
Abstract
BACKGROUND:
High collision rates and frequency of entering the opening from non-paretic sides are associated with collision in individuals with stroke.
OBJECTIVE:
To identify factors associated with collision avoidance behavior when individuals with stroke walked through narrow openings.
METHODS:
Participants with subacute or chronic stroke walked through a narrow opening and had to avoid colliding with obstacles. Multiple regression analyses were conducted with pathophysiology, motor function, and judgment ability as predictor variables; collision rate and frequency of entering the opening from non-paretic sides were outcome variables.
RESULTS:
Sixty-one eligible individuals with stroke aged 63±12 years were enrolled. Thirty participants collided twice or more and 37 entered the opening from the non-paretic side. Higher collision occurrence was associated with slower Timed Up and Go tests and left-right sway (odds ratios, 1.2 and 5.6; 95% confidence intervals, 1.1–1.3 and 1.3–28.2; p = .008 and.025, respectively). Entering from non-paretic sides was associated with lesions in the thalamus, left-sided hemiplegia, and Brunnstrom stage 3 or lower (odds ratios, 6.6, 8.7, and 6.7; 95% confidence intervals, 1.3–52.5, 2.5–36.5, and 1.2–57.5; and p = .038,.001, and.048, respectively).
CONCLUSION:
Walking ability is associated with avoiding obstacle collision, while pathophysiological characteristics and degree of paralysis are associated with a preference for which side of the body enters an opening first. Interventions to improve walking ability may improve collision avoidance. Avoidance behavior during intervention varies depending on the lesion position.
Introduction
Approximately half of the patients with stroke (37–51%) experience falls within 6 months of onset (Kerse et al., 2008; Yates et al., 2002). A common cause of falls in such individuals is turning while walking (Hyndman et al., 2002; Simpson et al., 2011; Harris et al., 2005). Falls in individuals with stroke, who can accurately tell the information of the past fall (i.e., there is no prominent dementia or higher brain dysfunction), are related to motor factors (such as imbalance and impaired walking ability) or cognitive factors (such as misjudgment, and attention disorder) (Hyndman et al., 2002; Simpson et al., 2011), which are a major problem in daily life. A decline in the ability to judge the morphology and positional relationship of an obstacle (i.e., cognitive factors) and/or a decline in the ability to alter walking style according to the obstacle (i.e., motor factors) may be related to the falls when individuals with stroke try to avoid an obstacle while walking. Regarding motor factors, a previous study reported that individuals with stroke who failed the obstacle-crossing task had slow walking speed and a high risk of falling after 6 months compared with individuals who succeeded at the task (Said et al., 2013). Another previous study reported that it is difficult for stroke patients with poor lower limb function and slow walking speed to adjust the instantaneous gait pattern while stepping over an obstacle (Den Otter et al., 2005). Thus, inappropriate gait adaptability in obstacle avoidance is associated with lower extremity function and gait ability, leading to falls. These previous studies target individuals with stroke who have no cognitive problems, but the relationship between judgment ability and obstacle avoidance behavior is unknown. Therefore, we need to correctly assess the motor and cognitive factors associated with falls and fall-related behaviors in stroke individuals without dementia or higher brain dysfunction.
The task of walking through a narrow opening has often been used in previous studies and may be useful for assessing both motor and cognitive factors during collision avoidance behavior (Cowie et al., 2010; Higuchi et al., 2009; Hackney and Cinelli, 2013). This walking-through-an-opening task has been adapted for use in individuals with stroke in previous studies and has produced two main findings (Muroi, Hiroi, et al., 2017; Muroi, Saito, Koyake, Higo, et al., 2022). First, individuals with stroke who had a history of falls had more collisions with obstacles on the paretic side. Second, collision rates were reduced when individuals initially entered an opening from the paretic side of their body. These findings suggest that entering from the paretic side may be a desirable action to prevent collisions among individuals with stroke who experienced falls. Investigating the motor and cognitive (including the pathophysiological) characteristics of individuals with stroke who collide with obstacles and naturally enter from the paretic side is important to examine the factors associated with successful obstacle avoidance.
