al., 2008), acupuncture group and sham needling group showed no statistical difference in the improvement of neurologic outcome. The above contradictory evidence may be related to the small sample size of related studies. Additionally, most studies focus on the assessment of short-term efficacy of acupuncture. The mechanisms of acupuncture were commonly thought to be related with the neuromodulation, which usually needed a relative long time to produce effects. Besides, instant evaluation could barely provide convincing evidence to support the acupuncture could make a sustained efficacy to influence the long-term prognosis of patients.
Liu et al. (2020) found that the cortex thickness increased in the early phase of stroke, which could even continue to increase until the first 6 months. Wu & Liu (2009) proposed that post stroke 5-6 months, when the recovery enters a plateau period, is an appropriate time point to evaluate the results of neurological function. Based on above evidences, the primary aim of our observational study was to evaluate whether the acupuncture treatment could short the recovery time of patients with post-stroke dysphagia.
Methods
Study design
The purpose of our observational study was to investigate whether the acupuncture treatment could short the recovery time of patients with post-stroke dysphagia by extending the follow-up period to 6 months. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline served as the framework for the study design and methodology (Elm et al., 2008) (Supplementary Table 1).
Study populations
In this observational study, we retrospectively reviewed the medical records of Xuanwu Hospital Capital Medical University and Beijing Hospital of Traditional Chinese Medicine from June 2020 to October 2021. The disease diagnosis was mainly depended on the International Classification of Diseases-10 (ICD-10). For diagnosis of dysphagia: (1) ICD code of various types of dysphagia after stroke; (2) clinical symptoms or medication orders related to dysphagia are found in medical records, such as indwelling gastric tube, semi-liquid diet or liquid diet, prevention of aspiration and drinking test. If one or more of the criteria were met, clinical diagnosis was determined (Malagelada et al., 2015).
This study was prospectively registered (ChiCTR2100041848). Ethical approval was obtained from the Institutional Review Board of Xuanwu Hospital Capital Medical University (No. XW-20210902-1). All patients or their legally authorized representative provided written informed consent.
Inclusion criteria
The inclusion criteria are as follows: (1) Age between 40 and 80 years, and no gender restriction; (2) initial ischemic stroke; (3) with Food Intake Level Scale (FILS) less than seven points; (4) with disease duration less than one month.
Exclusion criteria
The exclusion criteria are as follows: (1) Dysphagia was relieved within two weeks after stroke; (2) with acupuncture treatment less than four times; (3) severe cognitive impairment and aphasia; (4) other diseases that can lead to dysphagia.
Exposure
The two groups of patients received nearly the same basic therapy, such as the antiplatelet aggregation, anticoagulant, lipid-lowering therapy, blood pressure control, and glycemic control, which commonly were used for secondary prevention. “Exposure” refers to acupuncture treatment. Acupuncture prescriptions are Hegu, Quchi, Neiguan, Yanglingquan, Zusanli and Sanyinjiao. We set the patients who did not receive the acupuncture to reflect the natural course of recovery after stroke.
Outcome measurement
Primary outcome was the time to clinical improvement, which defined as a gain three points of the FILS (0–10 points) (Kunieda et al., 2013). Secondary outcomes included: (1) the proportion of patients with clinical improvement in swallowing function; (2) distribution of the modified Rankin Scale (mRS) score at 6 months; (3) the proportion of patients with excellent function (mRS scores 0–2) and favorable function (mRS scores 0–3) at 6 months (Langezaal et al., 2021); (4) adverse events.
Baseline data collection
In our study, demographic information, characteristics related to stroke and baseline diseases were collected. During the 6-month follow-up, we obtained clinical study data by outpatient or telephone interview. Adverse events (AEs) related to acupuncture treatment were recorded, as well as related to basic treatment. Missing baseline data were handled by imputation method. Patients with missing outcome data were counted as non-responders and excluded. We also excluded the patients lost to follow-up.
