
Abstract
Introduction
Neurological conditions are inherently complex due to the involvement of a diverse range of impairments, thus the consequences for people with neurological conditions (pwNC) can permeate all aspects of their life and impose significant limitations on their participation in everyday activities [1]. Consequently, neurological conditions are a significant burden and a global health concern [2]. It is estimated that the prevalence of age-related neurological disease in Ireland is expected to rise at a higher rate than other European countries due to our rapidly ageing population [3]. It is projected that there will be a 70% increase in the number of males and 52% increase in the number of females aged 65 years or older living in Ireland from population figures in 2002 to 2021 [4]. This presents a substantial challenge for the Irish health service.
Physiotherapy is an integral part of health service provision for pwNC [3, 5] and is associated with positive rehabilitation outcomes [6–8]. Consequently, it is highly valued among community dwelling pwNC in Ireland [9]. Given the significant burden of neurological conditions for the community dwelling neurological population and the potential of a quality physiotherapy primary care service to alleviate some of this burden, there is a need to ensure that physiotherapy primary care services are delivered at an optimal level.
There is a paucity of literature examining physiotherapy service provision for pwNC in primary care in Ireland. However, it is well recognised that current community and primary care based health services in Ireland for pwNC are inadequate, with many barriers to quality service provision in this population [10–12]. A national survey of people living with a neurological condition in Ireland revealed a dearth of access to physiotherapy and other health services. Furthermore, 34% of those surveyed in 2014 reported that it is was more difficult to access physiotherapy compared to 2011, when the initial national survey was conducted, indicating a perceived worsening of access to physiotherapy [12].
A survey of 632 patients in Ireland with multiple sclerosis, revealed that more than 50% experienced unmet, non-pharmacological needs. Participants who were older, single, in rural settings, those with a greater level of disability and progressive non-relapsing multiple sclerosis were more likely to experience unmet needs, of which physiotherapy was most frequently cited [13].
The national audit of stroke care in Ireland [10] reported community stroke services were inequitable and inadequate with substandard physiotherapy service provision. Poor communication between acute and community settings, lack of an electronic patient database, scarcity of specialist services, limited resources and busy workloads were also identified by Allied Health Professionals (AHPs) as barriers to effective management of people with stroke in the community. Similar findings were reported in a national survey of stroke services provided by AHPs, in primary care in Ireland three years later, where reported barriers to service provision included inadequate therapy durations, facilities, infrastructure and insufficient administrative support [14].
Qualitative studies from the United Kingdom which explored physiotherapists’ perspectives of service provision for pwNC reveal that physiotherapists view neurological conditions as complex, requiring a high level of clinical knowledge [15, 16]. Furthermore, community physiotherapists experience challenges gaining access to specialist neurological training [16, 17]. Sackley and Lincoln [18] found significant occupational issues among physiotherapists who work with stroke patients in meeting managerial targets, addressing patient-centred needs and satisfying their own professional demands. Although this study is of moderate methodological quality, it’s findings are triangulated with similar literature, enhancing its credibility and dependability. A mixed-methods study by Bourne et al. [17] revealed that physiotherapists working with neurological patients experience anxiety due to lengthy waiting lists, lack of specialised training and the extent of their patient caseload. In conjunction with the Irish study by Scott and Keating, this study identified a lack of resources such as physiotherapy staff, administration support, inadequate facilities and time constraints.
The literature indicates that pwNC have complex needs and current service provision in Ireland falls short of delivering on these needs, particularly in the community dwelling neurological population. In addition, barriers such as inadequate resources and lack of support for training create challenges and stress for healthcare professionals. Evaluations of health service provision recognise the value of the health professionals’ perspective in exploring barriers and facilitators of quality service provision [19]. Consequently, this study aims to explore physiotherapists’ views and experiences of physiotherapy service provision for neurological patients in primary care.