The factors of collision, from both the motor and cognitive aspects, were investigated when individuals with stroke walked through an opening. Muroi, Saito, Koyake, Higo, et al. (2022) considered the effect of insufficient rotation of the body as a motor factor but was not able to demonstrate this. Additionally, in terms of cognitive factors, there were no significant differences between individuals with stroke and age-matched controls in the perceptual judgment task in the static standing position (Muroi, Hiroi, et al., 2017); however, there were many unexpected collisions in individuals with stroke (Muroi, Saito, Koyake, Higo, et al., 2022). In a single case study of a patient who presented with unilateral spatial neglect, the collision rate on the paretic side was reduced by practicing passing through the opening from the paretic side for 3 weeks, although the neglected symptom itself did not change (Muroi, Saito, Koyake, Yasuda, et al., 2022). This result showed that there was a gap between perceptual cognition and motor improvement. Thus, there is no consistent view of the factors related to collisions with obstacles. A study that observed spontaneous collision avoidance behavior noticed a large individual difference in whether to enter from the paretic or non-paretic side (Muroi, Hiroi et al., 2017). Entering from the non-paretic side can be difficult to recognize for individuals with stroke due to the posterior position of the paretic body. Some individuals with stroke did not change the direction of entry even though they frequently collided with the paretic side of the body. The reason for not changing their behavior was unclear.
A systematic review showed that motor dysfunction, imbalance, cognitive decline, and fall history were related to the factors that cause individuals with stroke to fall as behavioral errors and that they are strongly related to fall (Xu et al., 2018). Additionally, a preference of body side (i.e., paretic or non-paretic) in situations where compensatory stepping is required to avoid falls has been investigated (Mansfield et al., 2012). We hypothesized that motor and cognitive functions and fall history are factors that determine the behavioral error of individuals with stroke. This study aimed to clarify the following two characteristics of individuals with stroke while performing the walking-through-an-opening task (Harris et al., 2005): factors of collision and factors that make it difficult to enter from the paretic side. Identifying factors associated with collision or collision-related behavior may help guide rehabilitation therapists to develop interventions to improve collision avoidance behavior.
Materials and methods
Participants
Patients were recruited from two rehabilitation hospitals in Japan. All the participants provided written informed consent. This study was conducted in accordance with the Declaration of Helsinki and approved by the local ethics committee.
The participants were patients in or discharged from a subacute hospital (more than 1 month after stroke onset). The inclusion criteria were unilateral stroke and ability to independently walk for more than 100 m with or without an assistive device. The exclusion criteria were as follows: (a) neurological, orthopedic, or other disorders that could affect walking; (b) a history of visual deficits; (c) visual field deficits and visual spatial neglect; or (d) a score of less than 24 on the Mini-Mental State Examination (MMSE) (Holsinger et al., 2007). The following four assessments were conducted in the order of assessment of patient characteristics, perceptual judgment test, assessment of walking-through-an-opening test, and measurement of relative minimum passable width.
Assessment of patient characteristics
Participant characteristics and pathophysiological documentation of individuals with stroke were obtained from their medical records. All participants with stroke were asked whether they had fallen during the past 12 months. A fall was defined as an event that resulted in a person coming to rest unintentionally on the ground or another lower level (Clark et al., 1993). Participants’ cognitive function was assessed using the MMSE (Holsinger et al., 2007). Functional mobility was assessed using the Timed Up and Go (TUG) test (Podsiadlo and Richardson, 1991): participants were instructed to stand up from a standard chair, walk a distance of 3 m at maximum speed, turn, walk back to the chair, and sit down. To describe the impairment in stroke participants, the upper and lower extremity Brunnstrom recovery stages (BRS) (Brunnstrom, 1966), which assess the degree of recovery and muscle tone of upper and lower extremity mobility, were determined. Muscle tone of the upper and lower limbs was classified into 5 categories (normal, increased mildly, increased moderately, decreased, and increased) by assessing the passive resistance of the elbow and knee joint flexion and extension using the Stroke Impairment Assessment Set (SIAS) criteria (Tsuji et al., 2000; Liu et al., 2002). These measurements were performed in a random order.