Statistical analysis
The primary hypothesis of our study was that the acupuncture treatment could shorten the recovery time of patients with post-stroke dysphagia. The 1 : 1 propensity score matching method was used to match the two cohorts. We computed the propensity score by using logistic regression based on age, sex, body mass index, internal-medical diseases, characteristics related to stroke. This method can reduce the difference of baseline data and confounding factors (Austin, 2011). Multiple imputation approach was used for handling missing data (Huque et al., 2018; Li, G. et al., 2020), using all baseline characteristics (age, sex, body mass index, hypertension, diabetes, hyperlipidemia, atrial fibrillation, hyperhomocysteinaemia, Charlson comorbidity index, Toast, ASPECT, mRS, NIHSS, Barthel index, FILS) to generate 5 imputed data sets. And these imputed data were used in sensitivity analyses. Continuous variables were assessed using either the t test or Wilcoxon test where appropriate. Categorical variables were analyzed using χ2 or Fisher exact test as appropriate and risk ratio (RR) and 95% confidence interval (CI) were calculated. For primary outcome, the cumulative incidence of improvement rate at 6 months was estimated using the Kaplan-Meier method and hazard ratio (HR) and 95% CIs were calculated. To assess the relationship between the acupuncture and clinical outcomes, multivariable Cox regression models were executed. Model 1 without adjustment for any covariates. Model 2 included age, sex, BMI. Model 3 added hypertension, diabetes, hyperlipidemia, atrial fibrillation, hyperhomocysteinaemia. Finally, Model 4, the fully adjusted model, included the covariates in Model 3 plus CCI, ASPECT score, NIHSS score, TOAST, FILS score. The level of statistical significance was set at P < 0.05. All statistical tests were conducted using the R studio software (version 4.03).
Results
A total of 1127 consecutive patients from two hospitals were screened for eligibility. Finally, 375 patients were enrolled after screening, 152 of whom in acupuncture group and 223 of whom in control group. Two groups respectively included 129 cases after the 1:1 matching (Fig. 1). There was no significant difference in demographic and stroke characteristics between the two groups (Table 1).
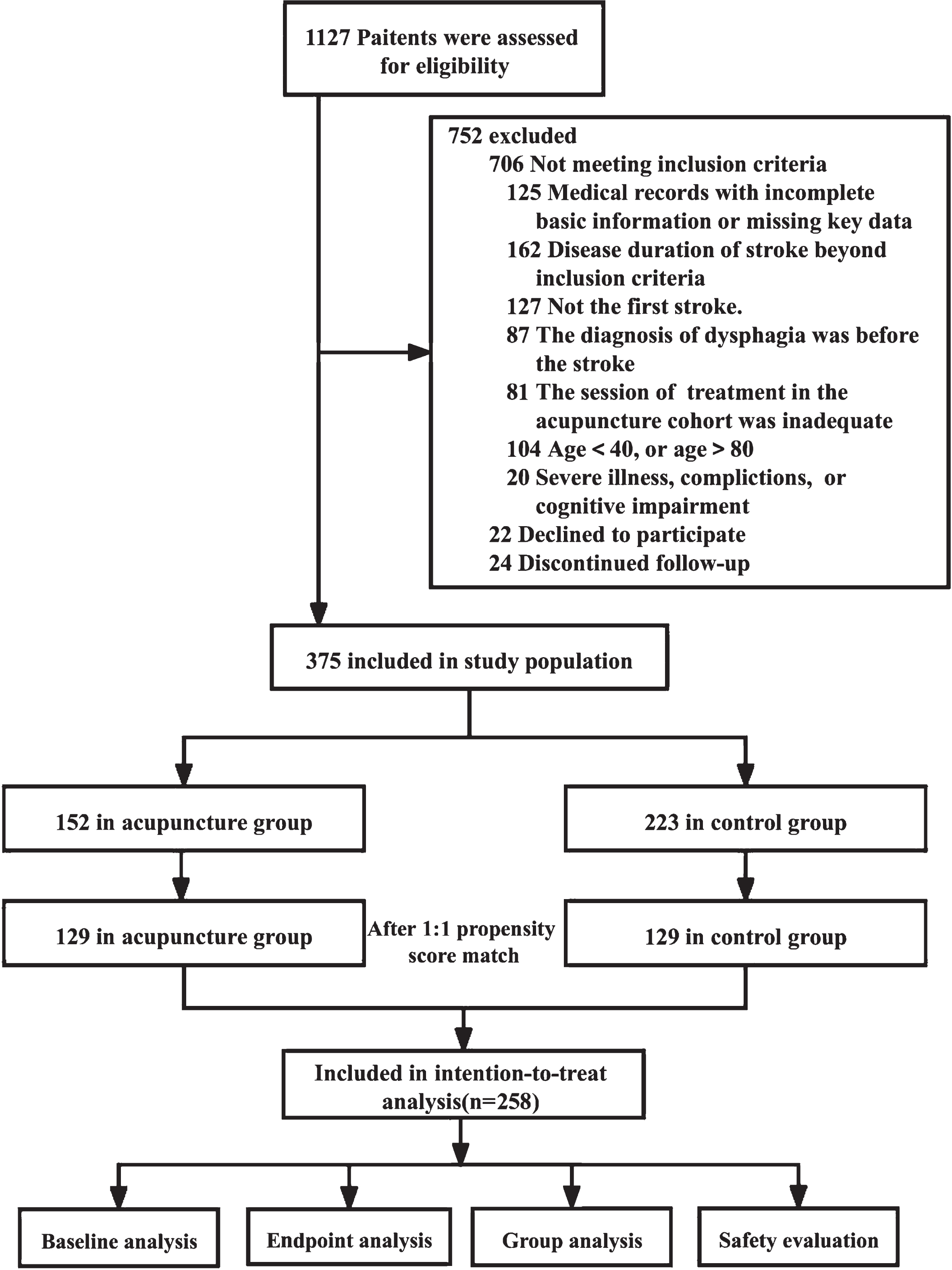
Flowchart of the study population.
