
Abstract
BACKGROUND:
Brain-derived neurotrophic factor (BDNF) promotes activity-dependent neuroplasticity and is released following aerobic-exercise.
OBJECTIVE:
Feasibility and efficacy of 1.Moderate-Intensity Cycle-Ergometer-Training (MI-ET) and 2.Low-Intensity Circuit-Training (LI-CT) on BDNF-serum-concentration in chronic-stroke and consequently efficacy of motor-learning in varying BDNF-concentrations (neuroplasticity being the substrate for motor-learning) via upper-limb robotic-training (RT) in both groups.
METHODS:
Randomised-control feasibility-study. 12-week, 3x/week intervention, 17 chronic-stroke-survivors randomized into: (1) MI-ET&RT or (2) LI-CT&RT. Both groups completed 40 mins MI-ET or LI-CT followed by 40 mins RT. Feasibility outcomes: (1) screening and enrollment-rates, (2) retention-rates, (3) adherence: (i) attendance-rates, (ii) training-duration, (4) adverse events. Primary clinical outcomes: 1. serum-BDNF changes pre-post training (immediate) and pre-training basal-levels over 12-weeks (long-term). 2.upper-limb performance with Action-Research-Arm-Test (ARAT). Additionally, feasibility of an embedded health economic evaluation (HEE) to evaluate health-costs and cost-effectiveness. Outcomes: cost-questionnaire return-rates, cost-of-illness (COI) and Health-Utitility-Index (HUI).
RESULTS:
21.5% of eligible and contactable enrolled. 10 randomized to MI-ET and 7 to LI-CT. 85% of training-sessions were completed in MI-ET (306/360) and 76.3% in LI-CT-group (165/216). 12-weeks: Drop-outs MI-ET-10%, LI-CT-43%. Clinical outcomes: No significant changes in immediate or long-term serum-BDNF in either group. Moderate-intensity aerobic-training did not increase serum-BDNF post-stroke. Individual but no group clinically-relevant changes in ARAT-scores. HEE outcomes at 12-weeks: 100% cost-questionnaires returned. Group-costs baseline and after treatment, consistently favouring MI-ET group. COI: (1-year-time-frame): MI-ET 67382 SD (43107) Swiss-Francs and LI-CT 95701(29473) Swiss-Francs.
CONCLUSION:
The study is feasible with modifications. Future studies should compare high-intensity versus moderate-intensity aerobic-exercise combined with higher dosage arm-training.
Keywords
Background
Stroke is the second leading cause of acquired disability in adultsand stroke survivors worldwide number 33 million (Feigin et al., 2014). Only 18% –50% of the stroke population regain full function of the upper limb, which negatively impacts independence in activities of daily living (ADLs) and social participation (Faria-Fortini et al., 2011), resulting in a significant economic burden (Andlin-Sobocki et al., 2005; Fattore et al., 2012). Neuroplasticity is the neuronal substrate for functional recovery following stroke (Liepert et al., 2000; Overman & Carmichael, 2014). Motor control and functional improvement of both upper and lower limbs occur for the most part within the first eight to twelve weeks post-stroke (Kwakkel et al., 2004; van Kordelaar et al., 2014) and are primarily explained by spontaneous “reactive” neurobiological recovery (Cortes et al., 2017; Kwakkel et al., 2006; Winters et al., 2018). This period coincides with a time-dependent set of molecular and cellular changes which create a plasticity promoting environment within cortical, subcortical and spinal neural networks mediating functional improvement (Nudo, 2007).
Brain-derived neurotrophic factor (BDNF) is one of several neurotrophic factors which play a significant part in this process by influencing the development, survival and function of neurons (Park & Poo, 2013; Poo, 2001). BDNF also promotes activity-dependent neuroplasticity influencing long-term potentiation (LTP), synaptogenesis, axonal and dendritic growth and remodelling (Kermani & Hempstead, 2007; Knaepen et al., 2010; Poo, 2001).
Ten to twelve weeks after stroke the initial plasticity-promoting environment has receded and reactive neurobiological recovery ceases (Kwakkel et al., 2006; Nudo, 2007; van Kordelaar et al., 2014). Subsequent functional gains, particularly of the upper limb,are usually minimal beyond this point (Byblow et al., 2015; Cortes et al., 2017; Stinear et al., 2017; Zarahn et al., 2011). Indeed, reduced levels of physical activity commonly lead to long-term decline or loss of function (van de Port et al., 2006).
As the initial period of spontaneous recovery is associated with a plasticity supporting environment, in which BDNF is one of numerous important factors, rehabilitation conducted within a BDNF enriched environment could potentially be more effective, even in chronic stroke.
Studies in both animals and humans indicate that aerobic exercise leads to increased levels of peripheral BDNF (Huang et al., 2014; Knaepen et al., 2010; Ploughman et al., 2015). In rodent models, moderate-intensity aerobic exercise also increases BDNF levels centrally in the hippocampus and sensorimotor cortex (Ploughman et al., 2015; Ploughman et al., 2007) and influences neuroplasticity by increasing axonal regeneration and decreasing concentrations of the growth inhibitor NogoA (Zhang et al., 2013). The importance of BDNF for functional recovery has also been demonstrated. When BDNF was blocked, recovery in rats was stopped despite receiving rehabilitation (Ploughman et al., 2009).
In humans, research indicates that systemic levels of BDNF transiently increase in healthy subjects following a bout of moderate (40–59 % Heart rate reserve (HRR), 64–76 % HR max) to high (60–84 % HR reserve, 77–93 % HR max) intensity aerobic exercise and in persons with disease or disability after low (< 40 % HR reserve, < 64 % HR max) to moderate intensity aerobic exercise and remains raised for 10 to 60 minutes (Billinger et al., 2015; Huang et al., 2014; Knaepen et al., 2010), returning to normal levels during the recovery period (Nofuji et al., 2012). A recent study in chronic stroke patients, showed serum BDNF was significantly increased following a single bout of moderate-intensity exercise but not after low-intensity (Morais et al., 2017).
When the effect of aerobic exercise is investigated without specifically measuring BDNF, the influence on plasticity (Luft et al., 2008) and functional outcomes (Hasan et al., 2016; Pyoria et al., 2007; Pyun et al., 2009) in chronic stroke survivors has also been demonstrated. Increased activation in the cerebellum and midbrain during movement of the paretic limb (Luft et al., 2008) and increased bilateral cortical activation (Enzinger et al., 2009) were shown following aerobic training programmes between 3–6 months. Moderate to highintensity exercise improved cognition and memory (Pyoria et al., 2007; Pyun et al., 2009), lower limb function and upper limb function when combined with specific motor task training (Hasan et al., 2016). Ward et al. demonstrated that high-dose, high-intensity upper limb neurorehabilitation, a component of which was aerobic exercise, improved functional and patient-reported outcomes over a three week period (Ward et al., 2019).