Perceptual judgment test
Participants stood 4 m in front of an opening. They observed openings of various widths and reported whether they believed they would be able to walk through the opening without colliding. A series of opening widths was presented in either an ascending or descending order with 2-cm intervals (staircase method). The presentation of the series was terminated when the participants alternated their response (i.e., from passable to impassable, or from impassable to passable) six times. The perceived minimum passable width was averaged from 6 times response, and each ascending and descending order was averaged. Perceptual judgment passability is the perceived minimum passable width relative to the minimum passable width. We interpreted that if the relative value was close to 1.0 times their shoulder width, the participants’ judgment was correct; however, if it was less than 1.0, they underestimated the space (Cowie et al., 2010; Muroi, Hiroi, et al., 2017).
Assessment of walking-through-an-opening test
Participants were instructed to walk through an opening without colliding with a screen (Fig. 1a). Four different opening widths were used: 0.9-, 1.0-, 1.1-, and 1.2- times the width of the participants’ shoulders. The opening widths were randomly selected. To ensure the participants’ safety, two therapists stood behind the door opening while the participants performed the task. The participants were required to start walking and were permitted to rotate their bodies when necessary to avoid collisions. Each participant performed a total of 12 trials (three trials for each of the four opening widths). Three therapists observed the participants’ spontaneous body rotation and determined the collision with the opening and which body side entered first.
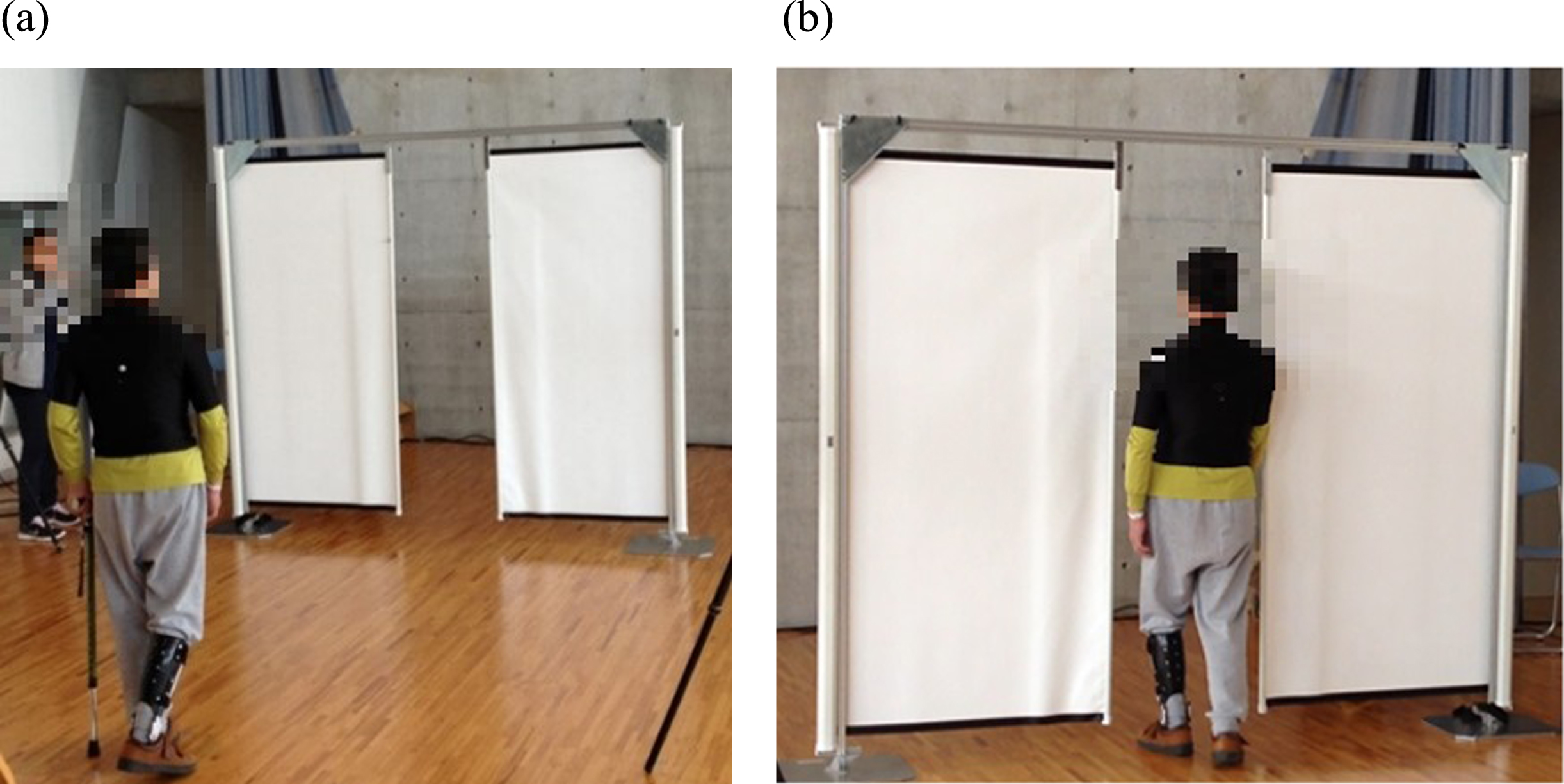
(a) The walking-through-an-opening test. Participants were permitted to rotate their bodies when necessary to avoid collisions. (b) Assessment of relative minimum passable width. Participants walked through the opening without body rotation.
At the end of the assessment, participants’ minimum passable widths were measured (Fig. 1b). The minimum passable width was defined as the minimum width that a participant could walk through the opening twice consecutively, without body rotation. The relative minimum passable width is the ratio between the minimum passable width and the participant’s shoulder width. A large relative value indicates that the left-right (frontal plane) sway during the task is large, because they collide with the door due to left-right sway while walking.
Statistical analysis
