
Abstract
BACKGROUND:
Acquired brain injury (BI) is associated with negative mental health outcomes for both people with BI, their caregivers (CG), and patient-CG dyads, which may be mitigated through increased resilience. However, little is known regarding the efficacy of resilience interventions focused on CGs of individuals with BI, as well as dyads, which may be instrumental for positive outcomes.
OBJECTIVE:
To systematically review the evidence of the efficacy of resilience interventions focused on CGs and/or dyads of individuals with BI.
METHODS:
A search of MEDLINE, Embase, APA PsycINFO, CINAHL with Full Text, Scopus, SCIE, and ESCI was conducted. Each title and abstract were screened by two authors independently. Each full text review, study data extraction, and study quality assessment was performed independently by two authors. Study quality was assessed using the Joanna Briggs Institute (JBI) critical appraisal tool.
RESULTS:
Out of 11,959 articles retrieved, 347 full text articles were assessed for review and 18 met inclusion criteria for data extraction and quality assessment. Resilience interventions were stratified into 5 different categories based on the type of intervention.
CONCLUSION:
This systematic review suggests that dyadic/CG resilience interventions may improve mental health related outcomes, but conclusions were limited secondary to heterogenous outcomes and lack of a standardized resiliency construct. Future efforts are compulsory to create a standardized resiliency construct and associated outcomes focused on persons with BI, their CGs, and dyads.
Introduction
Acquired brain injury (BI), including stroke, brain tumor (BT), and traumatic brain injury (TBI), are important causes of long term disability in the United States (Benjamin et al., 2019; Dunbar et al., 2018; Schneider, Wang, Gottesman, & Selvin, 2021; Thakkar, Greenwald, & Patel, 2020). While advancements in care have significantly improved mortality in these populations, there continues to be a need to address the substantial emotional distress that often accompanies these conditions for both patients and their caregivers (CGs) (McCurley et al., 2019). Rates of clinically significant anxiety, depression, and posttraumatic stress are high for both patients and CGs during hospitalization after BI and up to 6 months after discharge (McCurley et al., 2019; Meyers et al., 2020; Shaffer, Riklin, Jacobs, Rosand, & Vranceanu, 2016). In individuals after stroke, this is correlated with poorer medical adherence, slower recovery, higher mortality, worse cognitive, functional, and dependency status, and ultimately increased need of CG assistance (Gyawali et al., 2020; van Rijsbergen, Mark, Kop, de Kort, & Sitskoorn, 2019). Simultaneous CG emotional distress may reduce the CG’s ability to provide sufficient assistance to individuals with BI, which may further negatively impact outcomes (McCurley et al., 2019; Shaffer, Riklin, Jacobs, Rosand, & Vranceanu, 2016). Moreover, the distress of an individual with BI may increase the CG’s own psychological suffering and risk of morbidity and mortality (McCurley et al., 2019; Meyers et al., 2020). The negative effects that emotional distress has on individuals with BI and their CGs warrants investigation into areas for prevention and treatment.
The National Institute of Health (NIH) defines resilience as a dynamic process where individuals or teams exhibit a positive behavioral adaptation after encountering adversity or trauma (Luthar & Cicchetti, 2000). The inverse relationship between stress and resilience has led to the hypothesis that the qualities that contribute to resilience may be capable of limiting the intensity of stress, and in doing so, may mitigate many of the associated negative outcomes (Gyawali et al., 2020). For example, in individuals with TBI of various severity, self-reported resilience has been found to be associated with participation outcomes as well as improved quality of life (QOL) (Losoi et al., 2015; Vos et al., 2019). Moreover, rather than being only a characteristic associated with a particular personality trait, resilience is increasingly being understood as a characteristic that can be developed after adversity (Chmitorz et al., 2018). Meaning that one can learn to be resilient and exhibit positive behavioral adaptations after adverse events. This understanding has led to the development of resilience interventions across multiple different patient populations with evidence that resiliency is modifiable and obtainable, rather than a static attribute (Joyce et al., 2018; Leppin et al., 2014). Thus, it is possible that interventions focused on improving resilience can thereby improve outcomes for both individuals with BI, their CG, and the patient/CG dyad.