In total this evidence may indicate that moderate-intensity aerobic exercise in chronic stroke patients increases levels of BDNF, potentially inducing neural plasticity. Motor task training within this BDNF-enriched environment may increase the efficacy of rehabilitation enabling functional gains. To our knowledge, studies to date have only investigated the effect of aerobic exercise on BDNF levels or on functional outcomes, as described above. No studies have investigated these three factors in a causal relationship in stroke patients, namely the influence of moderate-intensity aerobic exercise on levels of peripheral BDNF and consequently the efficacy of motor training in this environment. In this study, we aim to evaluate the feasibility of an intervention to investigate whether moderate intensity aerobic exercise increases serum-concentration BDNF and if so, whether upper-limb motor training is more effective in this BDNF-enriched environment. This could provide clinically relevant information about how to increase the effectiveness of neurorehabilitation by potentiating neuroplasticity via moderate intensity aerobic exercise prior to motor learning interventions.
Robotic and sensor-based arm training
Robotic and sensor-based arm training provide high-intensity, intention-driven therapy with performance feedback in a motivating environment. These interventions are based on motor learning principles, in terms of dose and repetition, and can be delivered individually or in groups (Duret et al., 2019; Mehrholz et al., 2015). Training parameters and performance can be specified and recorded, enabling accurate data collection for research purposes (Conroy et al., 2019; Duret et al., 2019; Wittmann et al., 2016).
Health economic evaluation (HEE)
Studies which evaluate the efficacy of interventions, provide evidence to support clinical decision-making regarding effective treatment provision. Such decisions, implicitly or explicitly, also influence the allocation of resources, often in resource-poor healthcare contexts. Clinical trials which incorporate HEE, enable the cost-effectvieness as well as the efficacy of interventions to be evaluated. Assessing whether treatments deliver value for money, provides important information for decision makers at all levels of health care provision regarding the utility of new interventions (Craig et al., 2014; Hughes et al., 2016).
HEE can be defined as the comparative and simultaneous assessment of costs and outcomes of at least two alternative health care technologies (MF et al., 2015). Cost-of-illness (COI) studies do not consider effectiveness in the analysis and are therefore described as “partial” HEE (Jo, 2014).
Study aims
The primary aims of this randomised, controlled feasibility study were to evaluate the feasibility of a threemonth, three times weekly, 80 minute (2×40 minutes) intervention with an embedded HEE in which chronic stroke survivors were allocated to 1. Moderate-intensity aerobic exercise with a cycle-ergometer (MI-ET) and upper-limb robotic or sensor-based training (RT) or 2. Low-intensity aerobic circuit training (LI-CT) and upper-limb robotic or sensor-based training (RT). Further aims were to explore: 1. the influence of the interventions on serum levels of BDNF both immediate: pre and postexercise, and long-term: changes in basal (pre-training) levels over the three-month intervention 2. Upper-limb performance outcomes with the Action Research Arm Test (ARAT) 3. COI of chronic stroke patients pre and post intervention and the cost-effectiveness of the interventions.
Methods
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Northwest Switzerland (Project ID 2018-01249). The study protocol was registered at ClinicalTrials.gov ID: NCT03701035. Registered on 9.10.2018. https://clinicaltrials.gov/ct2/show/NCT03701035. The protocol was based on the “Consolidated Standards of Reporting Trials (CONSORT) Statement: extension to randomised pilot and feasibility trials (Eldridge et al., 2016) (see supplementary materials). The study was conducted in a neurorehabilitation centre in northwest Switzerland.
Data has been made available according to the PLOS data availability guidelines in the OLOS Swiss Portal. DOI: https://doi.org/10.34914/olos:cp7kty7h6zanfh737ionkdqrr4
Participants
Eligibility criteria
Inclusion criteria were first ischemic or hemorrhagic stroke more than 3 months, minimum age 18. Exclusion criteria were no detectable movement throughout the upper-limb (Ward et al., 2019), contraindications to maximal exercise testing according to the American College of Sports Medicine guidelines (Pescatello et al., 2014), concurrent neurological diagnoses e.g. Parkinsons disease, or comorbidities which may prevent adequate participation in the ergometer training or circuit training.
Recruitment and screening
Recruitment was conducted between October 2018 and December 2018 at the REHAB Basel, Clinic for Neurorehabilitation and Paraplegiology. Neurological patients were screened from the clinical information software of the physiotherapy out-patient department. As this process yielded insufficient participants, additional sites were included for recruitment: two clinics for neurorehabilitation, one geriatric hospital, two general hospitals and two private physiotherapy practices in northwest Switzerland. For additional sites, inclusion and exclusion criteria were given to treating physiotherapists who identified potential candidates. All patients meeting inclusion criteria were asked to participate. For interested patients, individual meetings were organised for a detailed screening and to collect informed consent.
Exercise stress testing
According to Best Practice Recommendations for exercise following stroke, participants underwent screening for cardiovascular risk factors before study begin (Mackay-Lyons M et al., 2012–2013). A medically conducted exercise stress test was conducted at the Cardiovascular Pulmonary Rehabilitation Department at the University Hospital Basel (“KARAMBA”) using a peak effort protocol with a 12 lead electrocardiogram (ECG) (Fletcher et al., 2013) prior to randomization. Peak effort is measured using peak oxygen volume (V02Peak) defined as the highest value of oxygen uptake attained upon an incremental or other high-intensity exercise test designed to bring the subject to the limit of tolerance (Whipp & Ward, 1990). This testing allowed unknown contraindications to aerobic exercise to be identified and also provided a valid measure of maximum heart rate to determine training parameters for participants in the aerobic exercise group.
Study arms
Group 1: Moderate intensity cycle-ergometer aerobic training (MI-ET) and upper limb robotic or sensor-based motor training (RT) upto 40 minutes, respectively, 3 times weekly for 12 weeks. Group 2: Low-intensity gait and balance circuit training (LI-CT) and upper limb robotic or sensor-based motor training (RT) up to 40 minutes, respectively, 3 times weekly for 12 weeks.
Interventions
Training was conducted by five trained physiotherapists and four sports therapists from the main study site. Sports therapists implemented the group MI-ET (two therapists per session). The LI-CT and RT group trainings were implemented by physiotherapists (two therapists per LI-CT session, one to two therapists per RT session). Each session began with the 40 minutes of MI-ET (Group 1) or LI-CT (group 2) training. After a break of approximately 20 minutes participants continued with the 40 minutes upper-limb robotic or sensor-based motor training (RT). The break of 20 minutes was defined to ensure that the upper-limb motor training took place within the time window in which serum-BDNF has been shown to be elevated after moderate-intensity aerobic training (Huang et al., 2014; Knaepen et al., 2010). The break included a switch of training area (about 200 m) and the option to have a light snack and drink in the group setting. For practical reasons (availability of equipment and therapists), Group 1. MI-ET trained in the morning, group 2. LI-CT trained in the afternoon. During the intervention period, all other physiotherapy or occupational therapy was stopped. Subjects were asked to continue with their usual daily activity but to desist from other forms of active training or passive therapeutic interventions.
