
Abstract
BACKGROUND:
While expert consensus recommendations support the use of speech and language therapy (SLT) for patients with functional speech disorder (FND-speech), there are limited published data on clinical outcomes.
OBJECTIVE:
To retrospectively report the treatment outcomes and clinical characteristics of patients with FND-speech that attended outpatient SLT as part of a multidisciplinary program for functional neurological disorder (FND).
METHODS:
In this case series, we included adult patients with FND-speech that consecutively participated in outpatient SLT at our institution between October 2014 and September 2021. Baseline demographic and neuropsychiatric characteristics were extracted from the medical records, along with data on FND-speech phenotypes, number of treatment sessions received, and clinician-determined outcomes. Only descriptive statistics were used to report findings.
RESULTS:
Twenty patients met inclusion criteria; ages ranged from 21–77, with a mean of 51.6±16.2 years. 85% of the cohort presented with mixed FND-speech symptoms. Patients attended a range of 2–37 visits, with an average of 9.2±8.0 visits over 4.4±3.5 months. At the last treatment session, 3 patients were asymptomatic, 15 had improved, and 2 had not improved; 8 individuals that improved received video telehealth interventions.
CONCLUSION:
This case series lends additional support for outpatient SLT in the assessment and management of individuals with FND-speech, and may help clarify patient and provider treatment expectations. Additional prospective research is needed to investigate baseline predictors of treatment response and further define the optimal frequency, intensity, duration, and clinical setting for SLT delivery in this population.
Keywords
Introduction
Patients with functional neurological disorder (FND), a condition at the intersection of neurology and psychiatry, present with a range of neurological symptoms such as abnormal movements, convulsions, speech difficulties, dizziness, sensory deficits, and/or cognitive concerns (Aybek & Perez, 2022; Finkelstein et al., 2022; Hallett et al., 2022). While historically neglected and framed as a diagnosis of exclusion, renewed clinical and research interest in the field has been catalyzed by the appreciation that physical examination signs and semiological features can be used to provide a rule-in diagnosis. Furthermore, modern-day mechanistic and etiological formulations of FND leverage the biopsychosocial formulation to provide a nuanced conceptualization of this patient population. For a range of functional motor symptoms, including functional hyperkinetic and hypokinetic movements, weakness, and speech disorders (FND-speech), a new multidisciplinary treatment paradigm is emerging emphasizing patient education, physical rehabilitation, and psychotherapy (LaFaver et al., 2020; LaFaver & Ricciardi, 2022; Nielsen et al., 2015). A major step forward has been the establishment of consensus recommendations for physical therapy, occupational therapy, and speech and language therapy (SLT) for FND (Baker et al., 2021; C. Nicholson et al., 2020; Nielsen et al., 2015). While clinical research in functional movement disorders and functional weakness (abbreviated collectively as FND-movt) as well as functional seizures (FND-seiz) has greatly advanced over the past two decades (Baslet et al., 2021; Perez et al., 2021), less research has been conducted in patients with FND-speech.
FND-speech phenotypes as described in the literature include functional stutter, prosodic disturbance/foreign accent, and articulatory disturbance/infantile speech (Baizabal-Carvallo & Jankovic, 2015; Baker et al., 2021; Chung et al., 2018; Duffy, 2016; Duffy, 2019; Maurer & Duffy, 2022; McWhirter et al., 2019). Functional stutter is typically characterized by hesitations, sound, syllable, or word repetitions, or prolongations interrupting the overall fluency of speech (Maurer & Duffy, 2022). For individuals exhibiting functional foreign accent syndrome (described as a primarily prosodic disturbance) variations in syllable/word stress, intonation, and atypical grammar patterns result in listener perception of “accented” speech (Baker et al., 2021; McWhirter et al., 2019). Functional articulatory disturbance/infantile speech is typically characterized by speech sound distortions or substitutions that may resemble developmental errors (despite sudden emergence in adults) and/or associate with excessive articulatory effort (Baker et al., 2021; Maurer & Duffy, 2022). While several examination signs have been identified to inform the diagnosis of FND-speech, overarching diagnostic features include prominent variability, distractibility, modifiability, and inefficient/non-ergonomic movement patterns (Baker et al., 2021; Duffy, 2016; Maurer & Duffy, 2022).