Prior research focusing on interventions to mitigate emotional distress after BI in general has largely focused on either individuals with neurological impairments or their CG, with little attention to the dyad and interdependence that may be foundational for positive outcomes (McCarthy et al., 2020). It has not been until recently that the dyadic approach has started to come under query in the BI population, with evidence that the brain injury patient and their informal caregiver are interdependent and therefore psychological factors of one effect the other (McCurley et al., 2019; Meyers et al., 2020). Due to these findings, the American Heart Association has emphasized the need for dyadic interventions targeting psychosocial outcomes such as depression, anxiety, social function, physical function, and health-related QOL (Bakas et al., 2014; Pan et al., 2019). As far as interventions focused on improving emotional distress outcomes for CGs or dyads after BI, several systematic reviews have been conducted including a systematic review of general interventions for caregivers of TBI (Baker et al., 2017; Kreitzer, Kurowski, & Bakas, 2018), psychological interventions for patients after stroke (Panzeri, Rossi Ferrario, & Vidotto, 2019), as well as interventions to support CGs of people with BTs (Boele et al., 2019). However, there is limited evidence specifically for resilience interventions designed to promote a positive behavioral adaptation after adversity as compared to a solely support/education intervention in the dyads of individuals with BI and their CG. The purpose of this systemic review was to assess the efficacy of the current dyadic or CG resilience interventions and to inform future interventions/research among BI dyads and their CGs.
Methods
Protocol and registration
We conducted a systematic review to study the effectiveness of resilience interventions among CGs and dyads of persons with BI. The reporting of this study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2015). The study protocol was registered with PROSPERO (CRD42021260182).
Data sources and search strategy
The medical librarian (EAKV) searched electronic health and science literature databases and a clinical trial register on 23-24 June 2021. The names and dates of the databases are provided in the Supplementary Materials. Science Citation Index Expanded (SCIE) and Emerging Sources Citation Index (ESCI) were searched simultaneously via the Web of Science search platform. Three known relevant studies were used to identify records within MEDLINE. Candidate search terms were identified by looking at words in the titles, abstracts, author keywords, and subject indexing of those records. Yale MeSH Analyzer was used to compare and select key search terms. Search concepts included traumatic brain injury, stroke, brain neoplasms, and resilience therapies. Search strategies were formulated using a combination of standardized index terms and keywords. The final search strategy was tested by whether it could retrieve the 3 relevant studies in MEDLINE. Search filters for randomized controlled trials were applied in MEDLINE (Study design search filters, 2021), Embase ("Study design search filters,” 2021), APA PsycINFO (Dennett, 2020), CINAHL with Full Text (Glanville et al., 2019), Scopus (Searching Scopus for “Randomised Controlled Trials”, 2021), SCIE (Tjosvold, 2018), and ESCI (Tjosvold, 2018). Filters for adult populations were applied in databases except for EBM Reviews and the Cochrane Central Register of Controlled Trials. No date or language limits were applied to any of the search results. Complete search strategies are provided in the Supplementary Materials. A total of 11,959 records were retrieved via database and register searches and exported to EndNote. References from EndNote were imported to Covidence. 3,694 duplicate references were identified and removed using the Covidence automated deduplication feature; 8,265 records were delivered to the systematic review team for screening (Covidence systematic review software).
Study selection
The inclusion criteria were the following: 1) Patient population was dyads of persons with BI and/or their CGs greater than 18 years of age; 2) Article was primarily studying a resilience intervention; 3) Primary outcomes were mental health related and associated with improved resilience; and 4) Trial design included a resilience intervention with pre- and post-intervention outcomes as well as a comparison group. BI was defined as an injury to the brain that is not hereditary, congenital, degenerative, or induced by birth trauma, and included TBI of all severity including mild TBI and concussion, primary and secondary brain neoplasm, anoxic BI, intracerebral or intracranial hemorrhage, ischemic stroke, hemorrhagic stroke, and subarachnoid hemorrhage. Resilience was defined as a dynamic process when individuals, teams and systems exhibit positive behavioral adaptation when they encounter significant adversity or trauma (Luthar & Cicchetti, 2000). By this definition, resilience interventions included those studies classifying themselves specifically as a resilience intervention but also included the following: mind-body interventions, mindfulness interventions, stress management interventions, psychoeducational interventions, peer support interventions, and skills training interventions. Interventions were classified as a resilience intervention if a primary focus of the intervention was on positive behavioral adaptation rather than a focus on receiving static support or education relating to the condition only. Outcomes were included if they targeted health maintenance, coping, and preventative or protective pathways indicative of positive behavioral adaptation, including but not limited to measures of stress, quality of life (QOL), mood/anxiety symptoms, coping skills, self-efficacy, and direct resilience outcomes.