We described the characteristics for all participants and two outcomes during the walking-through-an-opening test: (1) the number of collisions and (2) the direction of entry. The number of collisions was categorized as “high” if there were two or more collisions, or “low” if less than two. We classified the direction of entering when a subject walked through the opening as the “paretic” or “non-paretic” side. We calculated the mean±standard deviation (SD) for continuous variables.
Multiple regression analyses were conducted with pathophysiology, motor function, and judgment ability as predictor variables, and number of collisions and the frequency of entering the opening from the non-paretic side as outcome variables. Logistic regression analysis for each outcome was conducted using the factors selected based on the hypothesis. At first, we estimated the association of number of collisions with relative minimum passable widths and the TUG test. In the model, by adding variables of (i) upper and lower limb muscle tone, (ii) falls in the past year, and (iii) perceptual judgment passability, we verified changes in the association. The relative minimum passable width to the shoulder width was separated at a cut-off of 1.1. The muscle tone in the upper or lower limb, measured using the SIAS, was grouped as normal and others (Brunnstrom, 1966; Tsuji et al., 2000): 3 corresponds to normal, and 2 or less corresponds to increased or decreased. Perceptual judgment passability was separated using a cut-off of 1.0. We also estimated the association of the direction of entry with pathophysiology factors: (i) lesion on thalamus, (ii) hemiplegic side, and (iii) motor factor Brunnstrom stage. Then we added a variable of perceptual judgment passability to the model. The Brunnstrom stage was cut-off at stage 3. All analyses were performed using R software, version 4.0.5, and a p-value<0.05 was considered statistically significant.
Results
Sixty-one individuals with stroke (including 28 women) with a mean age of 62.9 years (SD = 11.6) were included in the study. The mean time from stroke onset to testing was 7.7 months (range, 1–67). During the walking-through-an-opening test, the median collision number was 1 (interquartile range: 1–3, minimum: 0, maximum: 8), 30 participants (49%) collided two or more times, and 37 participants (61%) entered the opening from the non-paretic side. Table 1 shows the participant characteristics.
Participant characteristics
Participant characteristics
Notes: Muscle tone was assessed using Stroke Impairment Assessment Set: 3 corresponds to normal, 2 corresponds to increased mildly, 1A and 0 correspond to increased, and 1B corresponds to decreased.