In terms of treatment, SLT is recognized as an emerging first line intervention although there are no published prospective controlled clinical trials in patients with FND-speech to date (Baker et al., 2021). A small body of existing literature highlights the potential for improvement in FND-speech symptoms following SLT, but these articles are mostly limited to case studies or a narrow subset of clinical speech presentations (Baker et al., 2021; Barnett et al., 2019; Freeburn, 2022; Jones et al., 2011; Utianski & Duffy, 2022). In the largest retrospective cohort study conducted in 69 patients with a functional stutter, 47% of individuals who received treatment became asymptomatic and 25% improved to near normal in the diagnostic SLT session or the first treatment session (Baumgartner & Duffy, 1997). An additional 19% improved but not to near normal in the diagnostic session, and the remaining 9% did not improve before being discharged at the third treatment session. Data from these studies and other small cohorts have lent support not only to a role for SLT in the management of FND-speech, but also underscore that most patients seemingly improve after only a few treatment sessions (Duffy, 2016; Roth et al., 1989; Utianski & Duffy, 2022). More recently, based on available data and expert opinion, consensus recommendations for the management of FND-speech and other functional communication disorders using SLT were published in 2021 (Baker et al., 2021). Overarching components of SLT treatment for FND-speech include education on the diagnosis, identification of symptomatic behaviors, introducing strategies to facilitate more automatic speech, and extending instances of therapeutic success towards a range of desired activities.
In this retrospective case series, we aim to report on the clinical characteristics and outcomes of patients with FND-speech referred for outpatient SLT within a multidisciplinary FND program (Matin et al., 2017; Perez et al., 2016). Our goal is to add to the treatment literature by reporting on a case series of 20 patients with FND-speech. Given that neuropsychiatric variables have been associated with clinical outcomes in other FND populations (Gelauff et al., 2014, 2019; Goldstein et al., 2022; Jalilianhasanpour et al., 2019), a secondary goal is to descriptively examine relationships between clinical characteristics, number of SLT treatment sessions, and clinical outcomes. Lastly, we make note of the number of patients that received virtual (video telehealth) SLT treatment to document the potential use of this mode of treatment delivery, which has grown exponentially since the onset of the COVID-19 pandemic – including in the FND field (Gandolfi et al., 2022; Perez, 2021; Watson et al., 2022).
Methods
Institutional review board (IRB) approval was obtained from the Mass General Brigham Human Research Committee. Individual informed consent was not required by the IRB for this retrospective chart review study. Given the small sample size and lack of available quantitative measurements in this cohort, only descriptive statistics were used to report findings.
Chart review
We reviewed the medical records of 24 consecutive individuals referred for the first time to outpatient SLT from an outpatient FND clinic at the Massachusetts General Hospital beginning from October 2014 through the end of February 2021. All patients were diagnosed with clinically established FND-speech using rule-in features (American Psychiatric Association, 2013; Baker et al., 2021) at their FND clinic appointment as assessed by a neurologist or neuropsychiatrist, and this diagnosis was confirmed at the SLT evaluation (conducted for all patients by co-author J.F., a certified and licensed speech and language pathologist with 7 years of experience treating patients with FND-speech). Four of the 24 patients were excluded, as SLT treatment sessions were never initiated (3 lost to follow-up, 1 asymptomatic at evaluation). The remaining sample (n = 20), all fluent in English (2 of 20 individuals identified Spanish as their first language and selected English as their preferred language for healthcare), had ended treatment by September 2021. Given the focus on FND-speech, isolated functional voice disorders (FND-voice) and/or those referred to SLT for cognitive symptoms without a concurrent FND-speech were excluded (Baker, 2016).
Demographic characteristics and baseline clinical variables were extracted from FND clinic notes prior to SLT intake and from the evaluation note of the single speech and language pathologist. Variables included FND-specific clinical features (including FND-speech phenotype and the presence of other functional neurological symptoms), medical and neuropsychiatric characteristics (e.g., concurrent pain, fatigue, insomnia, lifetime depression, anxiety), and any other FND-specific concurrent treatment (e.g., physical therapy, psychotherapy).
