
Abstract
BACKGROUND:
Older adults have the highest traumatic brain injury (TBI)-related morbidity and mortality, and rates in older adults are increasing, chiefly due to falls.
OBJECTIVE:
This study used hierarchical linear modeling (HLM) to examine baseline predictors of functional independence trajectories across 1, 2, 5, and 10 years after TBI in older adults.
METHODS:
Participants comprised 2,459 individuals aged 60 or older at the time of TBI, enrolled in the longitudinal TBI Model Systems database, and had Functional Independence Measure Motor and Cognitive subscale scores and Glasgow Outcome Scale-Extended scores during at least 1 time point.
RESULTS:
Functional independence trajectories generally declined over the 10 years after TBI. Individuals who were older, male, underrepresented minorities, had lower education, were unemployed at time of injury, had no history of substance use disorder, or had difficulties with learning, dressing, and going out of the home prior to the TBI, or longer time in posttraumatic amnesia had lower functional independence trajectories across at least one of the functional independence outcomes.
CONCLUSION:
These predictors of functional independence in older adults with TBI may heighten awareness of these factors in treatment planning and long-term health monitoring and ultimately as a way to decrease morbidity and mortality.
Introduction
Older adults represent the group with the highest TBI-related morbidity and mortality when compared to other groups (Dams-O’Connor, 2013), and rates of TBI in older adults are increasing, chiefly due to falls (e.g., CDC, 2019b). Compared to younger adults, those who are older have longer rehabilitation periods, show lower levels of improvement, and are less likely to return to their previous domicile post-TBI (Cuthbert et al., 2015). Although TBIs in older adults appear to be comparatively less severe (Cuthbert et al., 2015), explanations for worse rehabilitation outcomes are inconclusive. Theories as to why older adults seem to have increased vulnerability after TBI range from problems with the reliability of measurement instruments (Zuercher et al., 2009), especially with regard to use with older adults (Yap & Chua, 2008), to age-related physiological changes (Liu et al., 2017) or health conditions (Dams-O’Connor et al., 2016).
The ability of an individual consistently and autonomously to perform basic tasks necessary for living is termed functional independence (Curzel et al., 2013). Older age predicts lower functional independence after TBI (Sendroy-Terrill et al., 2010), despite comparatively lower injury severity levels (Marquez de la Plata et al., 2008). Individuals who are older when they sustain a TBI have lower functional independence at hospital discharge, at six months post injury, and at five years post TBI compared to younger adults (Marquez de la Plata et al., 2008; Mosenthal et al., 2004). Although discharge to specialized rehabilitation facilities is associated with better long-term functional independence, older adults are not directly admitted to specialized TBI rehabilitation as often as younger adults, even when injury severity is equivalent (Sveen et al., 2016).
Worldwide lifespans are increasing (WHO, 2019), resulting in a growing number and ratio of older adults to other age groups (Worldometer, 2020). For example, projections indicate that older people will make up nearly one-quarter of the U.S. population by 2060 (Statista, 2020), with the oldest old (ages 85 and over) projected to increase to approximately 19 million by that time (Vespa et al., 2020). With older age, risk for sustaining a TBI rises (CDC, 2019b), post-TBI morbidity and mortality rates are higher (Dams-O’Connor, 2013), and recovery outcomes are lower (Cuthbert et al., 2015). Understanding sociodemographic and injury-related risk factors in older adults with TBI with regard to long-term functional independence outcomes is an understudied area, and one which may provide increased awareness of contributors to recovery after TBI. As a result, the purpose of this study was to examine baseline sociodemographic and injury characteristics as predictors of functional independence trajectories in older adults with TBI across the 10 years after injury.
Method
Procedure
This study conducted secondary analyses of data collected as part of the TBI Model Systems (TBIMS) program, funded through the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) (NDSC, March 2020).
Participants
Criteria for inclusion in the TBIMS database are complicated mild or moderate-to-severe TBI, admission to a TBIMS emergency department within 72 hours of sustaining the TBI, age of at least 16 years at injury, acute care and inpatient rehabilitation in a TBIMS hospital, and informed consent by patient, family member, or guardian. Data from participants in the TBIMS national database who sustained a TBI at age 60 and older and had at least one Functional Independence Measure (FIM) Motor, FIM Cognitive, and Glasgow Outcome Scale-Extended (GOS-E) score at one follow-up time point (data were collected at 1 year, 2 years, 5 years, and 10 years post TBI) were included in the present study. In the current sample, 2,459 older adults met these inclusion criteria. Demographic and injury-related data are presented in Table 1.
Sample characteristics
Sample characteristics
Sociodemographic characteristics
Age was reported at the time of injury, and participants ranged from 60 years to more than 89 years (data were not collected on specific age past age 89 for confidentiality purposes, and those above age 89 were recoded as age 89). Sex was reported as male or female at the time of injury. Race/ethnicity was dichotomized as White and Asian/Pacific Islander or underrepresented minority (Black, Native American, Hispanic Origin, and Other). Level of education was noted in years from 0 to 19. Participants were considered partnered if they were married or cohabiting at the time of injury. Insurance was categorized as either private or other. Employment status was recorded for the month before injury, and participants were considered employed if they were competitively employed. Participants were divided into those with a history of substance use disorder and those without such a history. Participants’ physical and mental health pre-TBI was measured by endorsement of limitations to learning, dressing, working, going out of the house, or by a history of treatment for mental illness.
Injury severity
Injury severity was measured by length of PTA. Emergence from PTA is based on documented evidence provided in the acute care medical record or tracked prospectively through standardized measures upon admission to inpatient rehabilitation. If an individual was discharged from inpatient rehabilitation while still in PTA, for the purposes of this study their PTA score was coded as length of the combined hospital and inpatient rehabilitation stay (days) plus one, as is the convention in the TBIMS database.
Functional independence
Data analyses
All analyses were conducted using IBM SPSS Statistics version 27. As over the 10-year follow-up period many participants had missing data, Little’s missing completely at random (MCAR) test was performed on the data, and full information maximum likelihood (FIML) estimation was used to account for missing values, allowing retention of all participants meeting inclusion criteria. Dichotomous variables were given a reference point of 0, and continuous variables were centered around their means to reduce multicollinearity.