The exclusion criteria were the following: 1) Age <18 for both dyads with BI and CGs; 2) Article did not primarily study a resilience intervention (not focused on developing positive behavioral adaptation); 3) No pre- and post-intervention outcome measures; 4) No comparison group; 5) Primary outcome measures focused on physical/cognitive outcomes including but not limited to measures of balance, spasticity, gait, endurance, strength, fatigue, cognition; 6) Case reports; 7) Animal studies; 8) Study protocols or abstracts; and 9) Article only focused on patients with BI, without discussion about CGs or dyads.
Each title and abstract were reviewed by 2 authors independently to determine eligibility for full-text review via Covidence Software. If the inclusion criteria were not fully clear from the abstract screening, the article was included for full-text review. Two authors reviewed each full text article, and any disagreements were then settled based on mutual consensus of all authors. All 5 authors reviewed titles, abstracts, and full texts.
Data extraction
Decisions on which variables to extract from the studies were decided based on mutual consensus of all coauthors, and each study that met inclusion criteria was reviewed by 2 authors independently (E.A.H. reviewed all). Discrepancies in data abstraction were resolved by mutual consensus. The following were abstracted: article title, author name, study date, study aim, study design, intervention description, intervention setting, intervention delivery, number of participants in intervention group, intervention group age, sex, ethnicity, primary outcome measures, and authors’ summary of findings. A summary of all included study characteristics are in Table 1.
Summary of included CG and dyadic resilience interventions characteristics and findings
Summary of included CG and dyadic resilience interventions characteristics and findings
The methodological quality of each study was assessed independently by two coauthors using the Joanna Briggs Institute (JBI) critical appraisal tool (Joanna Briggs Institute, 2017). The following were assessed: true randomization, concealed allocation, similarity between groups as baseline, blinding, variation between control and treatment aside from the intervention, appropriate assessment of loss to follow-up, intention-to-treat analysis, appropriate outcome measurements for both control and treatment, reliability of measurement tools, appropriate statistical analysis, and assessment of deviations from RCT design. Discrepancies were resolved based on mutual consensus of all authors. A scoring system was decided based on mutual consensus as well, as there is no standard scoring system for the JBI appraisal tool. The maximum score for the modified checklist was 13 with all individual items rated as either yes (=1) or no/unclear (=0). Scores were grouped into 3 categories based on mutual consensus into the following: good (10–13), fair (5–9), and poor (0–4) (Table 2).
JBI quality assessment for risk of bias in studies [SOURCE]
JBI quality assessment for risk of bias in studies [SOURCE]
Quality assessment statements as charted above: A. True randomization used for assignment of participants to treatment groups. B. Allocation to treatment groups concealed. C. Treatment groups similar at the baseline. D. Participants blind to treatment assignment. E. Those delivering treatment blind to treatment assignment. F. Outcomes assessors blind to treatment assignment. G. Treatment groups treated identically other than the intervention of interest. H. Follow up complete, but if not, differences between groups in terms of their follow up adequately described and analyzed. I. Participants analyzed in the groups to which they were randomized. J. Outcomes measured in the same way for treatment groups. K. Outcomes measured in a reliable way. L. Appropriate statistical analysis used. M. Trial design appropriate, and any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial.