SLT assessment
All patients participated in a full motor speech and language examination with perceptual analysis and description by the speech and language pathologist (co-author J.F.) as consistent with broad clinical practice recommendations for all motor speech disorders (American Speech-Language-Hearing Association, 2022). The initial assessment ranged from 60 to 120 minutes in length. Examination components included an in-depth case history obtained via chart review and interview, an oral mechanism examination, and a variety of speech production tasks including reading, oral picture description, and free conversation. In addition to clinical observations made during the session, speech samples were recorded and qualitatively analyzed. Perceptual analyses of speech samples focused on patient-specific metrics (e.g., voice quality, fluency, articulatory precision), as well as positive rule-in features of FND-speech including internal task-to-task inconsistency and distractibility (Baker et al., 2021; Utianski & Duffy, 2022). Initial trials of speech modification strategies to assess stimulability for change were typically performed at the assessment, albeit with some variability due to time constraints.
Importantly, the assessment and treatment course for this cohort partially overlapped with the COVID-19 pandemic. As such, virtual (video telehealth) care was at times offered in place of in-person treatment due to hospital policy and/or patient preferences in addition to the clinician’s determination of appropriateness. Virtual care sessions did not differ inherently from in-person sessions in terms of targets, scope, or frequency.
Definition of FND-speech impairments observed on SLT examination
Each patient’s speech difficulties on SLT examination were described in the clinician’s initial assessment based on the motor speech subsystems affected. Traditionally, the five speech subsystems include respiration (speech breathing), phonation (voice quality), articulation (formation of specific speech sounds), resonance (shaping of airflow by oral/nasal cavities), and prosody (stress, rhythm, and intonation of speech) (Duffy, 2019). Two additional characteristics, speech fluency and agrammatism, were also recorded due to their prominence in this population. For the purposes of data collection, fluency was defined as disruptions to the continuity and consistency of speech rate, and agrammatism as disruptions in the grammar and/or syntax of a patient’s verbal language output. When applicable, functional motor symptoms affecting speech (e.g., dis-coordination of orofacial structures) were also noted.
Definition of general FND-speech phenotypes
Three FND-speech phenotypes – functional stutter, prosodic disturbance/foreign accent, and articulatory disturbance/infantile speech – have been described in the literature as detailed earlier (Baker et al., 2021; Duffy, 2019; McWhirter et al., 2019). Each patient in this cohort exhibited hallmark characteristics of at least one of these three categorical descriptors, and corresponding phenotypes were recorded based on the speech and language pathologist’s clinical descriptions of patient presentation.
SLT treatment
Treatment sessions, whether conducted in the clinic or virtually, ranged from 45 to 60 minutes in length and were also conducted by the same speech and language pathologist (co-author J.F.). Therapeutic interventions paralleled the principles found in the SLT consensus recommendations for FND-speech (Baker et al., 2021), beginning with patient education and counseling followed by initiation of symptomatic treatment. The initial treatment session was often dedicated to deepening the patient’s understanding of their atypical speech production and the underlying mechanisms at play (e.g., excess effort, musculoskeletal tension). Once shared language and a common understanding of therapy goals were established, the patient participated in treatment tailored to modifying their atypical speech characteristics while concurrently addressing unhelpful thoughts and behaviors contributing to communication disruptions. Given the importance of this psychotherapeutically-informed counseling alongside the motor speech focused symptomatic interventions, the precise targets of each SLT session necessarily varied from patient to patient. The recommended frequency of sessions typically decreased over the course of treatment as commensurate with patient improvement, but frequency of sessions also varied based on other relevant clinical factors and patient availability.
Symptomatic treatment followed a stepwise progression. Initially, both general and symptom-specific strategies were used to facilitate improved speech output. Broadly used strategies included attempts to facilitate a return to “natural” speech patterns through automatic and reflexive sounds, while symptom-specific interventions were tailored to target the specific breakdowns in one or more speech subsystems (see Table 1). Also, see Freeburn, 2022; Utianski & Duffy, 2022 for a case-based illustrations of the treatment of FND-speech. Following successful facilitation of a more typical speech pattern, the treatment targeted application of these learned strategies to a hierarchy of progressively more complex and lengthier speech tasks (e.g., from repetition to reading to structured conversation). The patient’s demonstrated accuracy and self-monitoring of speech production at each respective level was used by the clinician to gauge readiness to advance within this hierarchy.
Sample speech facilitation strategies
Sample speech facilitation strategies
Note: additional speech strategies can be found elsewhere (Baker et al., 2021; Freeburn, 2022).