To examine trajectories of functional independence across the 10 years after TBI in older adults, several series of hierarchical linear models (HLMs) were run, one series for each of the three outcome variables. For each series, an unconditional growth model was run first with the successive additions of time2 and time3 to determine whether linear, quadratic, or cubic time models best depicted functional independence movement over time. -2 log likelihoods (-2LLs) were calculated and compared for each model, with a drop of 3.84 chi-squared points reflecting a statistically significant improvement over the previous model.
HLM was then used to examine baseline predictors of FIM Motor, FIM Cognitive, and GOS-E trajectories among older adults across 1, 2, 5, and 10 years after TBI. Predictors were entered simultaneously as fixed effects after being centered or given a reference point of 0, along with time (and with time2 or time3 as applicable). Each main HLM determined whether linear outcome trajectories across the four time points were predicted by baseline sociodemographic and injury severity characteristics of: time (coded as 0 [1 year], 1 [2 years], 4 [5 years], and 9 [10 years]); age; sex (coded as 0 = female, 1 = male); race/ethnicity (coded as 0 = White/Asian/Pacific Islander, 1 = underrepresented minority); education level; relationship status (coded as 0 = unpartnered, 1 = partnered); insurance type (coded as 0 = other, 1 = private); employment status at time of injury (coded as 0 = not employed, 1 = employed); history of substance use disorder (coded as 0 = no, 1 = yes); pre-TBI functional limitations in learning, dressing, working, or going out of the home (coded as 0 = no limitations, 1 = limitations); history of mental health treatment (coded as 0 = no, 1 = yes); and days in posttraumatic amnesia (PTA, with discharge while still in PTA being recoded as the number of days in TBI care +1). In order to test potential differential effects of the predictors over time (e.g., differences in slope as a function of the predictor), follow-up HLMs included each of the previously significant predictors from the first full model, time (and with time2 or time3 as applicable), and the interaction terms between time terms and the previously significant predictor. In order to avoid biasing figures by only graphing the outcome scores of participants with data present, the expectation maximization algorithm was used to impute missing values that then were used to calculate overall means to be presented in the figures. For parsimony, only statistically significant and meaningful interaction effects were graphed rather than main effects.
Results
Little’s MCAR tests
Given that all three Little’s MCAR tests were statistically significant (FIM Motor: χ2 (28) = 166.21, p < .001; FIM Cognitive: χ2 (28) = 150.81, p < .001; and GOS-E: χ2 (28) = 201.49, p < .001), reflecting differential attrition over time, FIML was used to account for missing data in the trajectory analyses. For degree of missingness of FIM Motor, FIM Cognitive, and GOS-E scores at follow-up time points, see Table 2.
Percentage of data present at each follow-up time point
Percentage of data present at each follow-up time point
The -2LL of the initial model with linear time was 43,787.53; the -2LL of the model with the addition of quadratic time was 43,787.53; and the -2LL of the model with the addition of cubic time was 43,787.23. Each successive addition of a time product term did not result in a -2LL decrease of more than 3.84 chi-square points from the previous models, which suggested that linear (straight line) movement of FIM Motor trajectories was the best fit for the data.
In the main HLM, FIM Motor scores decreased over time. The unstandardized b-weights and p-values for this HLM appear in Table 3. Lower FIM Motor trajectories were seen among participants who had been older at baseline; were members of an underrepresented racial/ethnic minority group; had lower educational attainment; had been unemployed at injury; had pre-TBI functional limitations in learning, dressing, or going out of the home; and had greater injury severity based on length of PTA.
Fixed effects
Fixed effects
Follow-up HLMs examined whether linear trajectories of FIM Motor could be predicted by the previously significant predictors and their interactions with time (Table 4). There were significant interactions for time*age, time*employment status at baseline, and time*pre-TBI learning limitations, suggesting differential change over time in motor functional independence as a function of these characteristics. The significant time*age interaction suggested that FIM Motor scores decreased over time for all older adults with TBI, but the decrease was steeper for those who had sustained their TBI at an older age (Fig. 1). The significant time*employment status interaction suggested that FIM Motor scores decreased over time for those who had been employed at the time of injury as well as for those who had been unemployed at the time of injury, with scores of those who had been employed decreasing at a slightly faster rate. However, the visual interaction effect when graphed was barely detectable so this interpretation may be unreliable and will not be interpreted further. The significant time*pre-injury learning limitations interaction suggested that FIM Motor scores decreased over time, with scores decreasing at a slightly faster rate for those who had had no pre-TBI learning limitations (Fig. 2).
