
Abstract
PURPOSE:
There is limited evidence to guide the delivery of rehabilitation during ward-based recovery post intensive care (ICU). The aim of this study was to explore the feasibility of augmenting usual care physiotherapy with the REhabilitation after Critical illness Assisted discharge Pack (RECAP) in the initial 3 weeks after ICU discharge and to explore the feasibility of conducting a fully powered RECAP trial.
METHODS:
Twenty patients with an ICU stay greater than 4 days and referred to physiotherapy were randomized to receive usual care or usual care plus RECAP. The Functional Independence Measure (FIM) and State Anxiety Inventory (SAI) were used to measure physical and psychological function respectively, with blinded assessments completed at weeks 1 and 3 after ICU discharge. Patient satisfaction with rehabilitation was explored with a short questionnaire.
RESULTS:
A recruitment rate of 72% (21/29 eligible patients) was observed. The intervention was successfully delivered to n = 8 patients with a median of 4.0 (IRQ 2.0–4.0) sessions. 45% of study participants were discharged before the study endpoint. The intervention group reported higher satisfaction scores (44.5/50 +/–5.9 vs 42.8/50 +/–7.6). No adverse events were reported. Intervention delivery appeared feasible and aspects to further enhance the intervention were identified.
CONCLUSION:
RECAP is a short, safe intervention to deliver in combination with ward-based rehabilitation after ICU discharge. Further research is required to optimise RECAP before exploring any effects on physical or psychological function. Methods to overcome challenges to conducting future trials, including defining standards of usual care and choice of appropriate outcome measure could be further explored.
Keywords
Introduction
A significant number of patients who survive an episode of critical illness have persistent physical and psychological problems [1–3]. Return to pre-illness function is not guaranteed resulting in substantial quality of life consequences [4, 5]. Transitioning from ICU to the general ward is one of the most stressful experiences for ICU survivors [6], associated with feelings of vulnerability [7], anxiety, relocation stress and depression [8]. Structured critical illness rehabilitation pathways which have been recommended by National Institute for Clinical Excellence (NICE) are lacking, with only 27% of organizations in a UK survey offering follow-up services and 85% of these were provided after hospital discharge [9].
Evidence identifying effective physiotherapy interventions during ward-based care is limited. To date, studies investigating physical rehabilitation based interventions during the ward-based phase alone [10, 11], or across the continuum of care [12, 13], have demonstrated limited benefit on recovery of physical function of ICU survivors. Interestingly, a recently published qualitative analysis of patient experience of increased ward-based rehabilitation [14] found that although the increased rehabilitation did not improve physical function, the intervention was associated with improved patient satisfaction and perceived quality of care. Providing ICU survivors with a self-directed rehabilitation manual, detailing general information on ICU recovery, a self-directed exercise programme and a diary, supported with follow up phone calls after hospital discharge, improved physical function outcomes at 3 month follow up [15]. Information delivery as a key principle of care is endorsed in the NICE guideline [16] but to date this has mostly not been included in practice [9].
Research from qualitative studies emphasises that patients prefer information to be delivered by someone with ICU expertise and that verbal information is reinforced with written material [17]. Patients recovering from critical illness express a need to know when they are making progress [18–20]. Difficulties with recall and concentration in this patient group can challenge effective information delivery [21]. Goal setting, as a key concept in any rehabilitation strategy, is shown to have a major impact on the relationship between patient and professional, with the availability of professional time and expertise key to successful outcome [22]. Setting rehabilitation goals is also a key recommendation of the NICE guidelines [16]. Self-efficacy, as a feature of effective goal setting, is reported as influencing positive outcomes on pain, disability and quality of life in patients after acute injury [23]. Goal setting as a key feature in the rehabilitation process during the transition from ICU to ward-based care may be of benefit in post critical care rehabilitation, but to date, this has not been studied. The Rehabilitation after critical illness assisted discharge pack (RECAP) was developed as a brief intervention to help implement this evidence into clinical practice. RECAP was designed to support patients during their ward based recovery after ICU by delivering information on individual ICU experience, reinforcing goals of physiotherapy and providing opportunity for patients to discuss their ICU and rehabilitation experiences.