Characteristics of included study populations
ASPECT, Alberta stroke program early computed tomography score; CCI, Charlson Comorbidity Index; CE, cardioembolism; FILS, food intake level scale; IQR, interquartile range; LAA, large-artery atherosclerosis; mRS, modified Rankin scale; OD, other determined; SVO small vessel occlusion; Toast, Trial of Org 10172 in Acute Stroke Treatment; UD, undetermined.
In 6-month follow-up, the median time to achieve clinical improvement was 97 days (95% CI, 93–124) in acupuncture group and 119 days (95% CI, 108–145) in control group (Table 2). The Kaplan-Meier curves for the time to clinical improvement are shown in Fig. 2 (HR = 1.48; 95% CI, 1.14–1.92; LogRank, P = 0.003).
Primary and secondary outcomes
Primary and secondary outcomes
mRS indicates the modified Rankin scale; *Scores on the mRS range from 0 to 2; #Scores on the mRS range from 0 to 3.
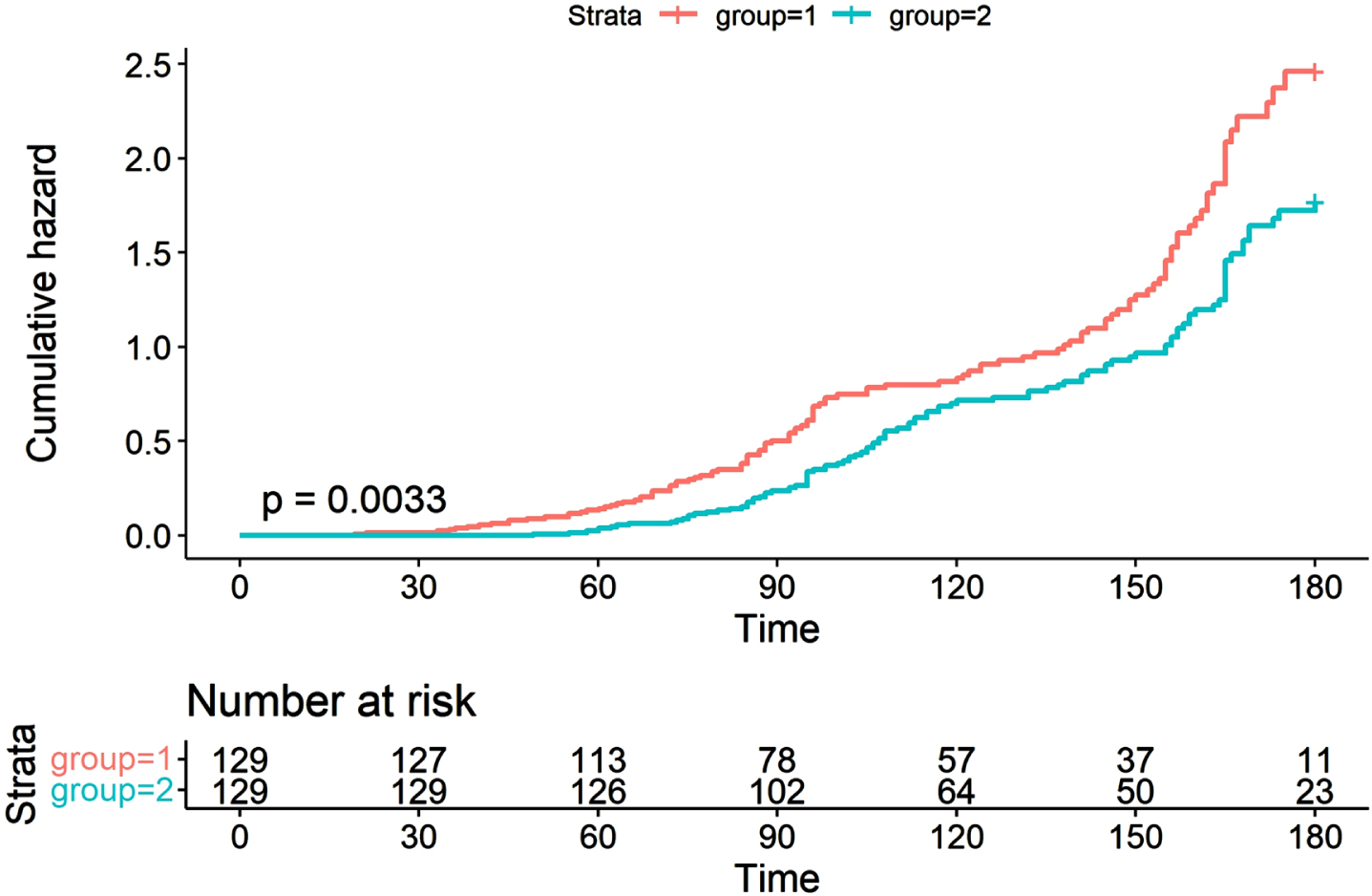
Time to clinical improvement (days). 1 = Acupuncture group, 2 = Control group.