Significant interactions in predictors over time
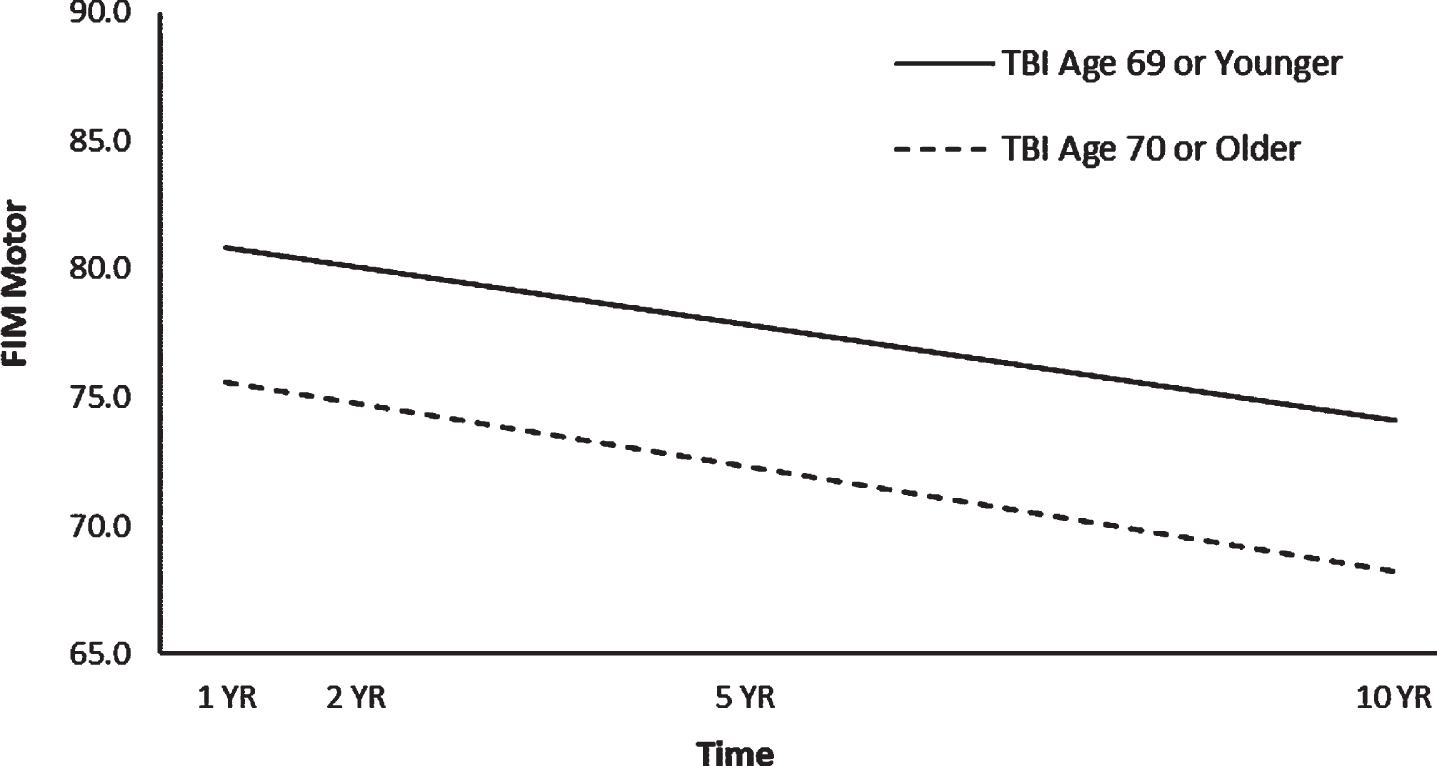
Interaction effect of age at injury and time on FIM motor trajectories.
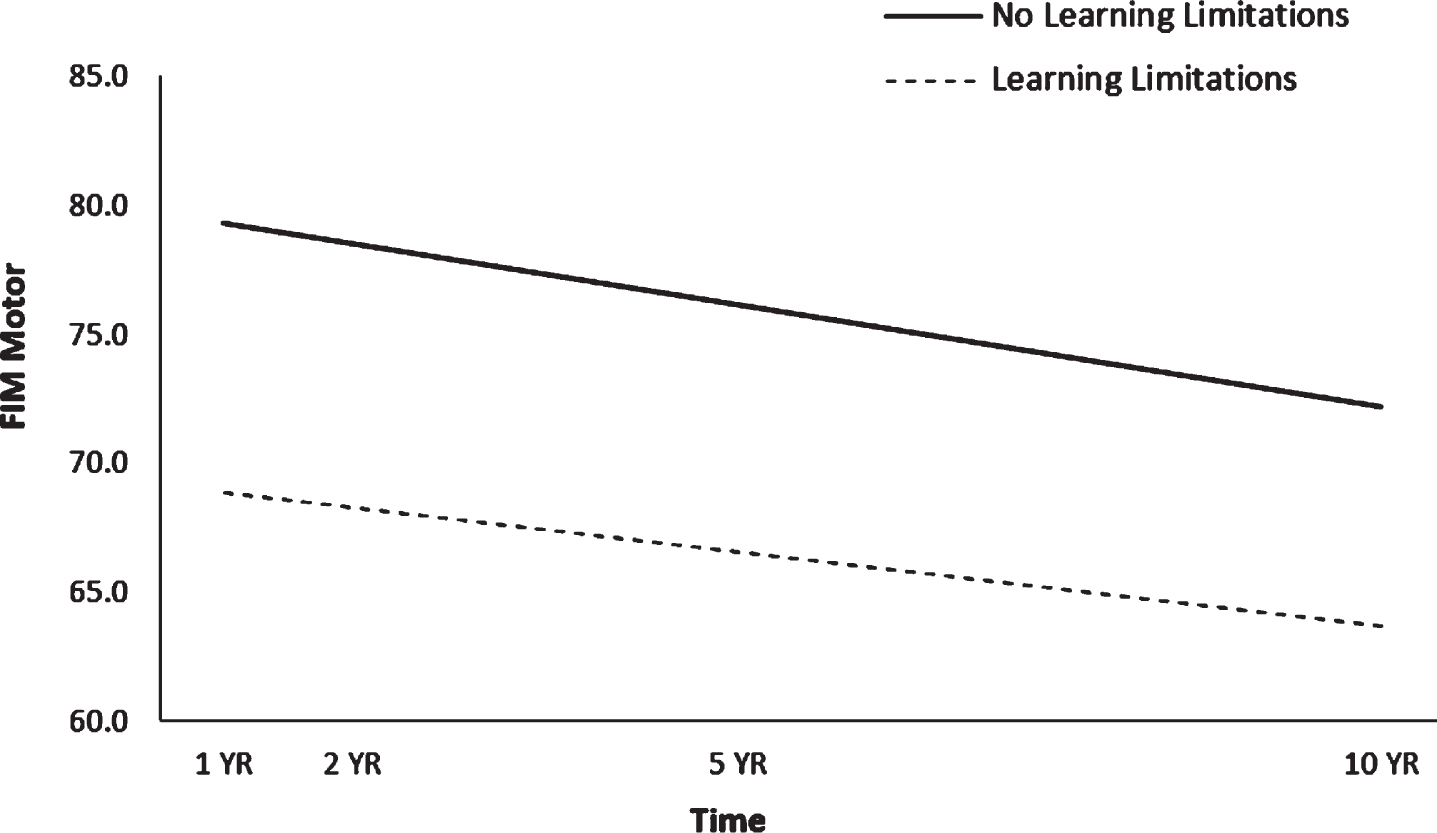
Interaction effect of pre-TBI learning limitations and time on FIM motor trajectories.
The -2LL of the initial model with linear time was 33,407.76; the -2LL of the model with the addition of quadratic time was 33,407.73; and the -2LL of the model with the addition of cubic time was 33,407.68. Each successive addition of a time product term did not result in a -2LL decrease of more than 3.84 chi-square points from the previous models, which suggested that linear (straight line) movement of FIM Cognitive trajectories was the best fit for the data.