Study selection and characteristics
Of the 8,265 abstracts identified, 347 were selected for full text review, and 18 met inclusion criteria, as shown in the PRISMA flowchart (Fig. 1). Of the 18 studies included, 15 were randomized controlled trials (RCT) (Backhaus et al., 2016; Backhaus et al., 2010; Bannon et al., 2020; Boele et al., 2013; Draper et al., 2007; Fortune, Rogan, & Richards, 2016; Inci & Temel, 2016; King et al., 2012; Lester et al., 2021; Milbury et al., 2019; Milbury et al., 2020; Robinson-Smith et al., 2016; Smith et al., 2012; Tielemans et al., 2015; Vranceanu et al., 2020; J. Wang et al., 2021; Wilz & Barskova, 2007; Yilma et al., 2019). Of these RCTs, 7 were pilot/feasibility studies, (Backhaus et al., 2010; Bannon et al., 2020; Boele et al., 2019; Lester et al., 2021; Milbury et al., 2019, 2020; Vranceanu et al., 2020; J. Wang et al., 2021) and 3 were wait-list control studies (Draper et al., 2007; King et al., 2012; Milbury et al., 2019). Out of the 3 additional studies, 1 was a 3-group quasi experimental study, (Wilz & Barskova, 2007) 1 was a 2-group quasi experimental pilot study, (Robinson-Smith et al., 2016) and 1 was an unrandomized wait-list control study (Fortune et al., 2016). The interventions varied in design, population type, setting, delivery, duration, and follow-up period (Table 1). Thirty-eight percent of the studies focused on CGs only, and 62% included dyads. Because our review focused on the resilience definition more broadly, we characterized the resilience interventions into 5 different intervention types: 1) mindfulness/relaxation (22%); 2) psychoeducation (11%); 3) skills training that consisted of coping, problem solving, self-management, behavioral therapy skills (33%); 4) peer support (6 %); and 5) mixture of 1–4 interventions (28%).
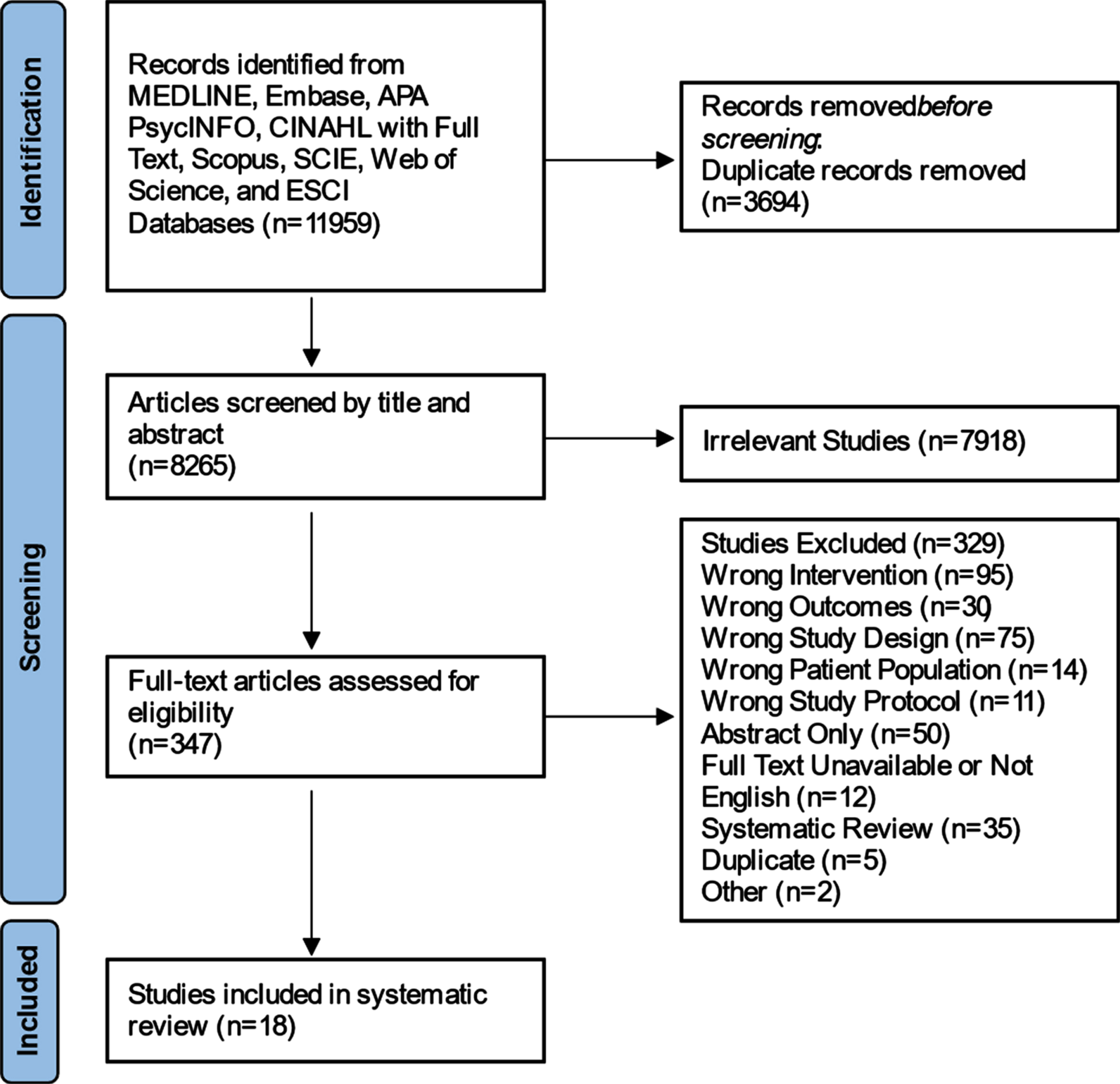
Flow diagram of included studies.