Methods
Study design and participants
A qualitative methodology was used to gain an insight into the views and experiences of the participants [20]. The application of a qualitative design for evaluating health services from the perspective of those involved in the service is valued for its strength in exploring and understanding human’s attitudes, experiences and behaviour [21]. Ten semi-structured interviews were conducted. Physiotherapists were eligible for interview if they were currently working in primary care, with at least one years’ experience and treating people with neurological conditions.
Recruitment of ten primary care physiotherapists took place via purposeful sampling which involves the intentional selection of specific participants [22]. Purposive sampling enabled access to participants who fit the inclusion criteria and a geographical spread of participants from various locations in Ireland. Snowball sampling, commonly used in qualitative research, was employed, whereby the researcher identified one participant who fit the inclusion criteria and this participant provided the contact details for other physiotherapists who also agreed to participate. The participants were located in two primary care practices in Co. Cork, one primary care practice in Co. Tipperary and one in Co. Dublin. There were no refusals to participate. No new information emerged from the data of the tenth interview, at which point data saturation was reached [23].
Procedure
The interview schedule was devised according to the aims of the study and was informed by the literature in the area [10, 24]. A pilot interview was conducted with one primary care physiotherapist to aid refinement of the interview schedule in advance of the main study. The physiotherapist who participated in the pilot study was purposively selected and did not participate in the main interviews. Analysis of the pilot study data also enabled the researcher to refine and focus the data analysis process. The semi-structured interview schedule consisted of five pre-set themes which formed open-ended questions. Interviews were conducted with one interviewer (MMD) in a quiet private space in the primary care centre in which the participants worked. All interviews were face- to- face and audio-recorded with prior written consent from the participants. The interviews were transcribed verbatim and, as agreed with the participants at the recruitment stage, respondent validation was sought [25], whereby the participant was asked to verify if the data accurately portrayed what they were trying to say. All participants’ transcripts were assigned a code to ensure anonymity.
Data analysis
Thematic analysis was adopted for analyses of all transcripts [26]. Transcripts were systematically coded involving a line by line analysis of the research transcripts. Codes were then sorted into categories and redefined into further focused categories according to their fit [27]. The categories were considered to be saturated when no additional information was found to develop them further. Category development involved two core criteria; categories were independent of each other and exhaustive [26]. Themes emerged from these categories and all transcripts were then compared and contrasted to aid thematic exploration and the development of theories. Themes were reviewed and refined and a map of themes and sub themes was generated. In this way links were identified among the complex subjective views and experiences of the participants.
Methodological rigour
The credibility of this study’s findings was strengthened by the independent thematic analysis of all transcripts by a second researcher (OAC). The main disagreement arose in relation to the barriers and inhibitory factors to the provision of a quality service. Disagreement was resolved in a consensus meeting in which both the primary and secondary researcher discussed the conflicting data and decided upon a common category system [28]. In addition, the primary researcher completed an initial line by line coding process of each transcript and several days later repeated the process on an uncoded copy of the transcripts, enhancing the dependability of the analyses. The primary researcher (MMD), a physiotherapist with previous experience of working as a primary care physiotherapist engaged in self-reflection throughout the study and made entries into a personal diary after each interview, enabling her to be aware of her own assumptions and biases due to her background as a physiotherapist. This enhanced the neutrality of the study’s findings by taking measures to address potential bias of preconceived perceptions of the participants’ reality.
Participant demographics
Participant demographics
Abbreviations: M = Male, F=Female, MSK = Musculoskeletal, PCCC = Primary Community and Continuing Care.