In the main HLM, FIM Cognitive scores decreased over time. The unstandardized b-weights and p-values for this HLM appear in Table 3. Lower FIM Cognitive trajectories were seen among participants who had been older at baseline; were underrepresented minorities; had lower educational attainment; were unemployed at the time of injury; had pre-TBI functional limitations in learning or going out of the home; or had longer length of PTA.
Follow-up HLMs examined whether linear trajectories of FIM Cognitive could be predicted by the previously significant predictors and their interactions with time (Table 4). There were significant interactions for time*age, time*employment status at baseline, time*pre-TBI limitations in going out of the home, and time*PTA, suggesting a differential change over time in cognitive functional independence as a function of these characteristics. The significant time*age interaction suggested that FIM Cognitive scores decreased for all participants but decreased at a faster rate for those who had sustained their TBI at an older age (Fig. 3). The significant time*employment interaction suggested that FIM Cognitive scores decreased over time for those who had been employed at the time of injury and for those who had been unemployed at the time of injury but decreased at a faster rate for those who had been unemployed at the time of injury (Fig. 4). The significant time*pre-TBI limitations in going out of the home interaction suggested that FIM Cognitive scores decreased over time for all participants but at a slightly faster rate for those who had had no pre-injury limitations in going out of the home (Fig. 5). The significant time*injury severity interaction suggested that FIM Cognitive scores decreased over time for all participants but at a slightly faster rate for those who had less severe TBI (Fig. 6).
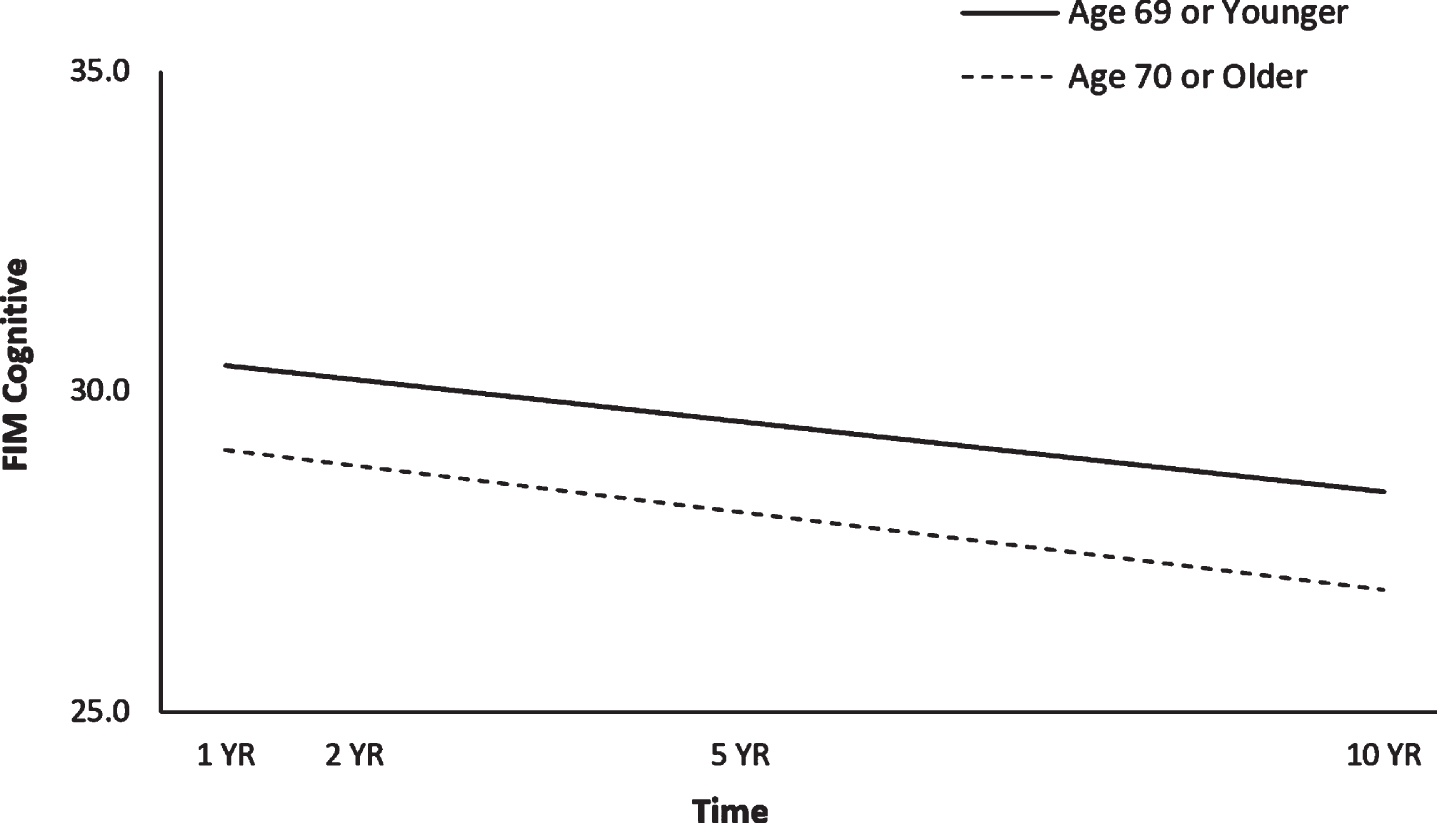
Interaction effect of age at injury and time on FIM cognitive trajectories.