Group 1 Moderate intensity ergometer training (MI-ET)
Aerobic training was based on the FITT (frequency, intensity, time, type) principles of exercise prescription (Billinger et al., 2015). F: 3 times a week, I: moderate intensity 40–59% HRR (Billinger et al., 2015). T: 40 mins (Hasan et al., 2016). T: Cycle Ergometry. Target heart rate (HR) was calculated using the HR reserve method (target HR = (target HR reserve% × [HR max–HR resting]) + HR resting) (Billinger et al., 2014).
Following exercise stress testing and the calculation of the HRR, the maximum time subjects were able to train at the desired aerobic intensity up to 40 minutes was evaluated. For patients not able to complete 40 minutes, the dose-limiting factor: pain, fatigue or effort required, was established (Dite et al., 2015). Time dosage was increased each session in these subjects from between 5–15 minutes per session depending on Dose-limiting Tolerance (DLT) until 40 minutes training was possible. DLT is defined as 1. subjects not able to complete the increased time due to pain, fatigue or effort required 2. the subject was not able to complete Activities of Daily Living (ADL) in the days following training likely due to training (Dite et al., 2015). HR was monitored continuously during aerobic training using the Polar FT1 wristwatch heart rate tracker (Polar FT1, Polar Electro Oy/Polar Electro Inc., 90440 Kempele, Finland) as was perceived exertion using the Borg scale to ensure the correct intensity (score of 12–14/20) (Borg, 1970).
Group 2 Low-intensity, task-oriented gait, balance circuit training (LI-CT)
Task-oriented circuit training following stroke is a model of physiotherapy in which participants practice task-specific, functional exercises in a high-repetition, low-aerobic intensity manner (English et al., 2017). Training is carried out in groups and exercises are progressed as patient function improves (Van de Port et al., 2012; Wevers et al., 2009). This form of circuit training has been shown to improve functional mobility (English et al., 2017; Wevers et al., 2009) and UL function (Blennerhassett & Dite, 2004).
Circuit-training was broadly based on the structure described by van de Port et al. (2012). In a group of 6, participants received a 40-minute, task-oriented circuit training programme with five workstations, 3 times weekly for 12 weeks prior to robotic arm training. Participants worked in pairs at each of five workstations. One participant completed the task for one and a half minutes the other observed, encouraged the fellow participant and helped to keep score of repetitions. The sessions were supervised by two physical therapists. When necessary to maintain safety, supervision or assistance was provided by the treating therapist. On completion the participants switched roles. At time up, each pair moved to the next station. The number of repetitions at each workstation was recorded in a training diary. The workstations included: Standing and throwing balls with the unaffected arm to specific targets. Reaching activities with the unaffected arm whilst sitting on an unstable surface with or without floor contact. Standing balance activities with or without a foam surface. Walking an obstacle course. Sit to stand slowly with or without weights, concentrating on form, posture and correct weight distribution between legs.
Each workstation had three levels of difficulty. Participants were encouraged to progress to the higher level as ability increased.
Upper limb interventions
Each participant conducted a robotic or sensor-based upper-limb training beginning 20 minutes after the MI-ET (group 1) or LI-CT (group 2). Research therapists were trained in the use of devices before study begin by the manufacturer’s educational teams and from therapists experienced in their use in clinical practice.
Five different training devices were selected (Armeo®Spring and Armeo®Senso [Hocoma, Volketswil Switzerland]; Pablo X2®and Amadeo® [Tyromotion, Graz Austria]) to provide different levels of arm and hand support ranging from adjustable suspension systems to wearable sensors (Inertial Measurement Units - IMUs). This enabled the prescription of patient-specific training programmes minimizing floor or ceiling effects of training (Bishop et al., 2017; Wittmann et al., 2016). Device software provided a library of virtual reality, computer game-like programmes which allowed performance feedback and supported high-repetition of movements.
The aim was to provide upper-limb training based on the level of impairment, functional ability and therapy goals of the participants. A programme of up to 40 minutes three times weekly was defined for each participant following a physiotherapy assessment and collaborative goal definition between a research therapist and the participant. For participants unable to complete 40 minutes due to fatigue, lack of concentration or other factors, training duration began at the participant’s maximum tolerance and was gradually increased according to ability (Perez-Marcos et al., 2017). Perceived exertion based on the Borg Scale (Borg, 1970) was monitored during training. The level of difficulty, intended to support motor learning was determined based on the following points: the participant was able to achieve 70–80% of tasks (monitored under “Scores”) at the given game level within the allotted time and the Borg Scale of perceived exertion was rated between 12–15 (Borg, 1970). When indicated, difficulty was increased by either raising game level, game complexity, or by reducing arm weight support. Data of training time and task difficulty was automatically collected for later analysis.
Training in all groups (MI-ET, LI-CT, and RT) was discontinued for the current session if patients experienced any of the following: angina, pain of any kind with particular attention paid to aching in the jaw, neck, down the left or right arm or across shoulders and back, unusual shortness of breath, dizziness, lightheadedness, perceived exertion > 17, abnormal heart rhythm or if participants complained of stiffness or increasing difficulty with active movement (Mackay-Lyons et al., 2013; Perez-Marcos et al., 2017; Pescatello et al., 2014). These symptoms were explained to participants before training began and they were asked to report the appearance of any such symptoms immediately. Training recontinued at the following session only if it was deemed safe following medical examination.
Health-economic evaluation (HEE)
HEE was conducted following domain-specific guidelines (Hughes et al., 2016), from a societal perspective, considering direct (medical and non-medical) and indirect costs while intangible costs were omitted. A two-step bottom-up approach was used for cost estimation. In a first step, health resources consumed were assessed using a (3 months) self-reported (or reported by a relative) cost questionnaire with structured closed questions (Goossens et al., 2000). A second step, consumed health resources were valued using official Swiss Tariffs. Costs were calculated as: units consumed x unit cost. Health profiles were assessed using the European Quality of Life questionnaire (EQ-5D-5L). This is a Patient Reported Outcome Measure which evaluates health status and is valid for use in stroke patients (Golicki et al., 2015). It has five dimensions and five levels and is transformed into weighted single Health Utility Indices (HUI’s) with “one” representing the “best health state” and “zero” representing the the “worst health state” using its crosswalk index value calculator with UK tariff (EuroQol, EuroQol).
Adherence
Based on research regarding barriers and facilitators to physical activity in persons with chronic physical impairments (Butler & Evenson, 2014; Nicholson et al., 2013; Nicholson et al., 2014; Simpson et al., 2011), actions were taken in the five domains “Knowledge”, “Self-efficacy”, “Social-interaction”, “External encouragement and routine participation” and ”Prevention of practical difficulties” to optimise subject participation and programme adherence.