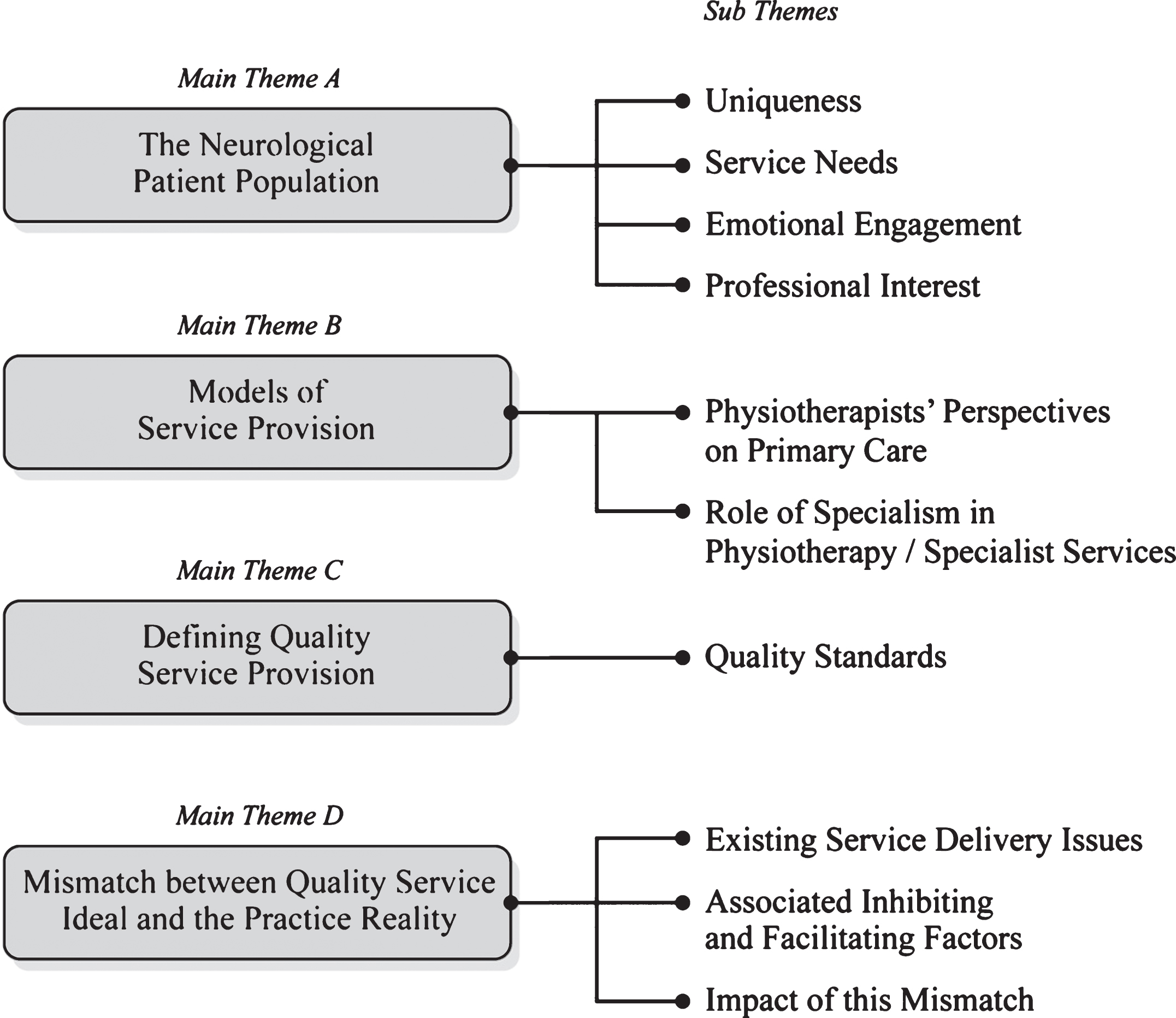
Over-arching themes and sub themes
Ten physiotherapists (nine females and one male) participated in the study. The mean age of the participants was 37 years±6.88 years. One participant had completed a postgraduate course in neurology and three participants had completed post graduate courses in musculoskeletal (MSK) physiotherapy.