Once patients achieved the goal of producing accurate speech during unstructured conversation, further goals targeting carryover to daily communication environments were established and targeted within the clinic (e.g., applying skills to novel situations such as making a phone call from the SLT office), as well as outside of the clinic. The final (discharge) treatment session covered strategies for self-cuing in case of future symptom relapse.
For individuals with FND-speech and concurrent cognitive complaints, SLT treatment targeting metacognitive education and implementation of strategies to support cognitive communication functioning was also introduced during the therapy course using approaches detailed elsewhere (Freeburn, 2022).
Information on SLT outcomes was extracted from clinician notes on the last available SLT treatment session attended by the patient. The primary outcome measure was clinician-determined improvement based on a combination of perceptual measures and patient progress toward treatment goals. “Asymptomatic” patients were noted as being completely or essentially back to their baseline speech pattern as gauged by clinician impression. Patients rated as “improved” had chart-documented evidence of significant and applicable improvement with implementation of speech strategies during clinical tasks or general improvement in FND-speech symptoms over the course of treatment. When patients reached either substantial improvement or a notable plateau in progress, discharge from SLT was recommended. Henceforth, the term “at discharge” will be used to describe the outcomes detailed in either the SLT clinician’s discharge note or the patient’s last known follow-up visit, and “improved” patients will refer to those who improved but were not asymptomatic at discharge.
Patient outcomes extracted from SLT notes also included the type of treatments received and targets achieved by each patient at discharge. For example, an outcome at the “conversation level” indicates that the patient consistently applied learned speech strategies to produce accurate speech during >90% of utterances during structured clinical conversational tasks.
Results
Sixteen cisgender females and 4 cisgender males with FND-speech underwent SLT treatment (see Table 2). Ages ranged from 21–77, with a mean of 51.6±16.2 years old. None were working full time, and 11 patients were on or applying for disability. Eighteen of 20 patients had a concurrent FND-movt (functional weakness (n = 12); other functional motor symptoms (n = 17)). Four patients had functional seizures (FND-seiz). In this cohort, patients had an average FND illness duration of 3.2±3.5 years (range: 0.3–14.4); FND-speech symptoms had been active for 3.0±3.6 years (range: 0.3–14.4).
Demographic and clinical characteristics of 20 patients with FND-speech