The aim of this study was to explore the feasibility of conducting a randomized controlled trial (RCT) to compare the addition of RECAP to usual ward based physiotherapy with usual care in patients after ICU. Additional objectives were to assess the study recruitment and retention rates; assess the safety of the intervention and study procedures and examine any change in physical and psychological function of patients in the first three weeks after ICU discharge.
Methodology
Study design
The study design is reported according to the Consort checklist for reporting RCTs (Supplement 1) and the intervention reported according to the TIDieR checklist (Supplement 2). The trial protocol has previously been published [24]. An assessor-blinded, single centre pilot randomized controlled trial was conducted in St. Vincent’s University Hospital (SVUH), Dublin, an academic teaching hospital caring for adult patients. The ethics committee at SVUH approved the study. All patients admitted to ICU for 4 days or more with an indication for physiotherapy intervention after ICU discharge (supplement 3) were screened for eligibility. A length of stay of 4 days was chosen based on local data at the study site, where median length of stay in the ICU was 3.7 days. The flow of study design including inclusion and exclusion criteria is outlined in Fig. 1. Once patients were deemed appropriate for discharge from ICU, eligible patients were approached for recruitment by a designated screening therapist who was not involved in intervention delivery. Patients provided written informed consent.
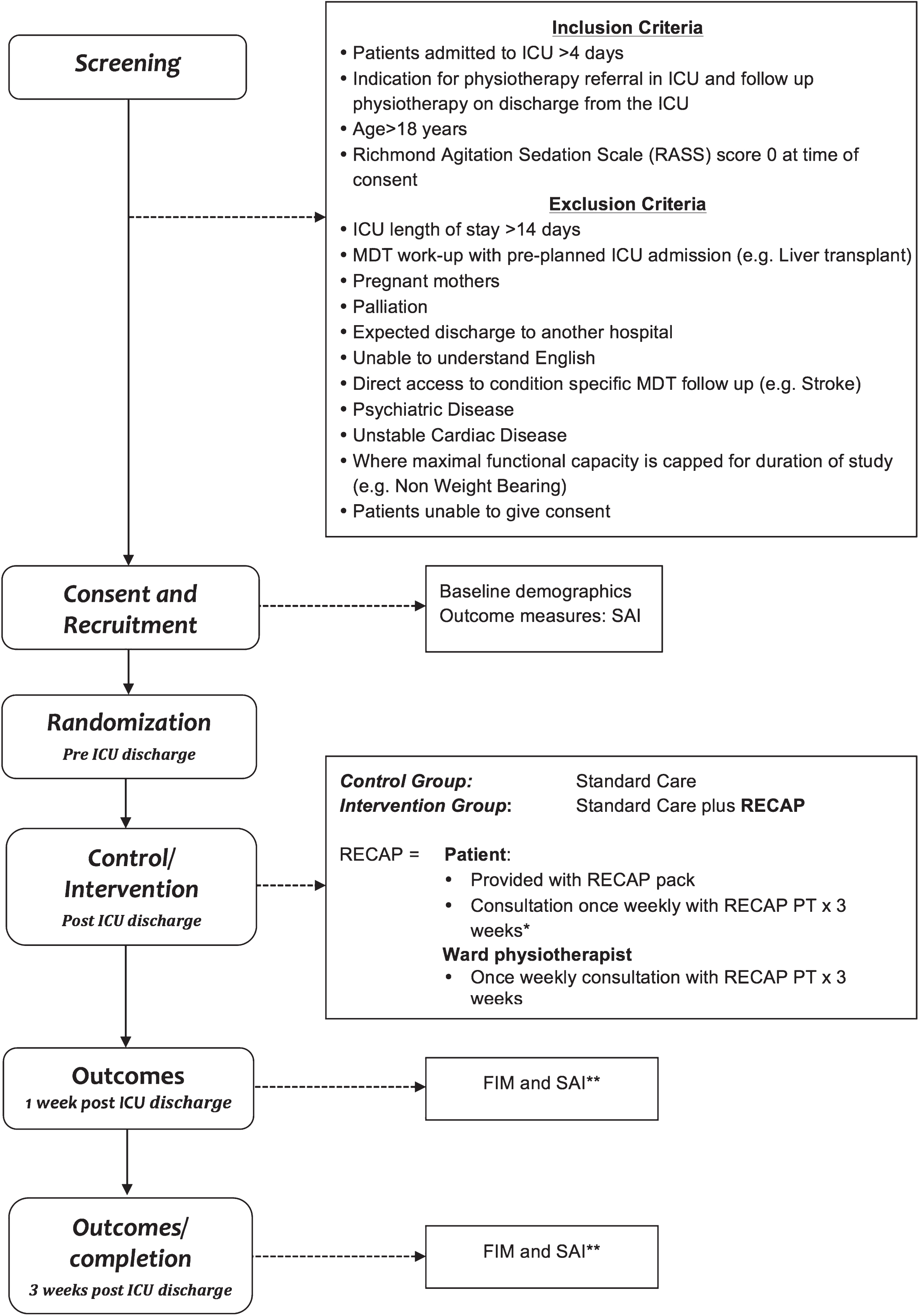
Flow diagram of study procedures. *When discharge from hospital occurred before the study endpoint RECAP delivery was via telephone. **When discharge from hospital occurred before the study endpoint outcome measures were completed via telephone.
Before the start of the trial, a computer generated randomisation list with 1 : 1 group allocation was independently prepared at Ulster University. Treatment allocation was completed independent of the research team. Full details of randomization procedures are outlined in Supplement 4.
Intervention
Patients randomized to both the control group and the intervention groups received usual physiotherapy care. This generally consisted of one to one individualised physiotherapy, delivered by the relevant ward physiotherapist (Supplement 3). Patients randomized to the intervention group received usual physiotherapy care plus the “Rehabilitation after critical care assisted discharge pack“(RECAP) (Supplement 5). The RECAP included:
Part 1: User centred critical care discharge information pack (UCCDIP)