In general, the study populations were predominantly female CGs, middle to late aged and mostly white participants (however, over half of the studies did not report race or ethnicity). The majority of studies had a stroke patient population (56%); however, 17% of studies focused on dyads/CG with BT, 28% had a patient population that was either multiple types of BIs (17%) or were ICU patients that largely included brain injury patients but were not exclusive to BI (11%).
Seventy-eight percent of the interventions were delivered in the outpatient setting and the rest were delivered in either the ICU or an acute rehabilitation unit. Fifty-six percent of studies had an in-person intervention delivery method, 11% were web-based intervention delivery only, 28% were a combination of in-person and web-based intervention delivery, and 6% did not describe the intervention delivery method.
Intervention length varied from 4 weeks to 12 months. The average length of time was approximately 12 weeks with the median being 9 weeks. The total number of hours per intervention varied from 3 hours to 36 hours. The average hours/intervention of the provided data was 15. Follow-up varied from no follow-up (11%) to 9 months post-intervention.
The risk of bias was rated as poor for 2 studies, fair for 12 studies, and good for 4 studies (Table 2). Out of the 18 included studies, 3 of those included participants who were blinded to study intervention (Lester et al., 2021; Tielemans et al., 2015; Vranceanu et al., 2020), no studies included blinding to those delivering treatment, and 4 studies included outcome assessors that were blinded to treatment assignment.All 4 studies rated as ‘good’ were RCTs of either mixed interventions or skilled training interventions. Two out of four studies that were rated as ‘good’ did not report statistically significant results when compared to control for the resilience outcome we were assessing (King et al., 2012; Lester et al., 2021). The other two studies did report statistically significant results (Smith et al., 2012; Vranceanu et al., 2020).
Main results of individual studies
The majority of studies, apart from two, assessed at least one of the following outcomes: psychological distress, QOL, and/or CG burden (Inci & Temel, 2016; Tielemans et al., 2015). Other outcomes included coping, self-efficacy, family functioning/stressors, wellbeing measures (e.g., compassion, mindfulness, intimacy), and interpersonal interactions. Seventy-eight percent of the interventions had at least one significant resilience outcome for either CG or dyad. Details of the included studies including primary outcomes and results can be seen in Table 1. Though no meta-analysis was performed secondary to the heterogeneity of outcomes, the authors did not find a clear correlation between significant findings reported across the studies and associated intervention type, population type, setting, delivery method, or duration of study. Below are descriptions of studies that were categorized into each intervention category.
Outcomes of mindfulness/relaxation interventions
Two studies were RCTs with a mindfulness/progressive muscle relaxation intervention for CG of a stroke patient population in an outpatient setting (Wang et al., 2021; Yimaz et al., 2019). The studies were conducted over 12 months and 8 weeks respectively, and both for a total of 36 hours. Both studies measured depression and CG burden, and Wang et al. also measured anxiety. Wang et al. measured outcomes at 3 months, 6 months, and 12 months, and a significant difference was seen for all outcomes starting at 6 months post-intervention. This differed from Yimaz et al. where there was no follow up besides immediately post-intervention. These two studies also differed in the delivery method - Wang et al. employed an in-person intervention, and while the training in the Yilmaz et al. study was in-person, the actual intervention was self-conducted via voice recorded Compact Disk.