“Knowledge”: Subjects were provided with educational booklets regarding the benefits of cardiovascular training and “question and answer” sessions were provided before the intervention began.
“Self-efficacy”: Subjects were involved in joint participant-therapist decision-making where possible e.g. by formulation of therapy goals and by use of the Borg scale to determine training intensity. Awareness of success gained was supported via feedback (in computer-games and via reported changes in training parameters in all groups).
“Social interaction”: Training took place in groups enabling peer-exchange and support. Snacks and drinks were provided to the groups following MI-ET or LI-CT training to facilitate exchange.
“External encouragement and routine participation”: Exercise sessions were led and monitored by qualifed physiotherapists and sport therapists. The sessions occurred regularly 3 times a week.
“Prevention of practical difficulties”: Transport was provided where necessary. Further difficulties for attending the sessions e.g. appointment times of session, were discussed with the participants and adapted where possible.
Outcomes and measurement procedures
Feasibility outcomes and criteria for success
Using the Criteria for Success model for feasibility outcomes as suggested by Thabane et al. (2010), these were defined as follows. (1) Outcome: Recruitment and enrollment rates. 25% of all eligible and contactable persons identified via recruitment screening strategies are enrolled. (2) Outcome: Retention rates at 12 weeks, 3 and 6 months. Criteria: Drop-outs < 15% in each arm at each point. (3) Outcome: Adherence to training (i) attendance rates: number of sessions attended. Criteria: For each arm, group mean attendance rate is > 80% (for individual participants attendance below 80% is classified as drop-out). (ii) duration of training: total training time. 75% of all participants train for at least 62.5% of maximum possible training minutes (average of at least 50 minutes from each 80 minute session). (4) Outcome: Number of moderate or serious adverse events reported by participants or therapists. Criteria: No moderate or serious adverse events as defined by the Office of Human Research Protections (OHRP), USA (Human & Research Protections (OHRP Guidance. Retrieved 20.12.2018 from https://www.hhs.gov/ohrp/policy/advevntguid.html). (5) Returned cost and EQ-5D-5L questionnaires≥80%.
Clinical outcomes
At baseline standard physiotherapy neurological assessment was done to establish patient goals (Shanmuga Raju P, 2012) and used as the basis for determining robotic training parameters.
Primary outcomes
Serum levels of BDNF were analysed according to the Protocol for Quantification of the biosensis ELISA Kits using the “Mature BDNF Rapid TM ELISA Kit: Human, Mouse, Rat” (biosensis® BDNFTM Rapid ELISA Kit. Biosensis Pty Ltd., 39 Winwood St, Thebarton 5031, SA; Australia). Blood was collected by a study-site nurse 10 to 30 minutes before and after MI-ET or LI-CT exercise. The BDNF serum levels were determined by a biomedical analyst. Upper limb (UL) capacity was quantified by the Action Research Arm Test (ARAT) (Yozbatiran et al., 2008). This is a reliable, valid and responsive instrument for measuring dexterity in the UL following stroke (Platz et al., 2005; van der Lee et al., 2001; Van der Lee et al., 2001).
Secondary outcomes
All measures are reliable, valid and responsive for this cohort of participants with chronic stroke. Upper limb impairment was assessed by the Fugl-Meyer Assessment - Upper Extremity Scale (FMA) according to the standardized procedure (Lundquist & Maribo, 2017). Postural and dynamic balance measured with the Mini BESTest (Godi et al., 2013). Patient-reported post-stroke fatigue measured with the Fatigue Severity Scale (FSS) (Nadarajah et al., 2017). Health Status (EuroQol-5D (EQ-5D)) (Devlin & Brooks, 2017). Patient resource use questionnaire.
Blinding
All outcomes, excluding BDNF serum analysis, were conducted by experienced therapists trained in their use. BDNF serum analysis was conducted by a blinded biomedical analyst. Practical challenges due to implementing and measuring outcomes in a clinical setting, meant that therapist assessments were not consistently blinded. Subjects were not blinded to allocation but were unaware of the study hypotheses.
Measurement timepoints
Figure 1 depicts the measurement timepoints in this study. Primary and secondary clinical outcomes were tested 5-6 days prior to training start (Baseline), 1–3 days after the last training session (Post 12), at 3 months follow-up (FU1), and 6 months follow-up (FU2). Serum BDNF was assessed additionally at 4 and 8 weeks of the intervention to monitor ongoing change in serum basal BDNF as studies in healthy individuals indicate that basal levels of BDNF reduce with increasing fitness (Figueiredo et al., 2019; Knaepen et al., 2010). Cost and HUI data were gathered at baseline, post-intervention (12 weeks), FU1 (3 months) and FU2 (6 months).

Timeline: Measurement timepoints (*only serum BDNF).
Participants fulfilling all criteria who gave informed consent were randomised after baseline assessment using a 1 : 1 allocation into one of the two study arms. Random assignment was perfomed by a clinical administrator using a web-randomization tool (freely available at https://www.randomizer.org/). To ensure concealed allocation the list was kept locked in the main study site. Allocation was revealed by a secretary following enrollment into the study.
Data analysis
Descriptive statistics were calculated for feasibility outcomes and presented as absolute and percentage values of patients screened, found eligible, recruited and randomised, “Drop-outs” and adverse events. Adherence to training was calculated as number of sessions attended as a percentage of maximum possible. Absolute training times in minutes were calculated for each participant and group. All values were compared to the defined criteria for success in order to evaluate feasibility. Clinical outcomes are presented with descriptive statistics (means and standard deviations). Friedmans ANOVA was used to evaluate chronic change in basal BDNF levels across repeated meaurements. The Wilcoxon signed-rank Test was used to evaluate acute change in serum BDNF between pre- and post training.
In order to avoid potential bias created by “Last Observantion Carried Forward” (LOCF) in this small sample (Lachin, 2016; National Research Council Panel on Handling Missing Data in Clinical, 2010), and to show the actual and not predicted effects in this feasibility study, analyses of feasibility and clinical outcomes were conducted based on available data without replacement of missing values (Tripepi et al., 2020).
Percentage of returned cost-effectiveness questions are presented. Partial (COI) and full (Cost-Effectiveness Analysis) HEE as well as (Health Utility Indices) HUI were calculated if appropriate. When HEEs are conducted within randomized trials, costs for individuals with missing data may be systematically different from those with full data sets (Gabrio et al., 2017), therefore missing values in the cost questionnaire were filled in using the median of the last measurement per participant. For missing data in the EQ-5D-5L questionnaire the Last Observation Carried Forward (LOCF) method was used.
The HEE was not described in the initial protocol registration because the decision to collect this data was determined after the inital submission. All participants provided written informed consent before data-collection.