The UCCDIP is an individualised summary of a patient’s critical care experience. It has previously been described in the literature [25] and was used with the author’s permission.
Part 2: A rehabilitation goal setting care plan
This section includes a lay summary to explain why rehabilitation is necessary and what to expect from physiotherapy. Three rehabilitation progress plans are included, one for completion at each weekly RECAP consultation. Each plan includes a summary of current functional status, including potential reasons limiting this (e.g. impairments). Goal setting is discussed with the patient in relation to goal attainment in the previous week, potential reasons if goals were not achieved and planned goals for the coming week. Activities that the patient can complete to help achieve goals (e.g. exercise programmes) are also discussed.
Part 3: A patient communication forum
If patients had questions or concerns about their care, they could note them in this section, to prompt discussion during RECAP consultations.
Part 4: Useful supports and contact information
This section provided information for patients/families about how to access ICU rehabilitation specific websites, charities and support services.
Part 5: Tailored exercise programme
Individualised exercise programmes could be inserted in this section if these were provided as part of usual care.
Part 1 of the RECAP was completed by the RECAP therapist (MG) (a senior physiotherapist in critical care) once a patient had been discharged from ICU. Patients were provided with their RECAP pack during an initial consultation with the RECAP therapist. This consultation occurred on either the day of ICU discharge or on day 1 after ICU discharge, during which Part 1 was specifically discussed, as were the patient’s current goals of rehabilitation (those set as part of usual care physiotherapy). Part 2 was delivered at each weekly consultation and patient’s were introduced to Parts 3–5 of the RECAP and informed that these could be completed at any stage during the 3-week intervention. Follow up consultations occurred once weekly for three weeks. If discharged from hospital before the study endpoint, patients were contacted by telephone to complete their consultations. During RECAP consultations, rehabilitation progress and goals set as part of usual care were discussed and reinforced. Part 2 of the RECAP was completed based on this discussion. The RECAP therapist also met with ward physiotherapists once weekly to provide clinical support if necessary, in determining the physiotherapy management of the patient post critical care. A consultation log, describing the content, recommendations, actions and duration of the consultation was retained by the RECAP therapist.