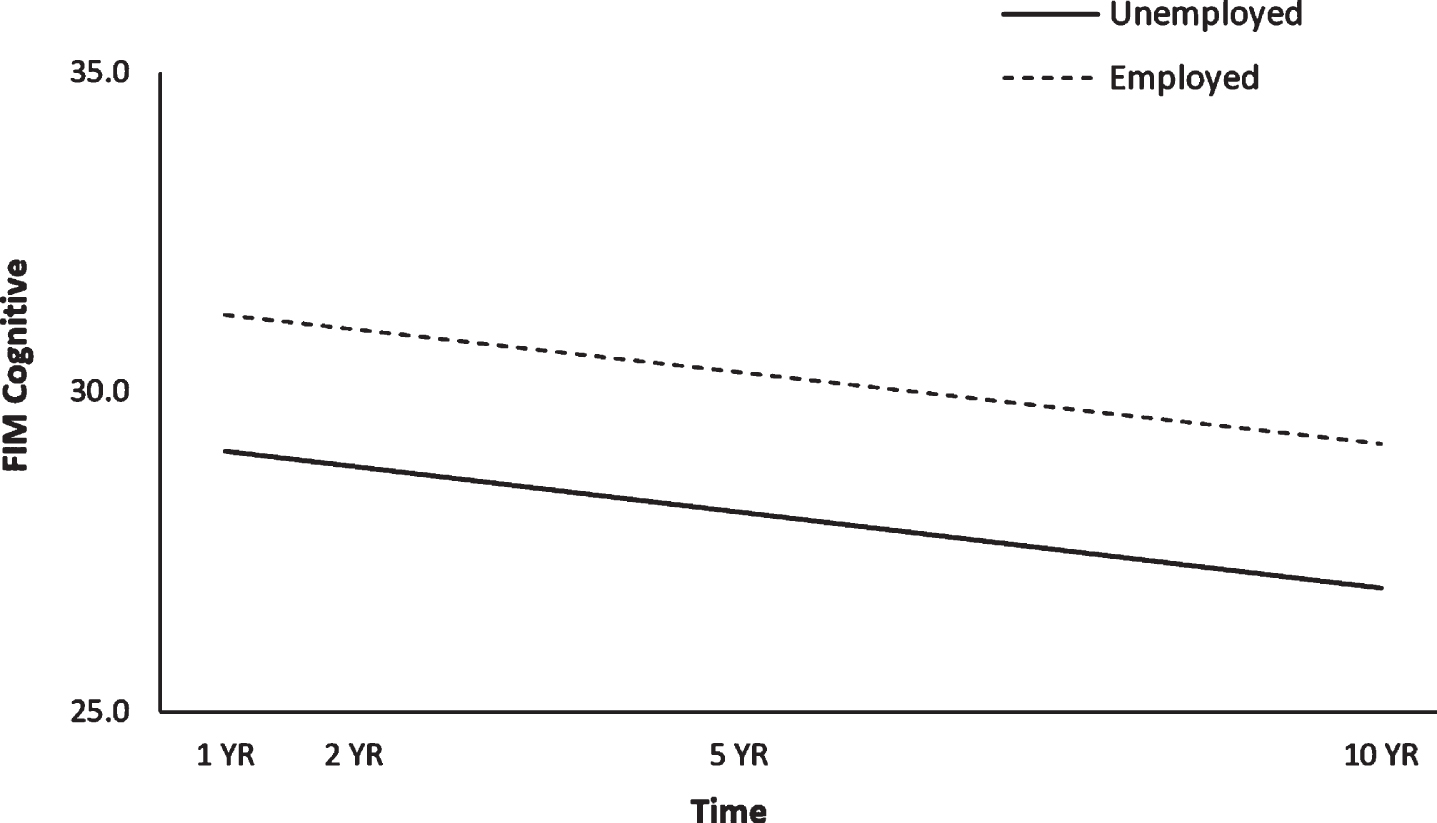
Interaction effect of pre-TBI employment and time on FIM cognitive trajectories.
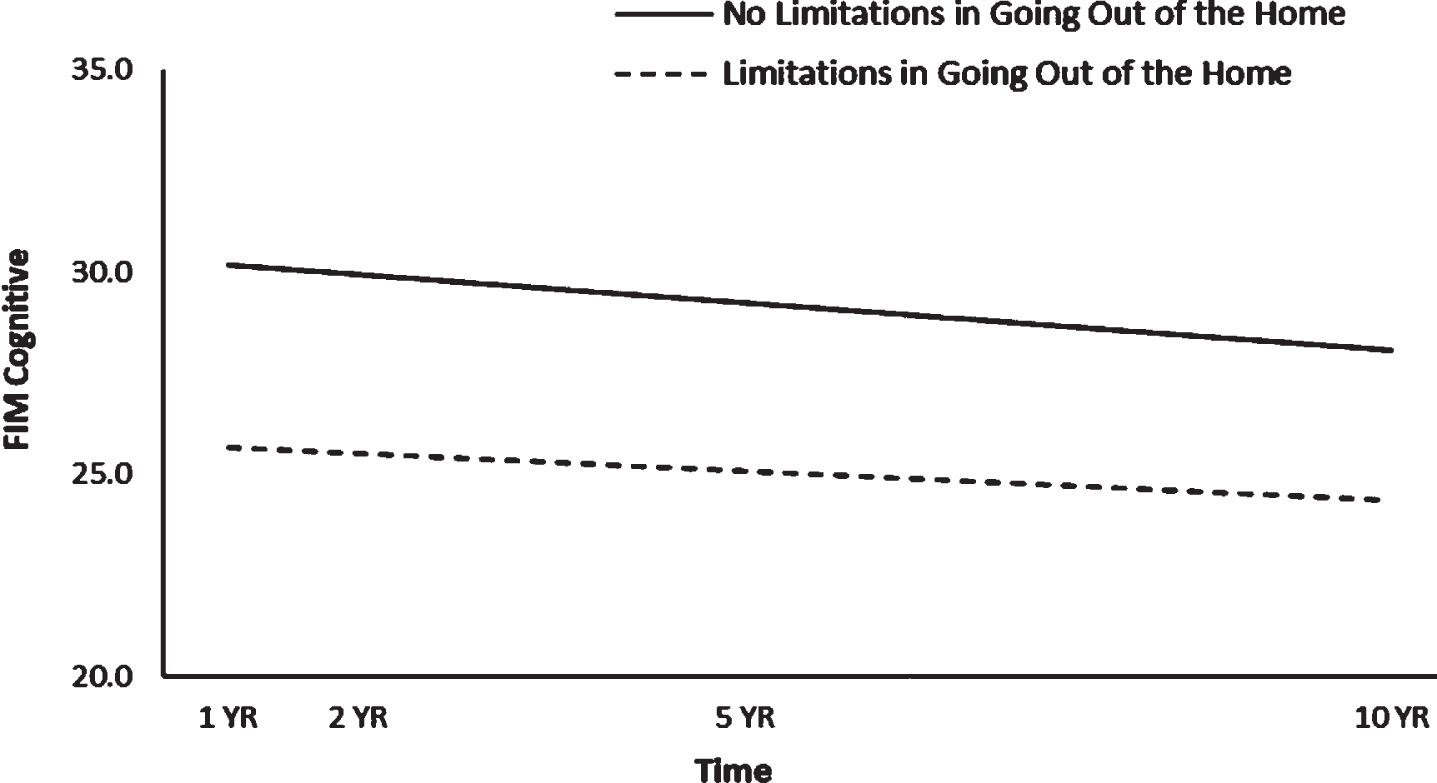
Interaction effect of pre-TBI limitations in going out of the home and time on FIM cognitive trajectories.