Demographic and clinical characteristics of 20 patients with FND-speech
Note: all averages are reported as mean (
In terms of FND-speech impairments observed on initial SLT examination, 17 patients (85%) presented with speech symptoms affecting multiple subsystems (see Fig. 1). Clinician evaluation results yielded the following disturbances: respiration (n = 9), phonation (n = 10), articulation precision (n = 12), resonance (n = 1), prosody (n = 8), speech fluency (n = 16), and agrammatism (n = 3). Five patients also presented with other FND-speech symptoms including spontaneous vocalizations, dis-coordinated oral motor movement, and/or reduced rate of speech.
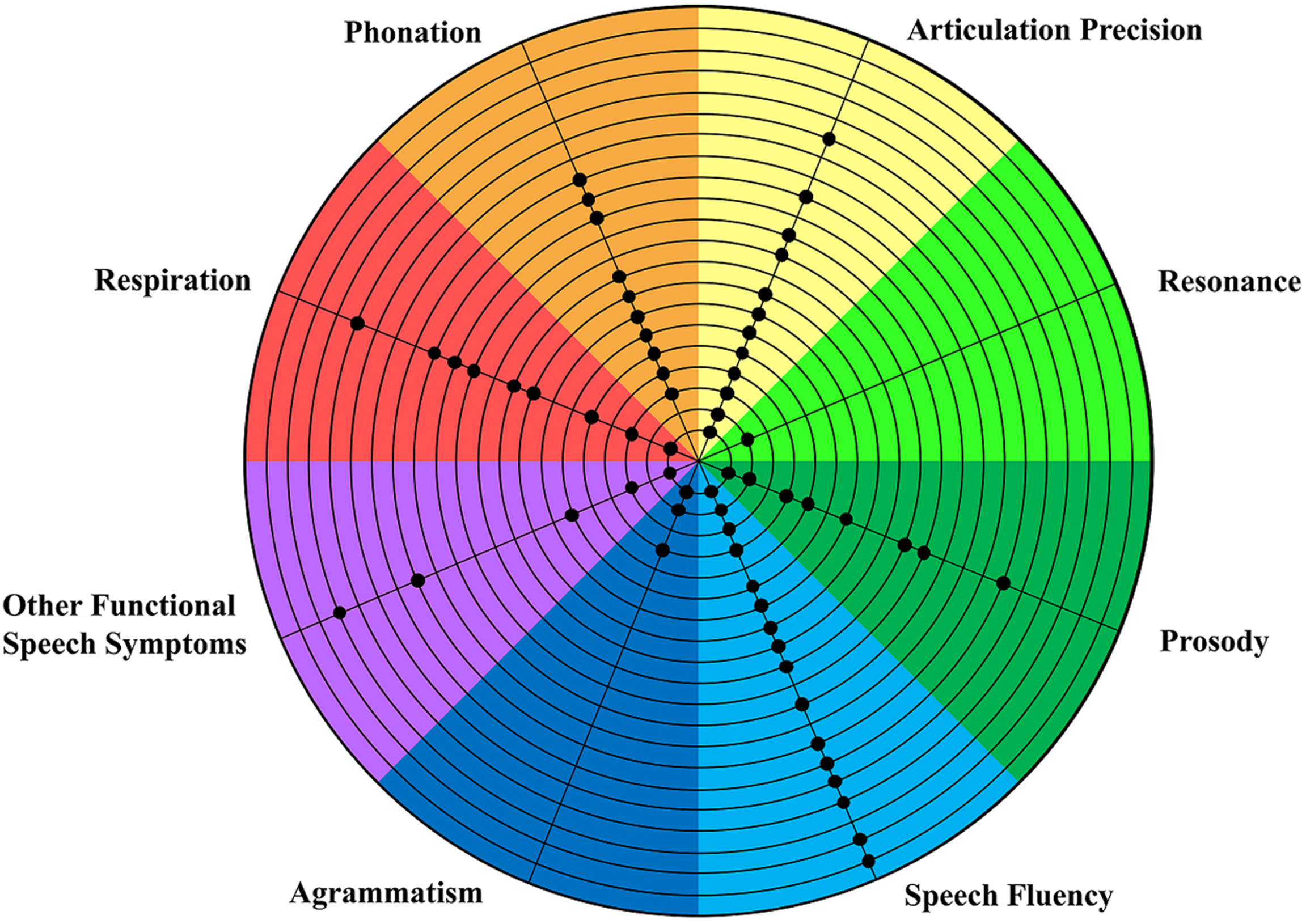
Patient speech impairments on speech and language therapy examination. The presenting speech impairments, categorized by speech subsystem(s) affected, are displayed for all patients in this case series based on speech and language therapy (SLT) intake data. Each circle represents one patient, and the pieces of the pie represent categorized impairments by speech subsystem.
Regarding general FND-speech phenotypes, 19 patients presented with hallmark characteristics of functional stutter, 8 with prosodic disturbance/foreign accent, and 8 with articulatory disturbance/infantile speech. Six patients presented with concurrent characteristics of FND-voice. Ten patients (50%) exhibited characteristics of more than one FND-speech phenotype over the course of the examination.
At the SLT evaluation, all 20 patients verbalized understanding of their diagnosis (note: only individuals who demonstrate some initial acceptance of the diagnosis at their FND clinic neurology evaluation are referred for FND-specific treatments), and 19 patients successfully identified and described their speech symptoms. Clinician-initiated strategies aimed at facilitating improved speech production resulted in observable improvement in 11 patients at the first treatment session, an additional 6 patients by the third treatment session, and 1 patient by the eighth treatment session, even if this improvement was only on a specific task and not generalizable across settings. Additionally, a subset of individuals were concurrently participating in physical therapy (n = 11), occupational therapy (n = 9), and/or psychotherapy (n = 13) along with their SLT treatment.
The total number of SLT visits (including the evaluation) per patient ranged from 2–37 visits, with an average of 9.2±8.0 visits over 4.4±3.5 months; patients attended visits 2.1 times per month on average. Due to the COVID-19 pandemic, 8 patients had some video telehealth SLT visits (average of 7.4±5.5 virtual visits over 4.4±2.6 months in overall treatment; range: 1–15 virtual visits, on average 1.7 visits per month). These patients represented 8 of 15 in the “improved at discharge” category.