Measurements
Demographic information was collected from patient records and included age, ICU length of stay, baseline mobility, ICU supportive therapies and physical function. The Chelsea Critical Care Physical Assessment Tool (CPAx) [29] was used to measure baseline physical function prior to discharge from ICU to facilitate comparison of physical function in both groups at the point of ICU discharge.
The study used two key outcome measures of physical and psychological function. Physical function was measured using the Functional Independence Measure (FIM), a widely accepted, valid and reliable functional assessment, indicating the assistance required for an individual to complete activities of daily living [26, 27]. Formal training and certification is required to administer the FIM. This was provided prior to commencing the study. Psychological function was measured using the State Anxiety Inventory (SAI), a subscale of Spielbergers State Trait Anxiety Inventory [28]. It is a 20-item self-reported questionnaire designed to evaluate the degree of anxiety present in the moment. The license to administer the SAI was obtained prior to study commencement from Mindgarden Inc. At study completion, patients completed five questions on a patient satisfaction questionnaire regarding their rehabilitation experience after ICU (Supplement 6). This was designed for specific use in this study.
Outcome measurements were taken prior to ICU discharge (SAI), at 1-week post ICU discharge (SAI/FIM) and at 3 weeks post ICU discharge (SAI/FIM/patient satisfaction questionnaire). If patients were discharged from hospital before the 3-week endpoint for measurement, final assessments were completed via telephone interview. Due to the nature of the intervention, participant blinding was not feasible. Therapists completing outcome measures were blinded to the intervention received. Allocation was concealed.
Statistical approach
A sample of 20 patients was chosen for this pilot study. All data was analysed in the intention to treat analysis set: all participants randomised, who had at least one assessment measurement. Measures of feasibility were analysed using descriptive statistics. Outcomes of physical and psychological function change over time were analysed using a linear mixed effects model, including time, group, and time*group interaction terms. Non-Normally distributed measures were compared with the non-parametric Mann Whitney U test, or with a mixed model following appropriate transformation. Pearson product-moment correlation coefficients were calculated between physical function measures.
Results
Population