Secondary outcomes are listed in Table 2. 118 patients (91.5%) in acupuncture group and 107 patients (82.9%) in control group achieved clinical improvement (RR = 1.10; 95% CI, 1.05–1.22; P = 0.004). The difference between the two groups was 8.5% (95% CI, 0.4–16.6%; P < 0.05). 78 patients (60.5%) in acupuncture group achieved excellent function (mRS score 0–2) compared to 61 patients (47.3%) in control group (RR = 1.28; 95% CI, 1.02–1.62; P = 0.045), the difference between the two groups was 13.2% (95% CI, 1.1–25.2%; P < 0.05). 106 patients (82.2%) in acupuncture group achieved favorable function (mRS score 0–3) compared to 91 patients (70.5%) in control group (RR = 1.17; 95% CI, 1.02–1.35; P = 0.039). The difference between the two groups was 11.7% (95% CI, 1.4–21.9%, P < 0.05). The distribution of mRS scores at 6 months are shown in Fig. 3 (RR = 1.05; 95% CI, 0.80–1.25; P = 0. 20).

Distribution of mRS scores at 6 months.
Subgroup analysis was performed according to duration of treatment, 87.5 days (95% CI, 84–95) of dysphagia patients in group of duration > 1 month and 109 days (95% CI, 94–123) in group of duration < 1 month, the difference was statistically significant (LogRank, P = 0.005). The primary outcome occurred among 72 of 76 patients (94.7%) in group of duration > 1 month and among 46 of 53 patients (86.8%) in group of duration < 1 month (RR = 1.19; 95% CI, 1.07–1.33; P < 0.05).
Multivariate regression analyses
Table 3 shows the unadjusted and multivariate-adjusted HR and 95% CI. Compared with control group, patients who received acupuncture were at greater probability of recovery (HR = 1.48; 95% CI, 1.14–1.92) in the unadjusted model (Model 1). After adjustment for demographic characteristics (Model 2), a similar association still was observed (HR = 1.66; 95% CI, 1.27–2.18). After additional adjustment for internal-medical diseases (Model 3), the association did not change (HR = 1.62; 95% CI, 1.24–2.14). Finally, in the fully adjusted model (Model 4) for demographic characteristics, internal-medical diseases, characteristics related to stroke, the HR was 1.79 (95% CI, 1.34–2.39) for patients who received acupuncture compared with those who in control group. Similar findings were observed in sensitivity analyses excluding the top 10% recovery time patients in two groups patients (Supplementary Table 2).
Comparison of 6 months outcome between acupuncture group and control group
Comparison of 6 months outcome between acupuncture group and control group
aUnadjusted confounding factors. bAdjusted for age, sex, BMI. cAdjusted for age, sex, BMI, hypertension, diabetes, hyperlipidemia, atrial fibrillation, hyperhomocysteinaemia. dAdjusted for age, sex, BMI, hypertension, diabetes, hyperlipidemia, atrial fibrillation, hyperhomocysteinaemia, CCI, ASPECT, NIHSS, TOAST, FILS.
In fully adjusted models for primary outcome, 13.9% of patients had 1 or more missing covariates, with no significant difference in missingness between groups (acupuncture group = 14.7%, control group = 13.2%; P = 0.86). Models using imputed data to replace missing covariates yielded similar results to the primary models and did not appreciably alter the associations (Supplementary Table 3).