At discharge, 3 patients were asymptomatic, 15 had improved, and 2 had not improved. We split the cohort into sub-groups based on these clinical outcomes (see Fig. 2). Asymptomatic patients were 48.0±8.9 years old, and mean FND-speech illness duration was 2.4±3.4 years; improved patients were 51.3±18.3 years old, and mean FND-speech illness duration was 3.3±3.9 years; not improved patients were 59.0±0.0 years old and mean FND-speech illness duration was 1.8±1.3 years. All asymptomatic patients were either on or applying for disability, all had a concurrent FND-movt, 1 had FND-seiz, all had current cognitive symptoms and pain, and 1 had current fatigue; 7 improved patients were on or applying for disability, 13 had FND-movt, 3 had FND-seiz, 12 had current cognitive symptoms, 10 had current pain, and 8 had current fatigue; 1 patient who had not improved at discharge was on or applying for disability, both had FND-movt, none had FND-seiz, 1 had current cognitive symptoms, both had current pain, and 1 had current fatigue.
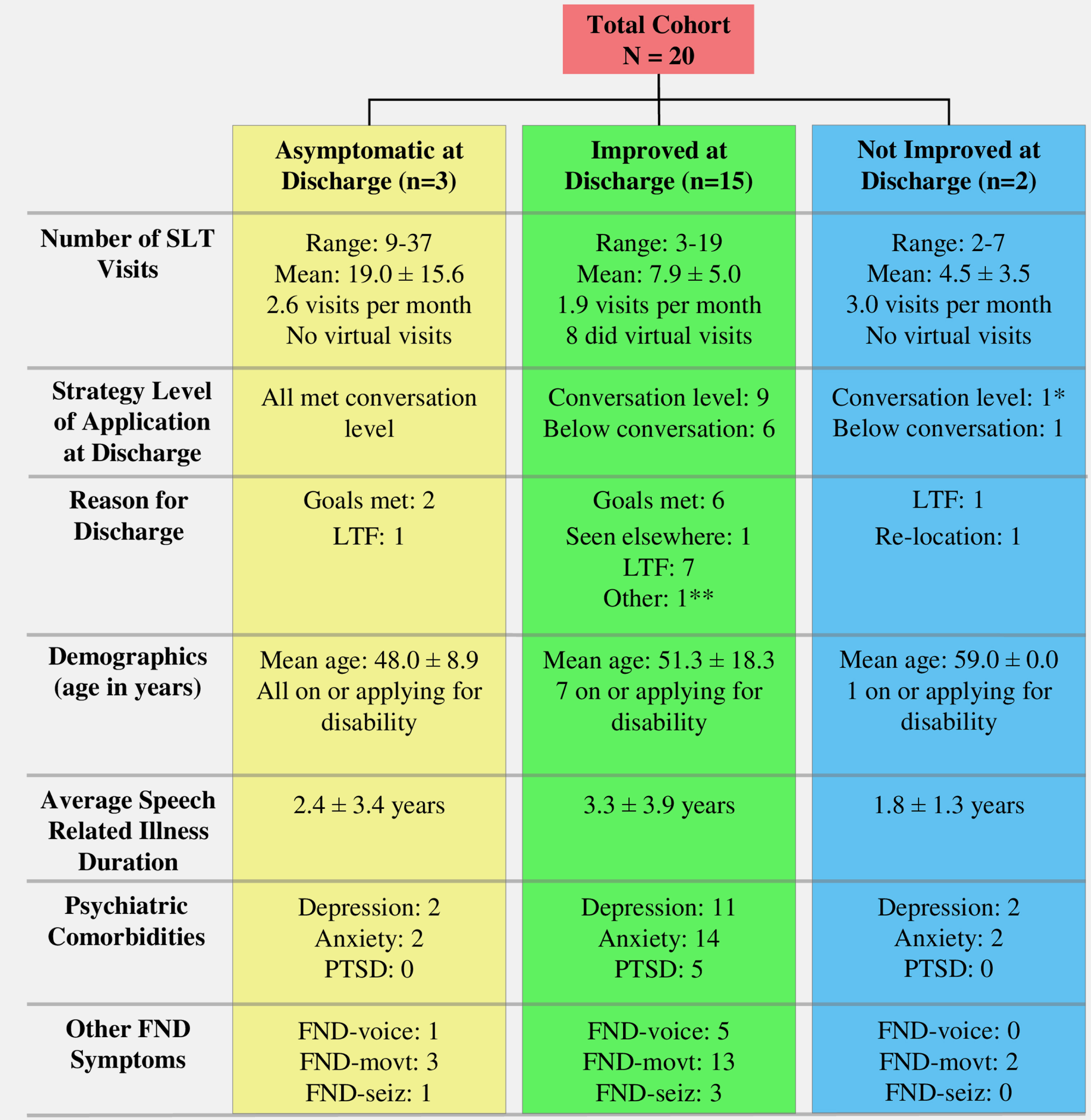
Clinical outcomes and patient characteristics in speech and language therapy. Patient outcome measures and clinical characteristics were divided by clinician-reported patient improvement. Note: measures of asymptomatic, improved, or not improved at discharge were all determined by clinician impression. LTF: Lost to Follow-up. FND-movt includes functional weakness and functional movement disorders. *Patient arrived at and finished SLT treatment at a conversational level, with a functional stutter. **Patient left treatment due to no longer being able to receive virtual out-of-state care.