There were 142 patients screened for eligibility during the 6 months between November 18th 2014 and May 6th 2015 (Fig. 2). 20% of all patients screened were eligible for recruitment (29/142 patients screened). A recruitment rate of 72% (21/29 eligible patients) and randomization rate of 69% (20/29 eligible patients) was observed. Six eligible patients (4.2%) were discharged from ICU outside of the screening period i.e. core physiotherapy hours (Monday-Friday) and as a result they were missed in recruitment. One participant completed recruitment but was discharged to another hospital prior to randomization in the study. Patients were excluded mainly due to ICU length of stay more than 14 days (18.3%), unable to provide consent (13.4%), psychiatric disease (8.5%), and functional capacity capped (7.7%), (Fig. 2).
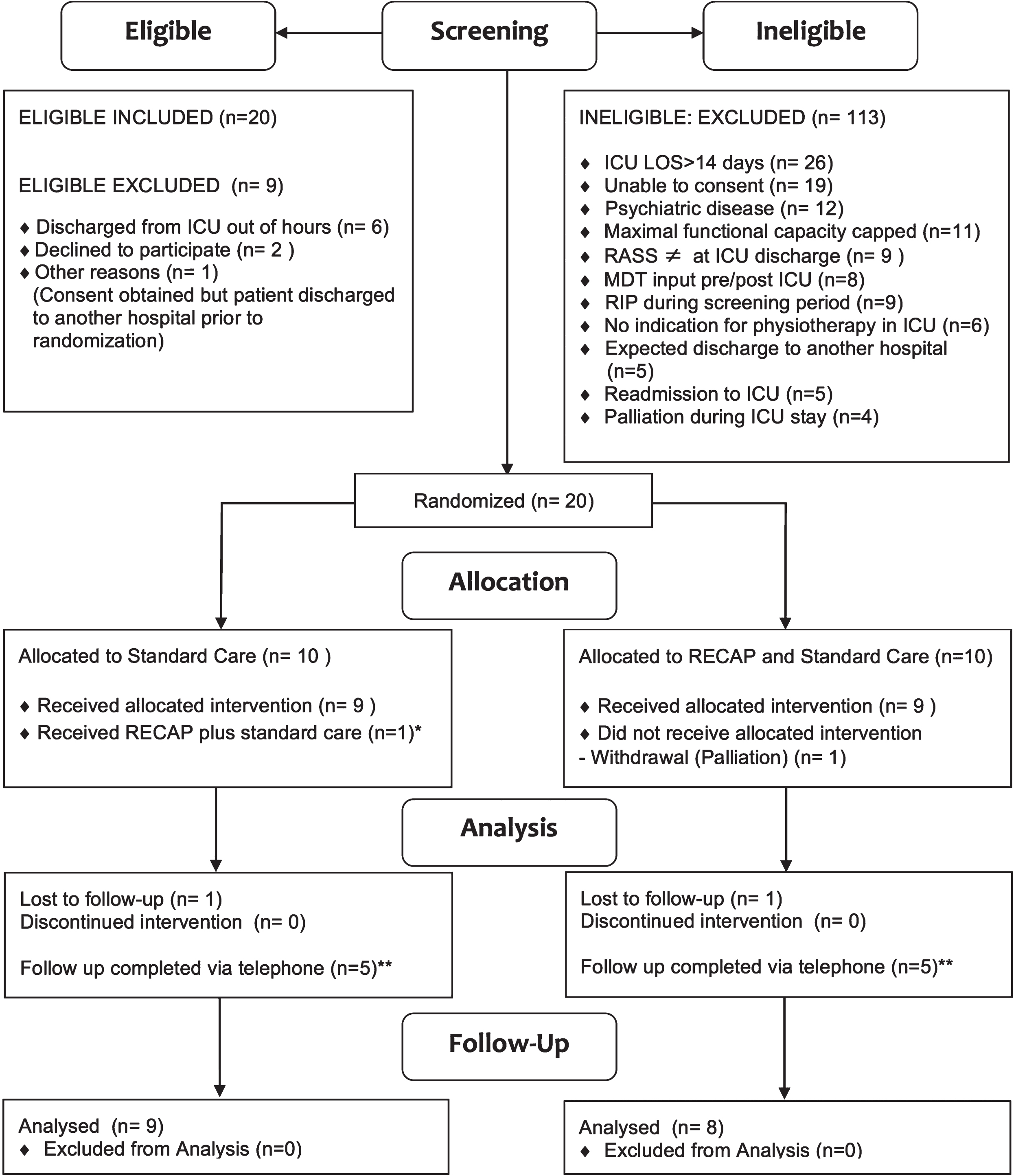
Diagram of study flow. *Protocol deviation due to randomization error. **Follow up completed by telephone interview where hospital discharge occurred prior to study endpoint.
Baseline demographics, length of stay and discharge data for the 20 patients who were recruited are outlined in Table 1. There were no significant differences between groups in the total ICU length of stay (p = 0.247), in the number (p = 0.579) or duration (p = 0.739) of ICU physiotherapy sessions or in the length of stay post-ICU (p = 0.400). In both groups 80% were discharged directly home from hospital. Of note, 45% (n = 9/20) were discharged home prior to completion of the anticipated study period (intervention n = 3, control n = 6) and where possible they were followed up by telephone (Fig. 2); 20% (n = 4/20) of these patients scored the maximum FIM scores of 140 (n = 3) or 139 (n = 1) at their baseline measurement.
Baseline demographics
SD: Standard Deviation, IQR: interquartile Range, ICU: Intensive Care, LOS: length of stay, RIP: Died during study, CPAX: Chelsea Critical Care Assessment Tool: Range 0–50 (0-dependence 50- independence). CRRT: Continuous Renal Replacement Therapy. Baseline physical function was determined through self-report; 100% of the cohort described a baseline of independent and were subdivided based on whether that independence required the use of an assistive device for mobility.
Table 2 provides an overview of the frequency and duration of usual care delivery for both groups. Ten patients were randomized to each group and an attention to treat analysis applied for data analysis. One participant in the control group did not receive the allocated intervention as intended and received the RECAP intervention in error. One participant in the intervention group was withdrawn from the study due to an unexpected change in status due to palliation. One participant was not medically appropriate to complete week two and week three consultations due to neurological deterioration. Three intervention group patients were discharged home prior to study endpoint, of which two completed follow up RECAP interventions by telephone; the third was lost to follow up after hospital discharge.