Results
Feasibility outcomes
Screening, recruitment, and randomisation rates
In total 868 patients were screened from the clinical information software of the physiotherapy out-patient department using data from 2003–2018. Due to low eligibility and recruitment rates, seven additional regional clinics were included and 20 further patients were identified using purposive sampling. In these clinics inclusion and exclusion criteria were used by treating physiotherapists to identify potential candidates. 123 of all patients screened or purposively sampled met the inclusion criteria (13.8 % of total). These were telephoned and 79 were contactable. 24 agreed to attend for detailed screening and to obtain informed consent. Of these, 17 patients were enrolled and randomised. This represented 2% of total screened or purposively sampled, 13.8% of eligibles and 21.5% of those eligible and contactable (Fig. 2 and Table 1). Reasons for failing to meet the inclusion criteria included non-stroke diagnosis (the clinical software database included all neurological diagnoses) or prohibited co-morbidities. Eligibles declining to participate included those not willing (due to general lack of motivation or reluctance because of length of the intervention or travel distance), those who were willing but unable (due to employment or other commitments, or practical difficulties), those who were non-contactable. 21.5 % enrollment of all eligible and contactable persons is 3.5% below the 25% defined as the enrollment rate criteria for success.

CONSORT flowchart.
Participant characteristics at baseline
FMA-UE: Fugl-Meyer Assessment - Upper Extremity Scale.
Enrolled participants were randomized, ten into the MI-ET group and seven into the LI-CT group. However, following randomisation three participants asked to transfer study-arm. These participants were all unable to attend the MI-ET group in the early morning due to need of support with self-care and transport difficulties.
The drop-out rate of the MI-ET was 1/10 (10%) at post-intervention (12 weeks) due to one participant who developed pain in the hemiplegic leg during ergometer cycling. This remained unchanged at FU 1 (3 month follow-up). These rates achieved the criteria for success. At FU 2 (6 month follow-up), one further participant dropped out because the measurements were onerous. This drop-out rate was 2/10 (20%) and below the success criteria. In the LI-CT group one participant was randomised but dropped-out before baseline measurements without explanation. Two further participants dropped-out during the intervention, one due to an unrelated illness, the other went travelling, totalling 3/7 (43 %) at post-intervention (12 weeks) which was below the success criteria. At FU 1 (3 month follow-up) there was a further drop-out due to unrelated death 4/7 (57%). At FU 2 (6 month follow-up) there were two more due to onerous measurements totalling 6/7 (85%).
Participant characteristics are presented in Table 1.
The MI-ET group consisted of eight males and two females. Age and time since stroke in years mean (SD) was 60(5) and 11(10) respectively. Five particpants had a left and five a right hemiparesis. The LI-CT group consisted of 5 males and 1 female. Mean (SD) of age and time since stroke in years was 56.6(10.61) and 5.5(1.8). Four participants had a left-sided hemiparesis, two a right-sided. Arm function (mean (SD)) as measured by the Fugl-Meyer Arm Score was 31(15.7) in the MI-ET and 28(14.7) in the LI-CT groups.
Adherence
Figure 3 demonstrates levels of adherence in terms of percentage of total possible sessions attended for each individual participant. Three participants failed to complete 80% of their personal training sessions which was defined as the cut-off for drop-outs. In total (306/360) 85% of all training sessions were completed in the aerobic group which fulfilled the group success criteria and (165/216) 76.3% in the circuit training group below the group success criteria. Cumulatively 471/576 (81.7%) were completed. Figure 4 illustrates training duration in minutes per participant.
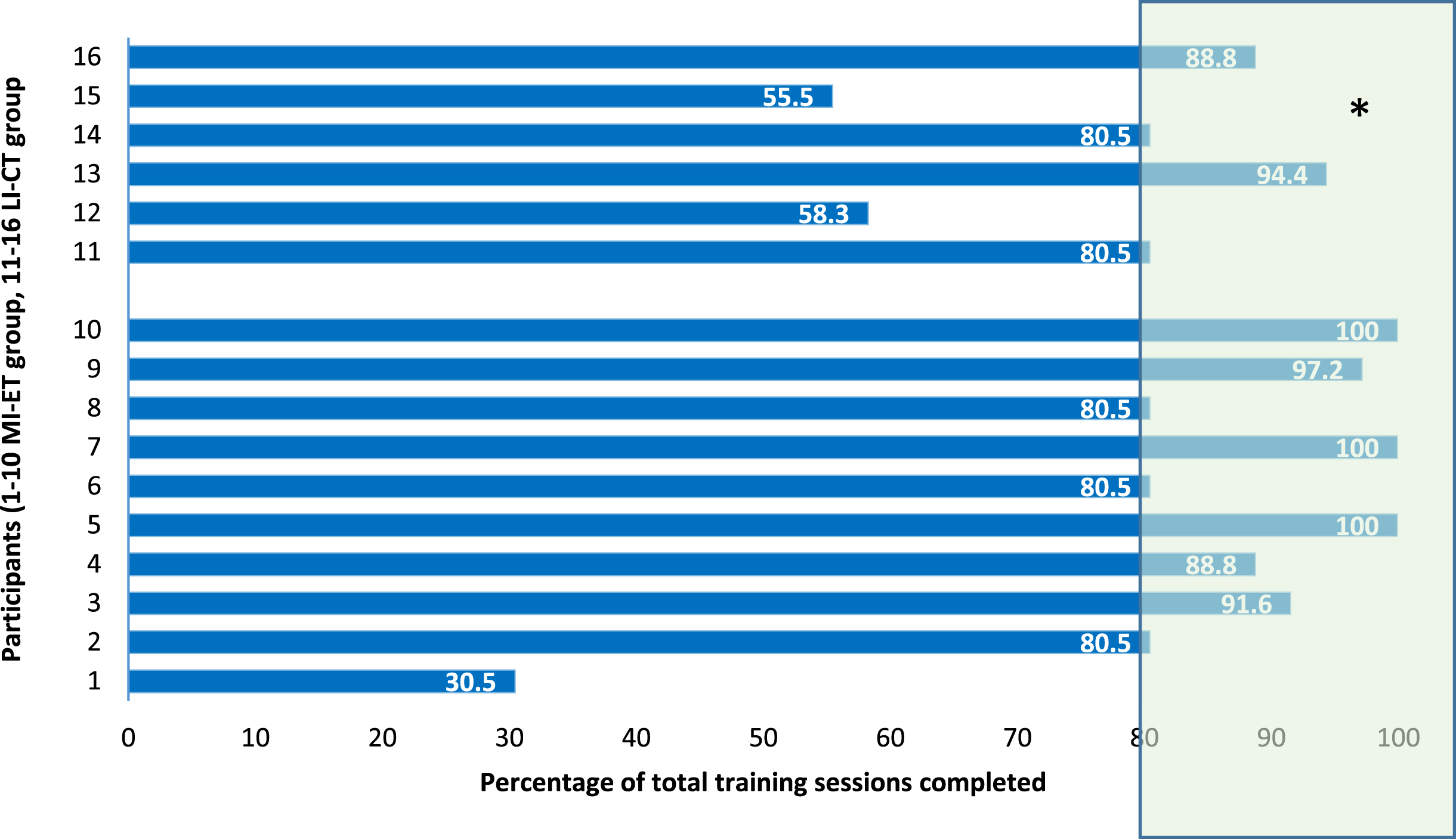
Adherence: percentage of training sessions completed. *shaded area represents training rates of 80% and above defined per protocol as adequate adherence. Training rates < 80% participants considered drop-outs.