In the logistic regression models, more than 1.1 of relative minimum passable width and slower speed on the TUG tests were associated with an increased number of collisions (Table 2). Models on the non-paretic side entering indicated an association with lesions in the thalamus, left-sided hemiplegia, and Brunnstrom stage 3 or lower (Table 3).
Logistic regression models on increased number of collisions
Abbreviations: OR, odds ratio; CI, confidence interval.
Logistic regression models on entering from the non-paretic side
Abbreviations: OR, odds ratio; CI, confidence interval.
We investigated the factors affecting two characteristic behaviors of individuals with stroke who had no dementia or higher brain dysfunction in obstacle avoidance situations and used multiple regression analysis to determine any associations. First, our results suggest that individuals with stroke who have large left-right sway during walking and slow TUG time, including turn movements, are at high risk of collisions in narrow opening passages. Second, non-paretic entry was associated with a lesion in the thalamus, left paralysis (i.e., right hemisphere injury), and Brunnstrom stage 3 or lower (i.e., remaining motor paralysis with abnormal muscle tone).
Factors resulting in collisions during obstacle avoidance tasks
We first investigated walking ability (i.e., minimum passable width and TUG), and then factors that widen the sway (i.e., action space) to the left and right (i.e., muscle tone, fall history, and perceptual judgment). We found that in individuals with stroke, the collisions with an obstacle were related to the minimum passage and TUG speed. However, past fall history did not significantly associate with an increase in the number of collisions and remained a trend (Table 2). In this study, the minimum passable width of the opening was measured as an index of the action space, including sway during walking. When the width of the opening was larger than 1.1 times the shoulder width (cf., for a 40-cm shoulder width, the left and right space margins must be 2 cm or more each), there were many collisions. Gait in individuals with stroke has a large lateral displacement in both the stance and swing phases, particularly in the stance phase (do Carmo et al., 2015; Kao et al., 2014). This is because of weakness of the gluteus medius muscle and desensitization of the lower limbs on the paretic side (Dean and Kautz, 2015). Thus, individuals with stroke need a wider action space than healthy individuals for obstacles at the frontal plane. However, hypertonia of the upper and lower limbs did not directly affect the collision because even if it is difficult to control muscle tone voluntarily, it is possible to avoid obstacles if such individuals have good recognition of their physical condition. Therefore, it is highly possible that the left-right sway was connected to the collisions; individuals not fully aware of their own sway during walking could not measure and time their rotation in the walking-through-an-opening task.
The ability to judge passability was measured as a cognitive aspect (whether one’s own physical ability could be recognized), but it was not a factor in collisions. The reason may be that judgment ability in a static standing position and judgment ability in a dynamic scene, such as walking, may differ. Hackney and Cinelli (2013) reported that static perception was not much different between the elderly and the young, but dynamic perception showed that the elderly had a large margin in consideration of their left-right sway. Considering the findings of Muroi, Saito, Koyake, Higo et al. (2022), who reported unexpected collisions in individuals with stroke, dynamic perception may be reduced. Thus, thinking about how to avoid obstacles while walking becomes a dual task, which may have made decision making more difficult for individuals with stroke leading to reduced walking automaticity. Another possibility as to why cognitive factors were not affected is that most participants had lesions of the thalamus, putamen, and crown of radiation, with no impairment of the dorsal pathways (see Supplemental material). It has been proposed that the dorsal visual pathway is important for actions related to visual objects (such as obstacle) based on coordinate information obtained by spatial visual perception (Milner and Goodale, 1995). Cognitive factors may not have contributed to the conflict because most of the participants in this study had this pathway intact. Our findings indicate that it may be necessary to improve walking ability in individuals with stroke to avoid collisions with obstacles. This would include standing and turning movements (such as those in the TUG test) and acquiring a walking pattern with minimal sway on the frontal plane.
Factors that make it difficult to enter from the paretic side
Previous studies have shown that entering an opening from the paretic side was useful for reducing the collision rate (Muroi, Hiroi, et al., 2017; Muroi, Saito, Koyake, Higo, et al., 2022). In this study, we examined factors for the lesion (site and left or right), the function of the lower limbs on the paretic side, and the influence of perceptual judgment on passability. Three factors were found to be associated with the conditions that inhibited entering from the paretic side (conditions for entering from the non-paretic side): right hemisphere injury (left motor paralysis), thalamic lesions, and lower limb BRS stage 3.