Summary of standard care physiotherapy and LOS post ICU
Summary of standard care physiotherapy and LOS post ICU
ICU: Intensive Care, LOS: length of stay, PT: Physiotherapy, IQR: Interquartile range. **frequency/time adjusted for number of active in-patient study days.
The intervention was successfully delivered to 8/11 patients (7 intervention group participants and 1 control group patient). Patients received a median of 4.0 RECAP consultations (2.0–4.0 IQR). The median cumulative duration of RECAP consultations across the study was 67 minutes per patient (IQR 8.75–82.5 minutes) i.e. about 17 minutes per consultation on average. Not all of the 5 components of the RECAP were utilised for all patients (Table 3). The UCCDIP (Part 1 of the RECAP) was provided to all of the intervention patients, while the communication forum (Part 3) was utilised by only one participant. The frequency of consultation between the RECAP therapist and the ward therapist about their patient was 3.0 (1.75–3.0); clinical reasoning, discharge planning and goal setting were the most frequently discussed topics within these consultations. A summary of the delivery and content of the RECAP intervention delivery is outlined in Table 3.
Components of RECAP intervention delivered
IQR: Interquartile range, MDT: multidisciplinary team, MSW: medical social work, OT: Occupational Therapy, PT: Physiotherapy, RECAP: Rehabilitation after critical illness assisted discharge pack, UCCDIP: User Centred Critical Care Discharge Information Pack. $Median (interquartile range).
Outcome measure scores for both groups are outlined in Table 4. Measurement of physical function (FIM) demonstrated similar patterns of improvement in both groups. The group difference in the FIM and change in the FIM over time was investigated using a linear mixed model on the ranked FIM values, in order to account for the correlations across time-points of the measure. The results indicated significant change over time (p < 0.001), and non-significant group differences (p = 0.080). There was no difference in the change between groups (p = 0.861). There were also no significant differences between the FIM scores at any time point. The FIM mean difference (95% CI) between groups was –20.4 (–47.7, 6.9) at week one and 20.8 (–46.6, 5.1) at week 3. The model for SAI indicated significant change over time (p = 0.015) and between groups (p = 0.038). While baseline SAI measures were significantly higher in the intervention group than the control group (p = 0.054, 95% CI), the decrease over time was more accentuated in the intervention group, but not significantly (p = 0.075). The SAI mean difference between groups was 13.3 (–0.3, 26.9) at baseline, 17.6 (3.0, 32.2) at week 1 and 9.2 (–1.8, 20.1) at week 3. The Rehabilitation Satisfaction questionnaire showed slightly lower scores in the control group (lower satisfaction by approximately 2 points), but not statistically significant. Correlations over the three weeks were modest with the FIM (Pearson r = 0.36), and considerably higher with the SAI (r = 0.7 to 0.9 over week 1; 0.6 to 0.86 week 1 to 3; 0.67 between ICU and week 3). No adverse events were reported during the study period.
Outcome measure scores at baseline, week one and week three post ICU discharge (*calculated using t-test analysis)
Outcome measure scores at baseline, week one and week three post ICU discharge (*calculated using t-test analysis)
Data is presented as Mean (Standard deviation). Difference refers to the mean difference between groups at each time point and its 95% confidence interval. FIM: Functional Independence Measure Range 20–140 (20 = complete dependence 140 = complete independence). SAI: State Anxiety Inventory: Range 20–80 (20: no anxiety, 80 high anxiety level, score >39 = cut off state anxiety), RSQ: Rehabilitation Satisfaction Questionnaire Range 0–50 (0 = not satisfied, 50 = fully satisfied).