Two studies were RCTs with mindfulness-based interventions for CGs of a glioma patient population in an outpatient setting (Milbury et al., 2019, 2020). One study focused on mindfulness through movement in a yoga intervention (Milbury et al., 2019), whereas Milbury et al. (2020) studied mindfulness through meditation. The yoga intervention was conducted as an in-person intervention and the meditation intervention was delivered via FaceTime. The studies were conducted over 4–6 weeks for a total of 9 and 4 hours, respectively. Both studies included measurements of depressive symptoms; however, Milbury et al. (2019) also measured overall QOL and Milbury et al. (2020) measured wellbeing outcomes. The yoga intervention showed significantly decreased depression in CGs and increased mental QOL for the dyad. The meditation intervention only showed significant change in compassion and intimacy wellbeing measures in patients.
Outcomes of psychoeducation interventions
Quasi-experimental studies with a psychoeducation-only intervention for CGs of a stroke patient population in a rehabilitation hospital (Robinson-Smith et al., 2016) and outpatient setting (Wilz & Barskova, 2007) included in-person interventions. Wilz et al. studied CGs only over a 7.5 month duration for a total of 22.5 hours with a 6 month post-intervention follow up. Robinson-Smith et al. delivered 6 tailored sessions over 6 weeks with exact hours of intervention unknown and only post-intervention follow up at 6 weeks. Depression and QOL were measured in both studies; however, Wilz et al. also measured anxiety and Robinson-Smith et al. also measured coping. Wilz et al. showed immediate improvement in anxiety but it took 6 months after intervention to see significant changes in depression and psychological QOL in CGs. Robinson-Smith et al. found significant improvements in coping in the dyad, but only patients had improvements in depression and QOL.
Outcomes of skills training interventions
Tielmans et al., Smith et al., Lester et al., Bannon et al., Vranceanu et al., and Draper et al. all conducted RCTs with a skills training intervention for CGs of stroke and ICU populations in both the outpatient and ICU settings (Bannon et al., 2020; Draper et al., 2007; Lester et al., 2021; Smith et al., 2012; Tielemans et al., 2015; Vranceanu et al., 2020). These interventions mainly consist of coping, problem solving, self-management skills, and behavioral therapy skills. Delivery method varied and included in person, web-based, and a combination of in person and virtual sessions. Intervention duration varied from 4 weeks to 11 weeks with a total of 3–14 hours. Outcomes measured included coping, psychological distress, QOL, mindfulness, self-efficacy, interpersonal bond, and CG burden. There was not one commonly assessed outcome among all skills intervention training studies. Lester et al., Bannon et al., and Vranceanu et al. all used the same “recovering together” intervention which was described as a skills-based dyadic intervention targeting emotional distress in the survivor and CG through cognitive behavioral therapy and dialectical behavior therapy. Outcomes assessed were self-efficacy, mindfulness, coping skills, and intimate bonds between partners (Bannon et al., 2020; Lester et al., 2021; Vranceanu et al., 2020). Two studies found significant improvement in psychological distress for the dyad (Bannon et al., 2020; Vranceanu et al., 2020). Only Vranceanu et al., found the results were sustained at 3 months Lester et al. showed no significant results after 6 weeks when only assessing QOL. Draper et al. only measured outcomes in CGs with significant improvement in psychological stress in that was not sustained at 3 months. Similarly, Smith et al. employed an intervention that was web-based and outcomes were measured for dyads with significant improvement in depression only in CGs, not patients. Tielaman et al. did not find any significant findings related to coping outcomes.
Outcomes of peer support interventions
Only one study included a peer support intervention (Inci & Temel, 2016). This was a RCT in the stroke patient population in an outpatient setting. The intervention was delivered in person only to CGs and outcomes included family stressors, strain, support, coping, hardiness, and distress. Results revealed a significant difference between the experimental and control group’s follow-up test scores for relative and friend support, social support, and family-coping coherence. A significant difference was found between the experimental group’s mean pretest, posttest and follow-up test scores in terms of family strain, relative and friend support, social support, family coping coherence, family hardiness and family distress (Inci & Temel, 2016).