Adherence: training duration. Total number of training minutes completed per participant (MI-ET + RT or LI-CT + RT). *shaded area represents training time of 62.5% and above of total possible number of training minutes defined per protocol as feasibility success criteria. § two participants completed 25 minutes at each session as only one ergometer was appropriate for their physical needs and had to be shared.
Seven from sixteen participants (44%) achieved the cut-off number of training minutes (1800 minutes from a possible maximum of 2880). This is below the 75% of participants who must achieve this amount of training in order for the criteria for success to be met.
Eight MI-ET participants completed 40 minutes aerobic training at all sessions attended, two participants completed 25 minutes at each session as only one ergometer was appropriate for their physical needs and had to be shared. All LI-CT participants completed 40 minutes training at the first and all subsequent sessions attended. The mean (SD) duration of aerobic or circuit training over all sessions in minutes from a maximum of 1440 was 1116(300) in the MI-ET group and 1100(230) in the LI-CT group.
The robotic training duration ranged from 12 to 40 minutes per session. The mean(SD) duration of robotic training over all sessions in minutes from a maximum of 1440 was 735.8(287.5) in the MI-ET group and 497.5(287.5) in the LI-CT group.
One participant in the MI-ET group suffered a minor adverse event. Training on the cycle ergometer caused pain in the hemiplegic leg. No further clinical changes were found on examination and no treatment was required. Neuropathic or central pain may have been responsible. The patient dropped out after eleven training sessions. No other adverse events occurred during the training or evaluation sessions. This fulfilled the criteria for success.
HEE
The response rate of cost and EQ-5D-5L questionnaires at baseline was 100% for MI-ET and LI-CT, respectively. At 12-week these rates were 89% for MI-ET and 100% for LI-CT. Rates dropped to 44% for MI-ET and 0% for LI-CT at FU 3 months and to 78% for MI-ET and 80% for LI-CT at FU 6 months (Table 2).
Summary of feasibility outcomes and criteria for success
Summary of feasibility outcomes and criteria for success
Nine from nineteen Criteria for Success were achieved. Based on the interpretation scheme from Thabane (Thabane et al., 2010) this can be classified as feasible with modifications.
In Table 3, the primary clinical outcomes BDNF serum concentrations and ARAT scores are presented. The BDNF serum levels presented are the basal (pre-training) levels. As can be seen in the table, there were no clinically relevant changes in ARAT scores (MCID 5.7) for either the MI-ET or the LI-CT groups. The Wilcoxon Test for pre-post intervention changes showed no statistically significant change, MI-ET p = 0.57, LI-CT p = 0.28. Friedman’s Test for repeated measures indicates that there were no statistically significant changes in chronic, basal (pre-training) values of serum BDNF concentration during the 12-week intervention in either group: MI-ET p = 0.99, LI-CT p = 0.3. Studies indicate that basal levels of BDNF reduce with increasing fitness (Figueiredo et al., 2019; Knaepen et al., 2010). In the MI-ET group there is a continuous but non-significant reduction in basal BDNF concentration during intervention which is not maintained at follow-up. In the LI-CT group this trend is not observed (Fig. 5).
Primary clinical outcomes. Basal BDNF serum concentrations and ARAT scores for MI-ET and LI-CT arms
Primary clinical outcomes. Basal BDNF serum concentrations and ARAT scores for MI-ET and LI-CT arms
Minimal clinical important difference (MCID) for chronic stroke in ARAT 5.7 (van der Lee et al., 2001).

Chronic, basal values of serum BDNF concentrations (mean(SD)) measured during the 12 week intervention at baseline, 4, 8 and 12 weeks in MI-ET and LI-CT arms.
Serum BDNF concentartions showed no statistically significant change from pre to post-training in either the MI-ET or LI-CT arm. BDNF serum concentration pg/mL mean(SD) pre-and post training were: MI-ET 31237(4955.4) and 32408(5464.9), Wilcoxon Test p = 0.10, LI-CT 35329.2(5711.6) and 36824.7(9259.3), Wilcoxen Test p = 0.45. Values in both groups did not vary significantly from BDNF serum concentrations in healthy, age-matched controls (Fig. 6).

BDNF serum concentration of pre- and post moderate intensity aerobic ergometer training (MI-ET) and pre- and post circuit training (LI-CT) Conc pg/mL, [mean(SD)]. Values in healthy, comparable age group illustrated as mean(SD). *BDNF serum concentrations taken from 259 volunteers age in years [mean (SD)] 32690±8330 pg/mL (Naegelin et al., 2018).
Secondary clinical outcomes of MI-ET and LI-CT groups at baseline, 12-weeks post intervention, FU1 and FU2 are presented in Table 4. Fugl-Meyer-UE scores improved, reaching the Minimally Clinical Important Difference (MCID) between pre and post-intervention and was maintained at follow-up. The Mini BESTest improved in the MI-ET group but remained below the MCID. Improvement in the LI-CT group did reach clinical relevance (> 4 points) possibly due to loss to follow-up of subjects with lower scores. Fatigue reduced in both groups following intervention but remained below the MCID. Improvement was maintained in the MI-ET group at FU1 and FU2.
Secondary clinical outcomes
§Minimal detectable change (MDC) 5.2, mininally clinically important difference (MCID) 5.25(Page et al., 2012); *MDC 3.5, MCID 4 (Godi et al., 2013); **Reduction in scores indicates reduced fatigue, MCID 1.9; (Learmonth et al., 2013). Where data is missing the actual N value is given.
Table 5 presents the results of the HUI at baseline, Post 12, FU1 and FU2 for the MI-ET and LI-CT groups respectively.
Health utilities (HUIs) for 1-year for MI-ET and LI-CT groups
Health utilities (HUIs) for 1-year for MI-ET and LI-CT groups
Data analysed including missing values. NA: not possible to calculate due to no data in the control group. HUIs: Health Utilities assessed with EQ-5D-5L with “one” representing the “best health state” and “zero” representing the “worst health state”.
The total costs from a societal perspective of a patient with stroke-related disorders during a retrospective time frame of 1 year were 67,382 (SD 43,107) Swiss-Francs for the MI-ET group and 95,701 (SD 29,473) Swiss-Francs for the LI-CT group.