There is very little research on the effects of ward-based rehabilitation in patients after critical illness. This study aimed to explore the feasibility of conducting a RCT to compare the addition of RECAP to usual ward based physiotherapy versus usual ward based physiotherapy alone in patients after ICU. In general while it appeared safe to conduct this small study, challenges to conducting a full RCT particularly relate to e.g. (i) the need for a definition and evidenced based guidelines for minimum standards for usual care, (ii) identification of the essential components of the RECAP intervention that are deemed additional to usual care, (iii) a greater capacity to identify those most in need of additional rehabilitation post ICU, (iv) the variability in timing of discharge from hospital and (iv) the challenge of choosing an appropriate, outcome measure that may capture any effect from goal setting and information provision in this population, at this stage of recovery.
Population and recruitment
Heterogeneity of patients after critical illness has been previously noted to challenge delivery and evaluation of rehabilitation interventions [29]. Inclusion and exclusion criteria applied in this study resulted in a reasonably homogenous cohort. The recruitment rate compares well to a recent ward-based study in patients post ICU [11]. In this current pilot, recruitment may have been influenced by the need for appropriate cognitive function base to allow for active participation in the RECAP intervention and a RASS score of zero at recruitment. All patients in this RCT were stepping and transferring to a chair at ICU discharge based on CPAx scores (Table 1). This may suggest that although patients had impaired physical function, they represent a high functioning cohort of critically ill patients, who were cognitively appropriate to engage with the goal-focused intervention on the ward. In addition, a large proportion of patients were excluded based on having an ICU length of stay greater than 14 days (18.3%) or pre-existing psychiatric disease (8.5%) and in future trials exclusion of these patients may not be warranted.
A number of patients in this study (20%) had independent physical function within one week after ICU discharge and this may indicate not all patients post critical illness have the same rehabilitation needs. The trajectory of recovery for patients post critical illness is not yet known. Factors that determine those most in need of rehabilitation have not yet been identified. Further research to identify those most in need of rehabilitation post ICU is warranted to guide inclusion/exclusion criteria for future trials evaluating the RECAP.
Intervention
Overall, eight patients (73%) randomised to the intervention group completed all of the weekly RECAP consultations. Almost all of these patients received Part 1 (ICU summary) and Part 2 (rehabilitation goal setting) of the RECAP intervention. When delivering Part 2, many patients were unclear about their goals of rehabilitation and concerned about their capacity to manage upon discharge. Although patients discussed concerns at length during consultations, it is interesting to note that only one participant chose to write anything in the communication section (i.e. Part 3) as instructed and perhaps they should be better supported to record this information e.g. by family members or therapy staff. Part 4 was provided to all patients as a standardized list of useful contacts. Part 5 was completed for 6 of the 11 patients and consisted of individualised exercise programmes. It is unclear if the remaining 5 patients needed a written exercise programme. However, considering the low frequency of physiotherapy intervention (Table 2) and the challenges with memory and recall in this patient population [21], it may have been challenging for these patients to independently complete tasks or exercises as part of their therapy programme outside of one to one physiotherapy sessions. Furthermore, considering the high level of function within the study cohort, exercise programmes may not have been clinically indicated.
For the physiotherapists delivering usual care to patients in the intervention group, the main areas where they required support from and/or discussion with the RECAP physiotherapist were clinical reasoning, goal setting and initiation of discharge planning. This suggests that future training for non-ICU experienced physiotherapists providing rehabilitation to this specific population, could focus on these areas to optimise therapist skills in supporting patients to move through the transition from ward care to hospital discharge. Enhanced opportunities for ward staff to link with the specialised critical care multidisciplinary teams may also be important [6, 33].
The RECAP is, in design, aimed to support patients across the ICU to ward transition. A high proportion of patients were unexpectedly discharged home prior to study completion. This was not an anticipated feature of the study design. As a result, supportive preparation could not be provided as planned and, in some cases two of three potential RECAP consultations had to be delivered by telephone after hospital discharge. This impacted on the fidelity of the intervention and presents a challenge for the delivery of interventions during this phase of recovery and for future research studies.