Outcomes of mixed interventions
King et al., Fortune et al., Boele et al., Backhaus 2010 et al., and Backhaus 2016 et al. all delivered combinations of interventions (Backhaus et al., 2016; Backhaus et al., 2010; Boele et al., 2013; Fortune et al., 2016; King et al., 2012; Vranceanu et al., 2020). The interventions included a combination of psychoeducation, cognitive behavioral therapy, skills training, mindfulness, and/or peer support. All but Fortune et al. were RCTs and the delivery method varied across the studies. Vranceanu et al. and King et al. delivered an intervention via a mixture of in-person and web-based versus telephone, respectively (King et al., 2012; Vranceanu et al., 2020). Fortune et al. did not describe a delivery method and Backhaus et al. delivered the interventions in-person (Backhaus et al., 2016, 2010; Fortune et al., 2016). Intervention duration varied from 6 weeks to 16 weeks with a total ranging from 6 hours/intervention to 32 hours/intervention. Outcomes measured included psychological distress, QOL, self-efficacy, and CG burden. There was not one commonly assessed outcome among all studies. Backhaus et al. 2010 and 2016 showed significant improvement in self-efficacy that was sustained at 3 month post-intervention follow up. Psychological distress was not significantly different over time; however, it did remain stable over the follow up period compared to the control group in which there was an increase in psychological distress at 3 months (Backhaus et al., 2016, Backhaus et al., 2010).
Discussion
The goal of this systematic review was to assess the efficacy of resilience interventions in dyads of individuals with BI and their CGs. While several prior systematic reviews have evaluated general self-management strategies and broad interventions targeted on the CGs and dyads of persons with BI, this systematic review is the first to our knowledge that attempted to understand and synthesize resilience interventions in BI as it relates to CGs and dyads. Systematic reviews assessing the efficacy of resilience interventions have shown benefit in a variety of adult patient populations; however, the inclusion criteria have been limited to almost exclusively cognitive behavioral therapy and/or mindfulness programs and have primarily focused on the patient rather than the interdependence of the dyad (Joyce et al., 2018; Leppin et al., 2014; Ludolph et al., 2019). Persons with BI represent a patient population with individual recovery trajectories and unique neurobehavioral changes along with cognitive and physical impairment that make both the delivery and efficacy of resilience interventions potentially unique in this population. Given the association of an individual’s resilience and various outcomes after BI, the possibility of a modifiable factor that can positively influence emotional outcomes has important implications (Losoi et al., 2015; Vos et al., 2019).
Although 78% of studies reported a significant improvement in at least one outcome for either CGs or dyads, the certainty in the evidence that resilience interventions are beneficial in this population is low (Murad, 2017). This is secondary to several factors including a lack of a consistent resilience construct and resulting differences in intervention types, heterogeneity in outcomes relating to resilience, small individual sample sizes, and an overall high risk of bias. We defined resilience as “a dynamic process when individuals, teams and systems exhibit positive behavioral adaptation when they encounter significant adversity or trauma,” a definition that conceptualizes resilience not as a personality trait or static attribute but rather as a modifiable characteristic (Luthar & Cicchetti, 2000). The resilience definition that we chose thus resulted in expanding our intervention search to include not only studies that were described as resilience interventions, but also mind-body interventions, mindfulness interventions, stress management interventions, psychoeducational interventions, peer support interventions, social support interventions, positive psychology, and wellbeing interventions. There were only 4 studies found that described their interventions as resilience interventions (Bannon et al., 2020; Inci & Temel, 2016; Lester et al., 2021; Vranceanu et al., 2020). Of these studies, no resilience specific outcome (e.g., Connor Davidson Resilience Scale, Brief Resilience Scale, The Resilience Scale for Adults) was included to distinguish them from the other interventions (Windle, Bennett, & Noyes, 2011). In addition, the intervention components were overall consistent with other interventions in the 5 categories (mindfulness/relaxation, psychoeducation, peer support, skills training, or mixed intervention). Because these studies did not have any unique intervention components relating to the construct of resilience, they were incorporated into the 5 broad intervention categories.