Table 6 presents direct and indirect costs over a timeframe of 3-months at baseline, Post 12, FU1 and FU2. The total costs of the MI-ET and LI-CT groups differed at baseline, and this difference increased further after treatment and at follow-up, consistently favouring the MI-ET group. Mean of the total and direct costs were calculated for all participants, mean of the indirect costs were calculated and reported only for participants in working age. In this group 90% costs were due to absence from work.
All costs (Swiss-Francs) derived from the resource use questionnaire by group
NA: not possible to calculate due to lack of data in the control group. Data analysed including missing values. Costs due to work absence were not included for mean calculation of indirect costs for retired participants.
The costs from the health insurance perspective (in the canton of Basel-Stadt) was calculated. Forty-five minutes of physiotherapy has a tariff of 77 Swiss-Francs. Both the MI-ET and cost 5544 Swiss-Francs per participant (72 sessions×77 Swiss-Francs). The hospital costs including: average physiotherapy per hour (35 Swiss-Francs), device-use per session (ergometer 3 Swiss-Francs, robotics 38 Swiss-Francs, other 0.30 Swiss-Francs). Device mainteinance and administration costs were not included. The device costs were calculated discounting the total costs over 5 years. Each instrument was used on average 3 time per day. The MI-ET group cost 1328 Swiss-Francs per participant and the LI-CT up 1368 Swiss-Francs per participant.
This study investigated the feasibility of a three month, three times weekly intervention for chronic stroke patients consisting of moderate-intensity aerobic exercise with cycle-ergometry (MI-ET) followed by robotic or sensor-based arm training (RT) or low-intensity circuit training (LI-CT) followed by robotic or sensor-based arm training (RT). A further aim was to investigate the influence of MI-ET and LT-CT training regimes on the immediate and long-term concentrations of serum BDNF and subsequently whether the effectiveness of motor-skills training varies in different BDNF environments.
Nine from nineteen of the pre-defined feasibility criteria for success were achieved, two further criteria closely missed the cut-off, indicating that the protocol is feasible with modifications. The BDNF serum levels did not significantly change immediately following either moderate or low intensity aerobic exercise. Basal (pre-training concentrations) did not change significantly during the intervention or follow-up periods in either group (long-term change) although levels did show consistent non-significant reductions in the MI-ET group. No clinically relevant group changes in arm performance as measured by the ARAT were found in the present cohort, but arm function measured with the Fugl-Meyer-UL assessment, did show clinically relevant changes in both groups.
Feasibility
Recruitment and enrollment were challenging aspects of feasibility. Of 888 patients screened or purposively sampled, 17 were enrolled indicating a recruitment yield of 2%. The difficulty of low recruitment yield in stroke recovery trials has been frequently documented (Ferreira et al., 2019). In this study the screened database included all patients, many of whom did not have a primary diagnosis of stroke, increasing absolute numbers screened. A more targeted strategy of purposive recruitment such as involvement of additional members of the interprofessional team (occupational therapists, nurses, etc.), via the distribution of information leaflets or through contact with patient groups may enable higher yields. Of those patients who were both eligible and contactable approximately one in five agreed to participate, below the pre-defined one in four success criteria. The frequency and length of the intervention was daunting for some patients and impractical for others who had employment or other commitments. As each session lasted for approximately two hours, it may be that shorter more intense sessions, or a shorter more intense intervention periods would be more realistic for some candidates as demonstrated by Ward et al. with a a 3 week, 90 hour intense programme (Ward et al., 2019).
Following study begin, attendance rates were good. The MI-ET group attended 85% of all sessions, above the 80% success criteria level and the LI-CT group 76.3 % slightly below. This indicates that the stategies incorporated into the protocol to support adherence were effective. Participants confirmed that provision of transport and peer-to-peer support gained through group training and a communal snack, were key factors. It was observed, but not formally evaluated, that commaradery developed between group members over the three month programme, manifesting as friendly competition and mutual support during difficult phases. This was the case for both MI-ET and LI-CT groups. Future studies should investigate this phenomena.
The proportion of patients who achieved the cut-off for total minutes trained was 44% which was below the 75% pre-defined success criteria. Time spent in robotic or sensor based arm training was lower than time spent in aerobic or circuit training. This may have been because participants were tired after the preceding training sessions, because training difficulty level was set too high or because the individual training removed group pressure to complete tasks. These factors should be formally evaluated in future studies so that appropriate protocol adaptations can be made to enable high dosed upper limb training times. In the MI-ET group it was unexpected that eight from ten participants would be able to complete 40 minutes of aerobic training at the first session. Based on standardized training protocols (Billinger et al., 2014; Ploughman & Kelly, 2016), we expected time of training to be increased incrementally based on tolerance. It may be that the support of self-efficacy via precieved exertion with the Borg Scale, as well as peer group participation increased motivation and facilitated training time adherence.
Drop-out rates in the MI-ET group were within the pre-defined cut-off at 12 weeks and 3 months (FU1), but did not reach the success criteria for 6 months (FU2). The reluctance to attend for final measurements may have been impacted by unusually hot weather and lack of air conditioning. The proportion of drop-outs in the LI-CT group was higher than the 15% criteria for success at all measurement points. This was partly due to lower group size, meaning that absolute numbers had a higher proportional effect. Three drop-outs were due to unrelated events rather than negative effects of the intervention or training programme. Lack of interest due to participation in the control group, reported as relevant in previous studies, was not a factor in this study (Barker et al., 2016; El-Kotob & Giangregorio, 2018). No participants were aware of the hypotheses and both arms had active interventions. The reason for one drop-out immediately following randomization is unknown. Although randomisation was done following recruitment, some participants were unable to arrive on time for the morning MI-ET group and were switched, after requesting to do so, into the afternoon LI-CT session. This protocol adaptation was allowed as part of the feasibility study and provided an important methodological insight. Future studies, should minimize early morning starts and enable similar intervention times on different days if therapists or equipment is limited.
The factors shown to positively impact exercise adherence in this study provide insights into strategies which could be applied in clinical practice. It is recognised that motivation for patients to participate in stroke rehabilitation may vary and that specific strategies are necessary (Oyake et al., 2020).
The embedded HEE demonstrated high levels of questionnaire return (costs and EQ-5D) at baseline and 12-week post-intervention. This was facilitated by a dedicated person who prepared, sent and actively followed the individual participants. At FU1 (post 3-months) questionnaires were sent by post instead of given by hand during the follow-up measurement. This led to a lower rate of return in both groups. The strategy was changed back at FU2 (post 6-months) so that participants were handed the questionnaires individually where possible, resulting in increased return rate.
Clinical outcomes
Only BDNF measurements were blinded. As the interventions were carried out during normal clinical daily practice, all participating therapists were aware of group allocation. In future, external assessors should be engaged.