Safety evaluation
Acupuncture-related adverse events occurred in 38 patients in acupuncture group, among which pain was the most common (36 patients, 27.9%). Beyond that, gastrointestinal symptoms occurred in 16.3% of the patients in the acupuncture group and 15.5% in the control group (P > 0.99). There was no significant difference in the incidence of lung infection and stroke recurrence between groups. The results are shown in Table 4.
Adverse events
Adverse events
NA, not applicable.
In this study, we assessed the efficacy of acupuncture on the recovery of swallow function. The time of dysphagia to clinical improvement was shortened in the acupuncture group compared with the control group (HR = 1.48; 95% CI, 1.14–1.92; P < 0.05), which indicated that acupuncture could promote the recovery of dysphagia after stroke. The proportion of clinical improvement at 6 months was higher in the acupuncture compared with the control group (RR = 1.10; 95% CI, 1.05–1.22; P < 0.05). Consistent with a previous research (Lu et al., 2021), the results showed that acupuncture can be effective in the treatment of post-stroke dysphagia. In terms of life quality, the proportion of excellent function and favorable function of mRS scores in the acupuncture group increased compared with the control group, suggesting that acupuncture can reduce the degree of disability and improve the life quality, which is consistent with the another study (Zhang et al., 2015).
There have been studies (Gordon et al., 1987) showed that 30–40% post-stroke patients suffered transient dysphagia, which may be related with compression of local brain tissue caused by edema. In this situation, dysphagia will be alleviated with the attenuations of edema. For this reason, we excluded patients whose dysphagia relieved rapidly within 2 weeks after stroke. On the other hand, given that the short duration of acupuncture treatment is insufficient to produce effect of neuromodulation, patients with duration time less than 4 were excluded.
Most studies focused on the short-term effect of acupuncture treatment, but failed to analyze whether acupuncture can make a continuous efficacy to influence the long-term outcomes. By prolonging follow-up and observation period, our study overcame the shortcomings mentioned above. Not only the time to clinical improvement, but the recovery incidence was analyzed. Besides, the distribution of mRS score, the proportion of excellent function and favorable function between groups were analyzed to evaluate the difference in life quality. Multiple aspects of analyses and comparisons make our conclusions more reliable.
Neural plasticity is essential for the recovery of swallow function (Li et al., 2019). Recent studies showed that acupuncture can regulate neuroplasticity (Li et al., 2020). As a non-invasive neural regulation technique, it can be used to treat various diseases, especially the neurological diseases. Several studies have identified that pinprick at Waiguan point can restore the balance of interhemispheric interaction (Censor et al., 2012; Chen et al., 2014). Accelerating nerve regeneration may be another possible mechanism. By up-regulating the expression of basic fibroblast growth factor, epidermal growth factor and brain-derived neurotrophic factor, acupuncture could provide a favorable microenvironment of the brain for proliferation and differentiation of neuronal stem cells (Kim et al., 2014). Acupuncture can repair the interruption of synaptic connections, contributes to axon regeneration (Jin et al., 2019; Yang et al., 2021), and promote the extension of injured corticospinal tract (Ahn et al., 2016). Moreover, acupuncture can protect the motor neurons of hypoglossal nucleus, strengthen the peripheral muscles involve the swallowing reflex, reduce the threshold intensity of contractions of tongue muscle after hypoglossal nerve injury (Cui et al., 2020).
Subgroup analysis for duration time of treatment showed that patients with duration time exceeding one month are more likely to recover from dysphagia, which may be related with the process of regulating neuroplasticity requires a specified time. Furthermore, our results found that the efficacy of acupuncture group is always better than control group at multiple time points during the 6 months follow-up. Whether acupuncture can prolong the time window of synaptic plasticity requires further study.
This study has several limitations. First, some clinical data were collected retrospectively, which increased the risk of recall bias. Second, according to the characteristics of “syndrome differentiation”, it was inevitable to be different in selection of acupoints. As a result, acupoint prescriptions fails to adhere to the standardized design. Third, the times from stroke onset to admission, a key element typically affect the recovery of stroke, cannot be included in the analyses due to lack of relevant information.
Conclusion
This study indicates that acupuncture can facilitate recovery of post-stroke dysphagia and has a better long-term outcome, as it reduces the degree of disability and improves life quality.
Footnotes
Acknowledgments
The first author thanks Siyuan Hou who helped prepare the tables and figures.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This study was supported by grants from the Traditional Chinese Medicine Science and Technology Development Project of Beijing, No. JJ-2020-66.