Interaction effect of days in PTA and time on FIM cognitive trajectories.
The -2LL of the initial model with linear time was 25,454.53; the -2LL of the model with the addition of quadratic time was 25,446.77; and the -2LL of the model with the addition of cubic time was 25,446.66. The addition of a time product term to the initial model resulted in a decrease of more than 3.84 chi-square points, but the addition of cubic time did not result in a decrease of more than 3.84 chi-square points, which suggested that quadratic movement of GOS-E trajectories was the best fit for the data.
In the main HLM, GOS-E scores decreased over time. The unstandardized b-weights and p-values for this HLM appear in Table 3. Lower GOS-E trajectories were seen among participants who had been older at baseline; were male; were underrepresented minorities; had lower educational attainment; did not have a history of substance use disorder; had pre-TBI functional limitations in learning, working, or going out of the home; and had longer PTA.
Follow-up HLMs examined whether quadratic trajectories of GOS-E scores could be predicted by the previously significant predictors and their interactions with time*time (Table 4). There were significant interactions for time*time*age, time*time*race/ethnicity, time*time*pre-TBI limitations in working, and time*time*pre-TBI limitations in going out of the home, suggesting a differential change over time in global outcomes as a function of these characteristics. The significant time*time*age interaction suggested that GOS-E scores decreased for younger participants at a steady rate over time but decreased faster for older participants across approximately the first three time points and then slowed the rate of decrease between the third and fourth time points (Fig. 7). The significant time*time*race/ethnicity interaction suggested that GOS-E scores decreased over time for all participants but at a faster rate for those who were not underrepresented minorities, with slower decreases for all participants between the third and fourth time points (Fig. 8). The significant time*time*pre-TBI limitations in working interaction suggested that GOS-E scores decreased over time for all participants, with the steepest and steadiest decrease in those with no pre-TBI working limitations and a faster rate of decrease in those with pre-TBI working limitations across the first three time points, with the rate of decrease leveling out at the fourth time point (Fig. 9). The significant time*time*pre-TBI limitations in going out of the home interaction suggested that GOS-E scores decreased at a steadier rate for those who had had no pre-TBI limitations in going out of the home, while scores for those who had had pre-TBI limitations in going out of the home decreased faster between the first three time points and then slowed until the decrease evened out (no more decrease) as it approached Year 10 (Fig. 10).

Interaction effect of age and time on GOS-E trajectories.
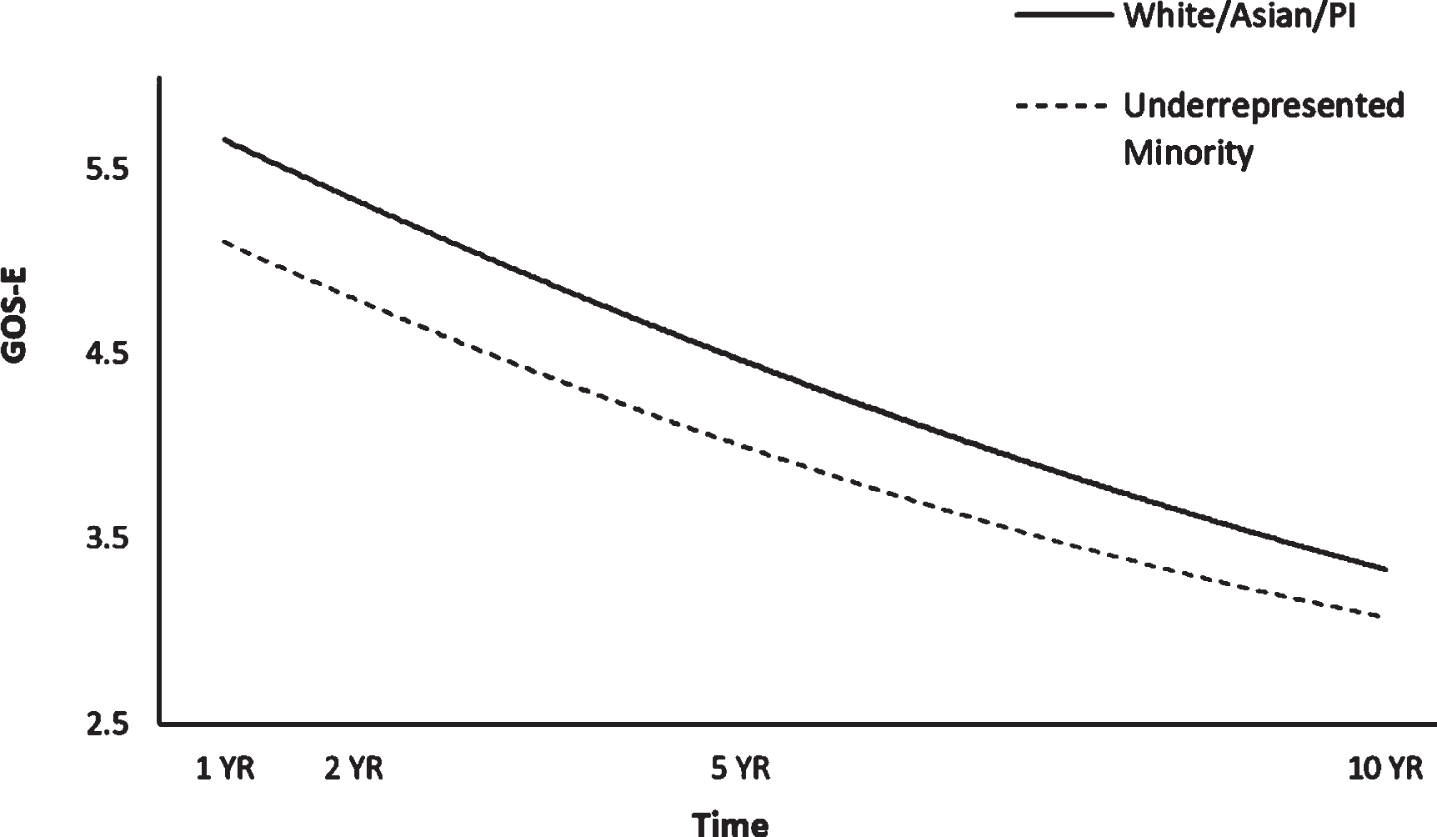
Interaction effect of race/ethnicity and time on GOS-E trajectories.