Theme A: People with neurological conditions
Results revealed that pwNC are viewed as a unique but diverse patient sub-group with distinct service needs from the general patient population in primary care. The unique characteristics of PwNC include the complexity of their condition, the impact of their condition on their life, the duration of their condition and associated multi-morbidities. This was illustrated by the following sentiments. ‘I think they are battling a more of a long term uphill, em life really’ (P6). ‘They are totally different in that even getting to you can be a challenge’ (P10). In addition, participants expressed that pwNC ‘are a very determined client group (P10) and they are ‘more driven’ (P6) than most in their attitude and commitment to physiotherapy. The participants also revealed that long-term management of pwNC often fosters a close relationship whereby the physiotherapists will become ‘nearly personally involved with them’ (P10). Participants also expressed an emotional engagement with the neurological patient population. ‘The other one as I say that is quite emotive is the likes of Motor Neuron’ (P1). ‘It can be a hard caseload and you would see so many young people getting a diagnosis like a young MS diagnosis’ (P4). The majority of the participants reported a professional interest in working with pwNC. ‘They are a clientele that I really enjoy working with’ (P2).
Theme B: Models of service provision
Participants reported that primary care can effectively manage basic level physiotherapy care for neurological patients but that complex care needs require specialist physiotherapy services to work alongside of primary care in the community. ‘Particularly when you are talking about more complex neurological conditions with more complex needs. I think that a tertiary specialist centre can then have considerations for kind of a more private, em, cubicle so that you know, you’re dealing with a client group where, to try and maximise their dignity and to have that option available to them where they would have increased treatment time as well, wider plinths, wheelchair access, a consideration for that’ (P2).
They also reported that specialist training in neurology is advantageous for all primary care physiotherapists. The specific characteristics of primary care which participants highlight as beneficial included the locality of primary care services, a de-emphasis on acute care, the potential for health promotion, the ability for the patient to develop a rapport with the multi-disciplinary team (MDT) and open access to a full MDT.
Theme C: Defining quality service provision
The quality standards of a primary care physiotherapy service for people with a neurological condition identified by participants included: access, resources, flexibility, collaboration between services, high professional standards and training, MDT work, engagement in health promotion and the development of good relationships between patient and physiotherapist. Access to physiotherapy was identified as the main quality indicator. Access was described in terms of the speed of access, the continuity of access and physical accessibility to the service. ‘It would be accessible, kind of as urgently as needed’ (P4). Easily accessible for those types of patients from the point of view of physical access’ (P9). In addition, the capacity to ‘tailor your treatment’ (P9) so that a ‘needs specific physio service’ (P2) could be delivered was suggested as an important component of this quality service. ‘I think that there really should be provision there for them to be reviewed on a long term basis’ (P4).
Theme D: Mismatch between the quality service ideal and the practice reality
The existing service delivery issues identified by participants include inadequate resources such as inappropriate staffing levels, lack of time, lack of administration support, lack of appropriate infrastructure and equipment for the needs of this patient population. ‘Again you are kind of restrained as to how much you can sort of just, from a staffing point of view, how much input you can actually give, that’s the problem’ (P3). ‘We are on the fifth floor, there is a lift but they’ve to go through some gates with kind of key coding numbers and everything that by the time they get in they’re a little bit stressed by the whole access to the building’ (P9).
Furthermore, the majority of participants reported that there was poor communication and ineffective collaboration between acute care, community based health care organisations and the primary care team. ‘Communication between systems as well, outside of different areas can sometimes be really poor and quite difficult to kind of track down between acute and primary care in particular is an ongoing issue’ (P2).
In addition, poor MDT work within primary care was reported by participants and this was mainly attributed to a lack of buy-in to the primary care team model by GPs. ‘The GPs aren’t attending our primary care meetings. They haven’t been for the last six months… felt like it was a bit of a mockery of what we were trying to achieve when the GPs weren’t attending and we were all attending’ (P6).
The participants identified a lack of organisational support from the Health Service Executive (HSE) as the main inhibiting factor to the provision of a quality service provision. This was reported in relation to a lack of support for training, ‘I think there is an onus on the HSE to do more, possible more neuro training and more regional neuro training where they allow staff to go on training days’ (P1).