Clinical outcomes in this feasibility study demonstrated that serum BDNF concentrations did not increase following moderate-intensity aerobic exercise. Our findings differ from the study by Carvalho de Morais et al. (2018) in which 10 chronic post-stroke participants conducted a single session of moderate intensity walking and showed a statistically significant increase in serum BDNF post training. However, more recent studies have compared the effect of moderate-intensity and high-intensity training on serum BDNF in chronic stroke patients (Boyne et al., 2019; Hsu et al., 2020). These studies conclude that high intensity but not moderate intensity training increases serum BDNF concentration. Boyne P. et al. state that high intensity training is necessary because “a vigorous aerobic intensity sufficient to generate lactate accumulation is needed to increase BDNF”(Boyne et al., 2019) Our results appear to corroborate these findings regarding the acute effect of moderate intensity training on serum BDNF in chronic stroke. In view of these results, future RCTs should compare the effects of high intensity to moderate intensity aerobic training on serum concentration BDNF and potential changes in the efficacy of motor-learning in different BDNF environments post-stroke. The adherence of patients to high-intensity exercise may differ to adherence to moderate-intensity exercise and those excluded due to cardiovascular risk factors may be higher. A “minimum level” of training intensity should be identified to promote change in BDNF concentrations and facilitate maximum patient participation.
Our results also indicate that chronic serum BDNF concentrations in the MI-ET group reduced slightly but non-significantly during the 12 week intervention. Research findings in healthy individuals indicate that basal levels of BDNF reduce with increasing fitness (Figueiredo et al., 2019; Knaepen et al., 2010). As five from nine participants in the MI-ET group increased cardiovascular fitness during the intervention (see supplementary materials), our findings may indicate that a similar physiological change occurs in chronic stroke patients. Larger studies are needed to confirm this trend.
We also found that serum BDNF concentration in chronic stroke patients did not vary significantly from healthy age-matched controls. This result is contrary to the findings of Lopes Santos et al. (2016), who found that the hemiparetic group (17 stroke, 17 healthy participants) presented serum BDNF concentrations 57.27% lower than healthy controls. Our sample of 17 participants, with repeated measurements, was compared to values of 259, healthy, age-matched volunteers (Naegelin et al., 2018) potentially increasing the power of the comparison. Further studies are required to clarify how serum BDNF concentrations in chronic stroke patients compare to values in healthy age-matched controls.
Although there were some individual improvements in arm performance, there were no clinically relevant, group changes pre-post intervention with fine motor control measured by ARAT. This may be due to a lack of statistical power but may also be influenced by an under dosage of therapy time and number of repetitions. Ward et al. (2019) have recently shown that functional improvement of the upper limb in chronic stroke patients can be achieved with high-dose, high-intensity therapy. “90 hours of therapy improves arm function while 32 hours does not” (Cramer, 2019) In our sample the longest time spent arm training was 1282.5 minutes (21.35 hours). This is below the dosage in the provided by Ward et al. Those individuals which did improve completed the most training minutes.
Both groups showed a similar improvement in balance post intervention as measured by the MiniBESTest, which narrowly failed to reach the MCID. These changes were maintained at three and six month follow-up. These finding support results of previous studies which indicate that circuit-training and cardiovascular aerobic training have positive effects on balance (English et al., 2017; Lund et al., 2018).
Based on the findings of this single blind, controlled feasibility study as well as recent research publications (Boyne et al., 2019; Hsu et al., 2020), we conclude that a future RCT should compare the effect of moderate versus high intensity aerobic exercise on serum BDNF levels prior to a higher dosed upper limb training, rather than moderate and low (or zero) aerobic training. It is possible that the numbers of potential stroke patients eligible and willing to participate in high intensity training is lower than the 21% found in this study. A broad, goal oriented recruitment strategy should therefore be defined as part of the study protocol to enable a higher recruitment yield and an adequately powered sample size. A more intense intervention for a shorter period of three to five weeks (Ward et al., 2019) would enable higher intensity training and may facilitate recruitment of some candidates. Treatment should not begin early morning. We recommend training in groups to increase peer-support and the minimization of practical difficulties such as travel arrangements, to increase adherence.
HEE
Because no significant between groups effect size could be observed, a full HEE with cost-effectiveness analysis or cost-utility analysis was not possible. In this case, the HEE reduces to a cost-minimization analysis. However, COI data could be reported. COI of stroke related disorders is not well reported. Therefore, COI results of the present study may serve health economists as input data when modelling HEE or may be used as “eye-opener” for policy makers, who are often not well aware of the economic burden of health problems.
The HUIs calculated with the EQ-5D-5L using the UK tariff (Devlin et al., 2018) was easy to complete and well comparable to other studies (Devlin & Brooks, 2017). The MCID of the EQ-5D-5L for stroke patients undergoing rehabilitation is 0.100 (Chen et al., 2016). The MI-ET group had an improvement of 0.064 at Post12 and 0.089 at FU1, while LI-CT improved at a maximum of 0.033 at Post-12. This could be an indication that the moderate aerobic training led to a better daily quality of life compared to circuit training (Aguiar et al., 2020). Resource use costs were able to capture the economic burden of chronic stroke patients and to demonstrate a difference between the two interventions. The aerobic training combined with robotics-training led to lower costs post intervention and also at follow-up, mostly driven from the lower direct medical costs.
The total costs from a societal perspective of a patient with stroke-related disorders during a retrospective time frame of 1 year were 67,382 (SD 43,107) Swiss-Francs for the MI-ET group and 95,701 (SD 29,473) Swiss-Francs for the LI-CT group. Average costs from a societal perspective of other chronic pathologies in Switzerland in a timeframe of 1-year yield up to 68,078 Swiss-Francs for multiple sclerosis, 50,753 Swiss-Francs for rheumatoid arthritis, 62,000 Swiss-Francs for dementia and 7,748 Swiss-Francs for chronic back pain (Telser et al., 2011).
Collecting the expenses reimbursement documention from each patient’s health insurance would increase the robusteness of such data for a bigger RCT. The method of follow-up contact (Ramsey et al., 2015) was useful and important to reduce missing values and errors due to recall bias.
Conclusions
It remains unclear as to which training parameters are optimal to increase serum BDNF levels in chronic stroke patients and consequently whether motor-training in BDNF-enriched environments increases motor learning due to increased neuroplasticity. This is an important clinical question. If it is possible to increase the efficacy of rehabilitation interventions following stroke, functional outcomes for patients may be increased and health costs could be reduced. With the results of this feasibility study we provide relevant methodological insights for future studies to support enquiry into these clinical questions and to allow the cost-effectiveness of such interventions to be evaluated.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have influenced the work reported in this paper.
Footnotes
Acknowledgments
The authors acknowledge the support of the physiotherapists and sport science staff members of the REHAB Basel and the Bern University of Applied Science (Basel Campus) including Thomas Rosenheck, Lukas Stammler, Alexandra Einert, Tanja di Nicola, Barbara Schürch, Tamara Blosch, Livia Solèr, Christine Hürlimann and Yvonne Glor. Thanks also to Peter Spies of the University of Applied Science of North West Switzerland, Department of Life Sciences.