Interaction effect of pre-TBI working limitations and time on GOS-E trajectories.

Interaction effect of pre-TBI limitations in going out of the home and time on GOS-E trajectories.
This study examined the roles of sociodemographic and injury characteristics as predictors of functional independence trajectories across the first 10 years after TBI in adults who experienced TBI at age 60 or older. Functional independence scores decreased steadily over time across the overall sample. Scores on FIM Motor, FIM Cognitive, and GOS-E had steeper declines for those who had sustained their TBI at an older age, with GOS-E score rate decreases slowing between years 5 and 10 post-TBI. Previous research in the general population with TBI has found that FIM scores improve from time of injury to 3 months and GOS-E scores show improvement up until 12 months (Sandhaug et al., 2015), but that greater time post injury predicts decreased physical and cognitive functioning (Sendroy-Terrill et al., 2010), more in line with the current findings and perhaps particularly so as the current study’s older adults may have had accentuated functional declines based on advancing age. The limited work with older adults has found that although recovery is significantly slower for older adults than for younger adults with TBI (Frankel et al., 2006), there is general improvement in FIM motor and cognitive scores in the acute rehabilitation period (Hammond et al., 2019). In the current study, it is likely that rehabilitation gains occurred during the first year, but the data were not granular enough to identify the uptick in functioning.
Although functional independence in both FIM Motor and FIM Cognitive scores declined for all participants, independence declined at a faster pace for those who had sustained their TBI at an older age. Likewise, GOS-E scores also decreased over time for both younger and older groups, but the decline in functional independence was faster for the older group for approximately the first 5 years after TBI with a slower rate of decrease from years 5 to 10. These results are similar to previous research in the general population with TBI which has found that greater age at injury predicts lower functional independence trajectories (Forslund et al., 2017) and declines in functional independence (Sendroy-Terrill et al., 2010) and with older adult studies showing increased age associated with lower odds of living independently (Utomo et al., 2009) and less functional improvement with age (Hammond et al., 2019).
There are several possible explanations for the finding of overall lower trajectories of functional independence in older adults as well as declines over time. One possibility is related to increased physical disability associated with aging independent of sequelae brought about by TBI. Disability rates increase as age increases (BLS, 2019), and most older adults have at least one chronic condition (He et al., 2018), so lower function with increased age could be reflective of increasing co-occurring age-related illnesses and disabilities. Another possible reason for lower and decreasing functional independence with greater age is decreased social participation. Social involvement after TBI may be constrained because of primary effects such as impaired motivation or ability to be with other people or changes in behavioral regulation and cognition (Tate & Broe, 1999). In the course of development, older adults already tend to condense the size of their social networks as they age (English & Carstensen, 2014), and while this may be adaptive for promoting emotional wellbeing prior to TBI, it is possible that the additional narrowing of the social network brought about by TBI may severely restrict availability of resources after TBI.
Members of underrepresented minority groups had lower functional independence trajectories across all three measures. This is consistent with literature which documents that underrepresented racial/ethnic minorities have worse functional outcomes over time than do Whites (Arango-Lasprilla et al., 2007a). This may be a result of not having equal access to care, whether through barriers such as language difficulties, uninsured or underinsured status (Shafi et al., 2007), mistrust of the medical community (Boulware et al., 2003), or receiving less inpatient therapy and fewer referrals to rehabilitation services (Asemota et al., 2013; Burnett et al., 2003). Minorities also have less steady competitive employment after TBI than racial/ethnic majority members (Gary et al., 2009). While underrepresented racial/ethnic minorities did have lower functional independence trajectories, only GOS-E scores showed a significant interaction with time, with functional independence decreasing over time at a faster rate for those who were not underrepresented minorities (Fig. 8). The rate of decline slowed for all participants between 5 and 10 years. This interaction with time may well be a demonstration of the regression toward the mean phenomenon.
Educational attainment levels showed main effects on functional independence across all three outcome measures, with individuals of lower educational attainment having lower functional independence trajectories. This is consistent with literature which has found that higher education levels are associated with better physical and cognitive functioning (e.g., Schonberger et al., 2011). It is still somewhat unclear why higher education should be associated with better functional outcomes, especially with some studies finding that education level itself does not predict global outcome trajectories (Forslund et al., 2019) after TBI. Proposed theories for the education–improved outcomes association include development of better cognitive reserve and compensatory ability (Giovacchini et al., 2019), as well as healthier lifestyles and access to healthcare (Fletcher & Frisvold, 2009).
Individuals who had been unemployed at injury had lower FIM Motor and FIM Cognitive trajectories. This finding is consistent with other studies which have found that employment at injury predicts employment after TBI (Gary et al., 2009) and lower disability (Willemse-van Son et al., 2007). Further, FIM Cognitive scores decreased at a slightly faster pace for those who had been unemployed at the time of injury. The FIM Cognitive finding is consistent with previous literature which found that being employed at time of injury predicts higher functional trajectories over time (Forslund et al., 2017) and that cognitive function is higher for older adults who stay in the workforce compared to those who remain retired (Lee et al., 2019).