There was a perception of managerial pressure to quantify throughput of patients rather than evaluate the quality of service provision. ‘our stats, which doesn’t look at, it doesn’t look at performance, it looks at performance in the sense of numbers but it doesn’t look at the quality of service’ (P9).
In particular participants felt that pressure to reduce waiting lists impacted on the quality of the service in a variety of ways, resulting in a reduction in continuity of care, difficulty in providing sufficient time for neurological patients and restricted time for continuous professional development (CPD). The participants reported that having a manager with a background in physiotherapy and neurology enhanced the managers’ understanding of the service needs and that upper level management who don’t have a physiotherapy background lack this understanding which hinders the delivery of a quality service provision for patients with neurological conditions. ‘They both have a neuro background so we’re very lucky with that but I think other managers ... have no comprehension of how complex it is’ (P10).
All participants revealed how knowledge exchange and the skill mix of the physiotherapy team in primary care was used to address challenges around managing complex cases and that physiotherapy peer support facilitated their attempts to provide a quality physiotherapy service in primary care, ‘Great peer support...makes a big difference’ (P10). Line manager support was identified by half of the participants as a facilitator in terms of supporting professional autonomy, maintaining service flexibility, supporting training needs and sanctioning resources as needed.
The participants acknowledged that neurological patients were receiving a basic level of service, fragmented care and a lack of communication from the MDT. ‘At the minute we provide a bit of an ad-hoc service to be honest that is really what it’s at the minute and obviously that’s not great’ (P3). ‘They really need to be reviewed and just the capacity for review is really not there in a lot of primary care centres’ (P5).
Participants described their frustration in their attempts to deliver a quality service in the face of limited resources and organisational pressure. Participants detailed the ‘constant pressure to get patients through the door and keep waiting lists down’ (P10) and stated that ‘in an ideal world they would have more input more regularly’ (P9).
Issues around discharge were emotive for the therapist in primary care as they view themselves as the last point of contact in these patients care. ‘We’re the end of the line, and when you discharge people it was actually a very hard thing to do for a lot of people who’d have months and months of rehab and then they came out to us and we were discharging them so they really felt they were being left off’ (P10).
Discussion
Participants viewed the management of pwNC as complex and patient-centered care was identified as the core quality standard for physiotherapy service provision. All the quality standards, including resources and access, identified by the participants concur with national and international literature examining quality service provision for pwNC [1–3, 29].
The participants identified substantial challenges to providing a quality physiotherapy service for pwNC in primary care. Extensive service limitations were highlighted including an inability to dedicate sufficient time to the management of pwNC. Neurological conditions were identified as complex to manage and participants highlighted that pwNC required longer than average primary care appointment times to carry out an effective assessment and treatment. However, similar to other study findings [10, 24], participants experienced time constraints. Participants also highlighted limitations in physical access to their primary care physiotherapy departments due to poor infrastructural planning. Insufficient administration and inadequate physiotherapy staffing levels were reported by participants resulting in a reduced quality service for pwNC and their engagement in health promotion activities.
It is well recognised in the literature that effective primary care teamwork results in improved outcomes for pwNC [5, 30]. Inefficiency of primary care teams was previously reported in a study of primary care services in Ireland [14]. The participants in this study highlighted the lack of primary care team meetings and poor communication between the primary care team and acute services as significant barriers to the provision of a high quality service for pwNC.
Many of the service deficits for neurological patients in primary care reported in this study have implications for other patient populations such as those with disabilities, chronic conditions and multimorbidities and this is substantiated in the literature [31–33]. This reveals a significant, more far-reaching issue with unmet needs in existing primary care services in Ireland and highlights the need for flexibility and a patient-centred approach, with sufficient resource provision to facilitate patients with complex care needs.