Data on SLT visits are as follows: asymptomatic patients attended a range of 9–37 visits, with a mean of 19.0±15.6 visits over 7.4±7.9 months, improved patients attended a range of 3–19 visits, with a mean of 7.9±5.0 visits over 4.2±2.0 months; patients who had not improved attended a range of 2–7 visits, with a mean of 4.5±3.5 visits over 1.5±1.7 months. One asymptomatic patient and 6 improved patients received cognitive treatment in addition to FND-speech symptom treatment in SLT.
Reasons for discharge from SLT were as follows: 2 asymptomatic patients were discharged by the clinician and 1 was lost to follow-up; 6 improved patients were discharged by the clinician, 7 were lost to follow-up, and 2 either transferred to a different clinician or lived out-of-state and could no longer attend virtual SLT sessions; 1 not improved patient was lost to follow-up and 1 left treatment due to a re-location.
This case series of 20 patients with FND-speech adds to the literature supporting a role for SLT in the management of this population. Specifically, 3 individuals achieved clinician-determined symptom resolution, and an additional 15 individuals improved at the end of outpatient SLT. Consistent with the treatment literature in patients with FND-speech (Duffy, 2016; Utianski & Duffy, 2022), most individuals used initial SLT treatment strategies to alleviate speech difficulties early in the treatment course (17 by the third treatment session, 11 with some success in the first treatment session). However, in our cohort the majority needed multiple treatment sessions to achieve clinical improvement (a range of 9–37 sessions in the asymptomatic group and a range of 3–19 sessions in the improved group). These data underscore the need for additional research examining the efficacy of SLT treatment for patients with FND-speech, with a particular effort needed to refine the optimal intensity, frequency, and duration of treatment.
Treatment impact of non-motor symptoms and other psychosocial features
A notable observation is that a subset of patients in the asymptomatic and improved categories were “on or applying for disability” and/or endorsed other bodily symptoms such as pain, fatigue, and cognitive complaints. These factors in other FND populations have been associated with poor clinical outcomes and reduced quality of life (Gelauff & Stone, 2016; Glass et al., 2018; Maggio et al., 2020; Věchetová et al., 2018). For example, a concurrent diagnosis of somatization disorder (indicative of prominent bodily complaints including pain) correlated with poor prognosis in a 14-year prospective study of clinical outcomes in patients with functional weakness (Gelauff et al., 2019). In patients with FND-seiz, concurrent pain syndromes negatively correlated with quality of life (Myers et al., 2012); the presence of cognitive complaints has also been linked to decreased quality of life in patients with FND-movt (Věchetová et al., 2018). Given the lack of prospective controlled clinical trial research in FND-speech to date, our case series findings suggest that the inclusion of a broad spectrum of FND-speech cases would likely be feasible for initial SLT trials. Similarly, being “on or applying for disability” does not appear to preclude the appreciation of positive communication-related clinical outcomes in this population.