Individuals with pre-TBI health limitations in learning and going out of the home had lower functional independence trajectories across all three outcome measures. Those with pre-injury limitations in dressing had lower FIM motor trajectories, and those with limitations in working had lower GOS-E trajectories. Pre-TBI limitations to performance of ADLs such as dressing may be indicative of overall poorer pre-TBI functioning, and it is therefore not unexpected to see this trend continue after TBI. Pre-TBI learning limitations showed a significant effect over time only for FIM Motor scores (Fig. 2), as those who had had no pre-injury learning limitations showed a slightly faster rate of decline over 10 years than those who had pre-injury learning limitations. The slightly steeper rate of decline may be more representative of the decline in motor functioning which would typically be associated with aging, as individuals who had had pre-TBI learning limitations showed 1 year follow-up scores which were lower than the 10-year scores of those who had had no pre-injury limitations in learning. FIM Cognitive scores for those with pre-TBI limitations in going out of the home decreased at a slightly slower rate than for those with no such limitations (Fig. 5), but GOS-E scores for those with limitations in going out of the home prior to their TBI decreased faster across the first three time points, with the rate of decrease slowing between years 5 and 10 until the decrease leveled out as it approached year 10 (Fig. 10). It may be that as GOS-E includes both motor and cognitive indices, the FIM Cognitive scale was picking up the most prevalent area of decline, possibly more noticeable for those with fewer limitations on going out of the home at injury. GOS-E trajectories decreased more quickly across the first 5 years for those with pre-TBI working limitations, with the rate of decrease leveling out at 10 years post-TBI (Fig. 9). Similar to findings related to employment at injury, these findings may be reflective of higher functional trajectories over time (Forslund et al., 2017) for those who had been employed at injury.
Individuals who had greater injury severity had lower functional independence across all three outcome trajectories. This is consistent with studies showing longer time in PTA predicts reduced global outcomes over time (Forslund et al., 2019). Additionally, FIM Cognitive scores decreased over time at a slightly faster rate for those with less severe TBI (Fig. 6). This may be associated with more noticeable age-related declines over time when TBI-related debilities are not subsuming age-related declines.
Clinical implications for older adults with TBI
The growing number and proportion of older adults makes it likely that clinicians will see more cases of TBI in this population, especially for those aged 80 years and older (CDC, 2019b). As morbidity and mortality rates are highest for older adults compared to other age groups (Dams-O’Connor, 2013), awareness of risk factors for reduced post-TBI outcomes in this group is the first critical step for treatment planning. In older adults with TBI, it is important for health care professionals to note increased risk for comparatively poorer outcomes associated with increased age, underrepresented minority status, lower educational attainment, being unemployed at injury, pre-TBI health comorbidities, and greater number of days in PTA. Knowing that older adults face higher morbidity and mortality after TBI, identification of the above risk factors should be a priority at intake, with subsequent implementation of treatment regimens specific to older adults. For example, physical and psychological interventions should take into consideration pre-TBI limitations (e.g., health comorbidities, decreased social networks) and the possibility that formal rehabilitation programs may need to be intensified, broader in scope, and longer in duration than is typical when basing treatment plans on standards established for younger people with TBI.
As some sociodemographic risk factors do not lend themselves to being addressed post-TBI (e.g., age, employment status at time of injury, and educational attainment), more efforts should be geared toward educating older adults about the increased risks associated with incurring TBI in older adulthood. Concerted educational endeavors on ways to offset these risk factors such as maintaining social engagement, reducing fall risks, adopting lifestyle habits that support better physical and mental health, and engaging in meaningful work may help older adults to exert control over mitigation of some of the risk factors associated with reduced outcomes after TBI.
Limitations and future directions
The current study has several limitations which should be considered when interpreting its findings, and as a result, directions for future research. When conducting a longitudinal study over 10 years and limiting the sample to adults aged 60 and older with complex medical histories, it is understandable that there would be a number of participants who would be lost to follow-up due to illness or death. Participants who are underrepresented minorities, have lower socioeconomic status, a history of substance use, or injury caused by violence are those who are most often lost to follow-up in the 2 years post TBI (Corrigan et al., 2003). In order to retain sufficient data for analysis at the 5- and 10-year time points and not limit participant inclusion to those with complete data (and therefore healthier participants), advanced statistical methods (FIML and expectation maximization) were used to account for or estimate missing values. As attrition was fairly high at follow-up years 5 and 10, it is likely that analyses included data which was estimated for individuals who were deceased at one or more time points, especially since missingness reached approximately 87% for FIM scores at year 10. Therefore, point estimates further out should be interpreted withcaution.
Although the TBIMS database contains a wide array of variables, there were limitations to the information available at the time of this study. For example, Form I (baseline) of the TBIMS database had no comprehensive index of either cognition or mental health, and participating TBIMS sites only recently started adding data regarding many of the pre-existing health conditions common in older adults such as congestive heart failure, diabetes, and disordered sleep. As these may be important considerations when examining functional outcomes after TBI in older adults, pre-injury functional limitations to learning, dressing, going out of the home, and working, and substance use history and treatment for mental health conditions were used as proxies for pre-injury physical and mental health status. When sufficient data on comorbidities common in older adults, formal indices of mental health and cognition, and health contributors such as sleep patterns at the time of injury become more available, functional outcomes in older adults with TBI should be reexamined to confirm our findings with consideration of those variables.
Conclusion
Many studies have shown that older adults with TBI have reduced rehabilitation outcomes compared to younger people, and the current study showed that this trend holds true throughout the older adult lifespan, with increasing age being a significant predictor of reduced long-term outcome trajectories. Moreover, in addition to increased age, this study identified several other risk factors for reduced functional independence in older adults with TBI, specifically: male; underrepresented racial/ethnic minority; lower educational attainment; unemployed at time of injury; no history of substance use; difficulties with learning, dressing, and going out of the home prior to the TBI; and longer time in PTA. FIM Motor, FIM Cognitive, and GOS-E trajectories were significantly predicted by interactions between time terms and a number of other demographic and injury-severity variables. The significant predictors of long-term functional independence trajectories in older adults with TBI identified in this study may serve individuals with TBI and care providers by heightening awareness of the need for attention to these factors in treatment planning and long-term health monitoring and ultimately as a way to decrease morbidity and mortality in this older adult population.
Conflict of interest
None to report.
Disclaimer
The Traumatic Brain Injury (TBI) Model Systems National Database is a multicenter study of the TBI Model Systems Centers Program, and is supported by the National Institute on Disability, Independent Living and Rehabilitation Research (NIDILRR) a center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). However, the content of this article does not necessarily reflect the opinions or views of the TBI Model Systems Centers, NIDILRR, ACL or HHS.