First, right hemisphere injury that causes “Rightward Orienting Bias” may lead to entering from the non-paretic (right) side while walking-through-an-opening, even in the absence of manifested higher brain dysfunction. The right hemisphere is involved in attention, body image, and spatial cognition, and disorders of the right hemisphere are prone to falls as action errors (Rapport et al., 1993; Wada et al., 2007). Action errors are reported to occur on the left side, particularly in obstacle avoidance situations, and their detection is more sensitive than the assessment of unilateral spatial neglect (USN) on paper (Webster et al., 1989). This phenomenon is described as “Rightward Orienting Bias” (attention to the right side is biased even if there is no special neglect). This study excluded participants with USN in the assessment on paper, but some participants may have had biased attention to the right and hence, difficulty paying attention to the left. Potential USN during motion may have been detected by passing through a narrow opening. In short, if there is a network failure due to a right hemisphere injury, recognition and attention to the paretic side may be impaired, and it is possible that movements predominant on the non-paretic side repeatedly fail.
Second, thalamic lesions may also contribute to “Rightward Orienting Bias.” The thalamus aggregates sensory information and contributes to the formation of a body schema (Massion, 1992). The thalamus is also involved in the neural network of spatial attention (Corbetta and Shulman, 2011); damage to the right hemisphere causes imbalance in the left and right dorsal attention systems. Thus, spatial factors, such as eye movements and attention, shift to the right space. Although a previous study (Corbetta and Shulman, 2011) explained the USN mechanism, this result may indicate that “Rightward Orienting Bias” can be observed without the USN. Further research is needed to elucidate the mechanism of the behavioral characteristics of thalamic lesions.
Third, the degree of motor paralysis of the lower limbs influences the determination of entry direction. Lower limb BRS stage 3 is less supportive and is a segregation movement due to motor paralysis (Brunnstrom, 1966). Multiple regression analysis has previously been performed to determine whether individuals with stroke stepped on the paretic or non-paretic sides (Mansfield et al., 2012). The degree of motor paralysis in the lower limb and the amount of load on the paretic side are related to the paretic side step. Thus, decreasing the load on the paretic side tends to be predominant on the non-paretic side. In this study, it is possible that individuals with stroke who had moderate paralysis (lower limb BRS stage 3) showed predominantly obstructive avoidance strategies on the non-paretic side due to decreased supportability on the paretic side and difficulty in separation movement.
Contrary to our hypothesis, the ability to judge passability did not affect collision or direction of entry. The width that can be passed without body rotation was measured in the image; however, participants rotated and passed through most of the opening widths. Thus, image and actual behavior may have different judgment processes. In the future, it will be necessary to examine its relationship with the image ability to determine the direction of entry.
We performed a hypothesis verification-type multiple regression analysis based on the number of participants, but the variables used in this study were limited. The minimum passable width of walking-through the opening was measured as an index of sway during walking, but it is not clear whether it accurately indicated the left-right sway or load deviation during walking. Therefore, in the future, it may be necessary to investigate the load ratio and lateral sway during normal walking and include them as dependent variables.
Conclusions
We found the collision rate in individuals with stroke was related to a large left-right sway when walking straight through a narrow opening and a slow TUG test speed. Right hemisphere injury (i.e., left hemiplegia), a thalamic lesion, and a BRS stage of 3 or less were associated with individuals entering the opening from the non-paretic side. Interventions to improve walking ability may improve collision avoidance. Furthermore, individuals with stroke with right hemisphere injury or thalamic lesions may have poor use of their paretic sides; improving their awareness of using this side in daily living would increase awareness of the paretic body and reduce the likelihood of falls occurring due to contact with obstacles.
Footnotes
Acknowledgments
The authors would like to thank Editage (www.editage.com) for English language editing.
Conflict of interest
None declared.
Funding
This work was supported by the Japan Society for the Promotion of Science (KAKENHI Grant Number 19K19845) awarded to Daisuke Muroi. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.