Control
Reporting on usual care is important to accurately interpret study results. Overall, the frequency of usual care delivered to both groups in this study (Table 2) may be considered low compared to that previously reported [10]; RECAP was designed to support usual care and this low frequency may limit any potential benefits of adding RECAP. The intervention group received a higher frequency of usual care than the control group. RECAP therapist consultations with the treating ward physiotherapist may have influenced this. However, the majority of patients who demonstrated a pattern of spontaneous recovery post ICU and discharged within one week of ICU discharge were in the control group. As a consequence the control group had both a shorter period of active inpatient study days and potentially did not require a higher frequency of usual care. The UK Intensive Care Society [30] endorse providing patients in ICU with at least 45 minutes of active intervention 5 days per week, delivered by specialised or adequately experienced therapists Due to the limited number of studies evaluating rehabilitation during ward-based recovery, there is no benchmark for the dose of usual care at this stage (i.e. ward based rehabilitation). NICE quality statement 158 [31] emphasises key quality standards of rehabilitation that should be components of usual care for this group, in particular goal setting, formal handover and communication pathways. There is a clear need for the development of evidenced based minimum standards for usual ward based care and for subsequent implementation of these. This would also help future trials to distinguish between usual care and any additional intervention.
Outcomes
Both groups appeared to demonstrate a similar pattern of improvement in both physical and psychological function over the study period. While not powered to detect meaningful differences between groups, the intervention group had higher baseline psychological scores (mean difference 13.3 points on SAI scores) and lower baseline physical function scores (mean difference 20.4 on FIM scores) by comparison to the control group. This potential relationship between physical and psychological function in patients post critical illness has previously been suggested [32] and further investigation is warranted to conclusively determine any relationship.
The rehabilitation satisfaction questionnaire used in this study shows the intervention group had a greater level of satisfaction with their rehabilitation experience. The questionnaire has not been validated but the development of a patient reported outcome measure that could better capture patient’s views is important. The importance of capturing patient experience with rehabilitation interventions has been highlighted in a recent paper [14], which showed a statistically significant benefit of increased rehabilitation in improving patient experience and perceived quality of life. While the associated intervention study did not demonstrate improvements to patient outcomes (physical function or quality of life), in contrast, the analysis of patient experience has.
Selection of an appropriate outcome measure for trials in critically ill patients that is responsive across the continuum of care is challenging [33–35]. As sequalae includes physical and psychological components we included a measure of both i.e. FIM and SAI respectively. The FIM appeared feasible to administer and is valid for telephone administration [36]. However, psychometric properties of the FIM have not been fully evaluated in this population, or across the continuum of recovery. The CPAX [37] provided a measure of physical function in this cohort at ICU discharge, however, at the time of study design, the responsive of the CPAX to ward based physiotherapy interventions had not been reported. The responsiveness of CPAX to detect improvement in physical function of critical care patients in a specialised burns ICU during their ICU and ward based care has recently been reported [38]. The development of a core outcome set for trials across all phases of rehabilitation following critical illness would be useful [39].
The main limitations of this study were that (i) all of the components of the RECAP intervention were not delivered fully as planned and the unanticipated short length of stay on the ward for many patients impacted on where consultations took place; (ii) the unanticipated low frequency of usual care delivery may have limited the RECAP capacity to support usual care and to influence outcome; (iii) the challenge of including a suitable outcome measure that is responsive to the provision of a brief intervention aimed at supplementing usual care.
Conclusion
RECAP is a brief intervention that is safe to deliver in conjunction with ward-based rehabilitation after ICU discharge. This study was helpful for identifying challenges that might need to be considered when designing a future study in this population at this timescale including the need for agreed standards of usual care, and optimisation of the RECAP intervention to help ensure a response can be elicited in the chosen outcome measures. It has also helped to highlight the need for further research in this population to establish the trajectory of recovery, factors predictive of recovery and the appropriate outcome measures to detect change in this population.
Conflict of interest
The authors have no conflict to report.
Funding source
None.
Footnotes
Acknowledgments
The authors wish to acknowledge the support of colleagues at SVUH; Catherine McLoughlin, Ciara Gill, Deirdre Molloy, Ruth McGlynn, Jeanne Keddy, Dr. Paul D’Alton and at Ulster University; Jackie Casey. In addition, we wish to thank the UCCDIP Project team as a whole and Suzanne Bench, the lead researcher for granting permission to use the UCCDIP as part of this study.