The participants in this study attributed responsibility for the deficits in quality physiotherapy service provision for neurological conditions with the Health Service Executive (HSE) and its management structures. The HSE was identified as being accountable for a lack of implementation of specialist neurological services, insufficient support for specialist training, inadequate allocation of resources, the development of primary care infrastructure without prior consultation and a lack of supportive strategies to improve multi-disciplinary teamwork and communication between acute and community services. In particular, lack of organisational support and allocated time for training from the HSE were reported as significant barriers to acquiring specialist training in the area of neurology, despite international recommendations for specialist training for all primary care service providers involved in the care of pwNC [2]. In addition, participants expressed frustration at the current method of monitoring physiotherapy services in primary care based upon quantity not quality. This was also reported in a study of physiotherapy management of people with stroke in the UK [17]. This is a significant finding because a lack of measurement of the effectiveness and quality of treatments and patient outcomes reduces the prioritisation of quality outcomes from the top-down.
In addition to the implications of service limitations for patients, this study identified significant implications for the physiotherapists themselves. Occupational stress was consistently reported by participants, mainly related to the imposed limitations on physiotherapy services and a lack of professional autonomy. The theoretical concept of moral distress ‘when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action’ [34] may be applied to 30% of physiotherapists in this study. This was illustrated by participants when they expressed a professional desire to continue to treat a patient with a neurological condition but were unable to do so due to time constraints. Similar research [17] discovered that physiotherapists expressed personal conflict when discharging stroke patients due to waiting list constraints as opposed to when they felt the time was right to discharge in a professional context. Moreover, participants reported that, as a result of the professional relationships developed with pwNC, they become emotionally engaged in their progress, instilling a desire to ensure a high quality service and an inability to do so further compounds their occupational stress.
Study strengths and limitations
It is acknowledged that there is a wide variety of contexts in which physiotherapists in primary care work, therefore the findings in this study are not transferrable or applicable to all physiotherapists working in primary care in Ireland. Nonetheless, this study is of sound methodological quality, is triangulated by similar findings in quantitative studies in the area and it reveals in-depth, credible views and experiences of participants working with pwNC across four primary care sites in the South and Dublin-Mid Leinster regions of Ireland. This study captures trustworthy and dependable findings in the context of localised primary care settings and contributes valuable qualitative data to the current evidence in this field.
Implications for research and practice
Future research which examines this subject with enhanced national representation will prove valuable. In addition, qualitative research exploring the perspectives of patients and managers in the primary care setting will provide a more comprehensive insight into the service needs of pwNC in primary care settings and how current service limitations can be addressed. The scale of the challenge to improve physiotherapy service provision for people with neurological conditions in primary care in Ireland is extensive and requires a multi-faceted approach. Firstly, the lack of organisational support from the Health Service Executive needs to be addressed. Physiotherapists require support from management to enable them to deliver a high quality service to pwNC. This includes increased funding for resources, measuring quality service provision as opposed to throughput of patients and investment in MDT work and collaboration between acute and community services. Secondly, support structures such as physiotherapy team work and line management support need to be promoted and facilitated. This can be achieved by ensuring that physiotherapists in primary care work as part of physiotherapy teams and have regular opportunity for case-reviews, in-services and service reviews with their peers and line managers. Thirdly, the development of centres for the advancement of inter-professional learning, as established in the United Kingdom [35], would be a model worth adopting in Ireland to promote more effective collaboration in primary care and across services. Finally, the increasing prevalence of neurological and chronic conditions in Ireland and the associated public health challenges require the implementation of a chronic care model and a focus on health promotion and preventative activities in primary care.
Conclusion
This study provides a unique insight into the role of physiotherapy in a primary care setting for people with neurological conditions. Previous research has highlighted the inadequacy of service provision for neurological patients in the community and this study demonstrates this within the context of the primary care setting in Ireland. In addition, the theoretical concept of moral distress experienced by these physiotherapists is an original finding in this context and the implications are that the physiotherapists’ perspectives are significant not only in terms of neurological patient outcomes but also for the individual physiotherapist themselves.
Conflict of interest
None of the authors have any conflict of interest.
Funding
None.
Ethical approval
Ethical approval was obtained from the Royal College of Surgeons in Ireland’s (RCSI) Research Ethics Committee. Reference number: REC857.