When synthesizing all interventions together, due to the scarcity in the literature and the large amount of heterogeneity between the studies, drawing conclusions regarding efficacy of the interventions was limited. However, classifying the interventions into several categories allowed for a clearer assessment. Relaxation interventions seemed to require at least 6 months of intervention to see significant changes in a resilience outcome, (Wang et al., 2021) while mindfulness studies supported the idea that increased frequency of sessions provides more significant benefit (Milbury et al., 2019; Milbury et al., 2020). For psychoeducational interventions, it is possible that a longer duration intervention with longer follow up is necessary to see emotional distress changes in both partners of the dyad (Robinson-Smith et al., 2016; Wilz & Barskova, 2007). Results of skills training interventions seemed to support that these interventions were most beneficial for only psychological distress outcomes, with unclear long-term benefits (Bannon et al., 2020; Draper et al., 2007; Lester et al., 2021; Smith et al., 2012; Tielemans et al., 2015; Vranceanu et al., 2020). Finally, when the intervention included a combination of different design types, there was some evidence that starting an intervention in the acute phase of injury has more benefit for psychological distress in the dyad (Backhaus et al., 2016; Backhaus et al., 2010; Boele et al., 2013; Fortune et al., 2016; King et al., 2012). This idea was supported by McCurley et al., where 24 different dyads were interviewed, and the participants agreed that starting an intervention while still in the acute hospital was likely most ideal (McCurley et al., 2019). However, this was based on qualitative data, and the current literature has conflicting information regarding a true critical period when an intervention is optimal (Meyers et al., 2020; Shaffer et al., 2016). Future studies are needed to further assess the optimal time for initiation of a resilience intervention.
There are multiple limitations of the literature included in this systematic review. Many of the studies were pilot studies that had small sample sizes resulting in limited power. While a majority of the studies (12/18) did conceal allocation to treatment groups, only a few (3/18) blinded participants to treatment group; 4/18 blinded outcome assessors to treatment assignment; and no studies meeting inclusion criteria blinded those delivering interventions to treatment assignment. There was concern for generalizability as most study participants across studies were White, middle-aged, and well-educated. In addition, most studies excluded individuals with cognitive or language impairments. Future studies are needed to understand the best way to deliver resilience interventions given the high incidence of cognitive and language impairment in the BI population. There was also concern for high dropout rates with no intention to treat analysis in 9/18 studies, lack of long term follow up in many, lack of valid measurement tools, lack of tailored interventions, use of waitlists versus true controls, and CG-only assessments.
There were several limitations within the systematic review as well. While we utilized a standard definition for resilience that is supported by the NIH, there are multiple different definitions used in the literature. The construct of resilience is dynamic and complex with no consensus, making it hard to create an operational definition that can be used to then measure changes in resilience. Our search criteria was broad, which allowed us to categorize a wide number of studies apart from those classifying themselves as a resiliency intervention, of which there were only 4 studies found. While this broad criterion is a strength of the study given the otherwise limited literature in this area, the lack of a unifying consensus likely leads to inclusion of potentially irrelevant articles and excluding salient ones during the review process. Ultimately, any discrepancies for including an intervention based on whether it met the definition of resilience was decided based on mutual consensus of all authors, which helped with internal consistency. The NIH has identified the need for a comprehensive resilience research model and since 2019 has been attempting to pave the road for future resilience programs and research (National Institutes of Health: Office of Dietary Supplements, n.d.). As part of this, a “Resilience Research Design Tool” has been identified as a best practice for designing studies intended to target resilience outcomes. This model includes recommendations that the experimental design includes a stressor or challenge (such as a high risk condition), measurements and/or outcomes targeting health maintenance or preventative pathways, and an intervention that has multiple diverse effects within a system or across multiple systems. This type of design model may be considered for future interventions within the BI population (Luthar & Cicchetti, 2000).
Lastly, we included studies with primary outcomes that addressed a form of positive adaptation through preventative or protective pathways, and ones focused on mental health outcomes. The lack of standardization for the outcomes lead to studies using different measurement tools, some of which are not validated, to assess similar results. The decision to include/exclude study outcomes was based on a consistent and mutual consensus of all authors, though resulted in increased heterogeneity between the studies that made it challenging to synthesize results. While there are several resilience specific scales that have been used across a variety of resilience interventions, there is no current standard resilience outcome measurement (Windle et al., 2011). Importantly, no included studies used any resilience-specific outcome measure, regardless of intervention type.
Conclusion
Our systematic review suggests that dyadic/CG resilience interventions in the BI population may be beneficial in improving related mental health outcomes, but due to the lack of a standardized resilience construct and heterogeneous outcomes, conclusions are limited. The positive trends in this review, as well as others, supports that resilience indeed is modifiable, (Leppin et al., 2014) and may in turn lead to improved outcomes after BI. Future study should include efforts to incorporate a standardized resilience research design with consistent outcome measures that can be used across BI populations. Further research that explores the ideal intervention type, duration, delivery method, and setting is needed.
Conflict of interest
The authors do not have any conflicts of interest to declare.