Virtual (Video Telehealth) SLT for FND-Speech
Given that 8 of 15 patients rated as improved at discharge received care virtually, this case series also lends support to a role for delivering SLT for FND-speech via video telehealth (Perez, 2021; Perez et al., 2020). Several pilot video telehealth studies have been performed in patients with FND. For example, a recently published study identified that use of 12 sessions of weekly physical therapy delivered via telemedicine following completion of a 5-day intensive rehabilitation program showed favorable clinical outcomes compared to self-management (Gandolfi et al., 2022). Other articles have indicated similar efficacy of virtual treatment (Demartini et al., 2020; Perez, 2021). Given the reduced prevalence of FND-speech in comparison to other subtypes of FND (e.g., FND-seiz, FND-movt) (Aybek & Perez, 2022), it is likely that leveraging video telehealth treatment delivery approaches will aid both participant recruitment for FND-speech focused clinical trials and the availability/dissemination of consensus treatment recommendations in the field (Baker et al., 2021).
Other considerations
From an FND-speech phenotypic characterization perspective, this case series raises some interesting questions. Most notably, across the 3 general phenotypes (i.e., functional stutter, prosodic disturbance/foreign accent, and articulatory impairments/infantile speech), 50% of individuals in this cohort had mixed speech phenotypes. Furthermore, 18 of 20 individuals with FND-speech had a concurrent functional motor symptom (across the spectrum of hyperkinetic and hypokinetic FND-movt that includes functional limb weakness); 4 of 20 individuals were also diagnosed with FND-seiz. The frequency of mixed FND presentations that includes functional speech symptoms as part of the overall symptom complex further supports the need for a transdiagnostic approach to the characterization and treatment of patients with FND that cuts across the FND-speech, FND-movt, and FND-seiz literatures (Lidstone et al., 2022; Matin et al., 2017; Tinazzi et al., 2020). Interesting differences to further investigate include that the average age of patients in this cohort was 51.6 years old, with a mean speech-related illness duration of 3 years. If such findings are replicated in large, prospectively collected cohorts, this would suggest that FND-speech onset occurs over a decade later than typical onset of functional dystonia and FND-seiz (Lidstone et al., 2022). Thus, while frequent mixed symptom presentations suggest convergent neural mechanisms and etiological considerations, age of onset differences lend support to some potential neurobiological differences that also warrant more research. Lastly, from an SLT perspective, it is notable that there is not a simple one-to-one correspondence between general FND-speech phenotypes as described in the literature and speech impairments detected on SLT examination. For example, patients exhibiting hallmark perceptual characteristics of “infantile speech” presented with speech impairments across multiple subsystems not limited to articulation. This finding highlights the need for broader integration of FND-speech perceptual phenotypes and speech impairments, perhaps resulting in further refinement of phenotype labels.
Limitations and future directions
There are several limitations to this present effort. This is a small, retrospectively collected patient sample that used only clinically available medical record data. While all patients in this cohort had speech difficulties impairing social and/or occupational functioning, we did not have a more specific clinician-rated or self-report measure of the severity of their functional speech symptoms (nor of their overall FND symptom complex more broadly). Future research should include prospective data collection with standardized baseline and post-treatment speech and language assessments (including long-term follow-up data), with a range of objective, clinician-rated, and patient-reported symptom severity measures (T. R. Nicholson et al., 2020; Pick et al., 2020). Pre-treatment psychometric characterization of neuropsychiatric variables will also aid future research regarding potential factors predicting response to SLT interventions for FND-speech. Furthermore, it is important to note that most patients in this FND-speech cohort were concurrently receiving other physical rehabilitation and/or psychotherapy interventions. While a multidisciplinary (and interdisciplinary) approach to patient care is encouraged for many patients with FND (LaFaver & Ricciardi, 2022), such naturalistic interventions make it difficult to explicitly link clinical improvement to one specific treatment modality. Future research is also encouraged to include a broad data analysis of all concurrent treatment progression, as it is unclear in this sample if FND-speech improvement corresponded with overall FND symptom complex improvement.
Conclusion
Outpatient SLT for the management of patients with FND-speech appears to be a viable therapeutic option. To further operationalize the use of SLT for FND-speech, prospective clinical trials (including using video telehealth) are needed to further advance the field.
Footnotes
Conflict of interest
D.L.P. has received honoraria for continuing medical education lectures and royalties from Springer Nature for a textbook on Functional Movement Disorder, is a paid senior editor to Brain and Behavior, is on the editorial board of Epilepsy & Behavior, and has received funding from the NIH and the Sidney R. Baer Jr. Foundation unrelated to this work.
Acknowledgments
None to report.
Funding
None to report.