
Abstract
BACKGROUND:
Low back pain (LBP) is a common cause for disabilities and reduced autonomy in older adults. Exercise therapy has shown to be effective in the reduction of the symptoms of LBP with bridging exercises as a commonly used intervention. Exercise therapy can be supported with biofeedback-based methods in order to further improve motor control. The availability of relatively inexpensive devices like the Nintendo Wii opens up new methods for the treatment for biofeedback-based exercises for patients with LBP.
METHODS:
We conducted a 3-armed randomized controlled trial (biofeedback, standard care and control) with 62 older adults aged 66 to 89 years and an intervention period of twelve weeks with 2 sessions/week. Primary outcome was the perceived disability using the Oswestry Disability Index (ODI). Additionally, we evaluated usability and user acceptance of the feedback system.
RESULTS:
The biofeedback group demonstrated significantly lower levels of perceived disability compared to the control group. Additionally, the Biering-Sørensen test was significantly better in the standard care group compared to both other groups. Usability and user-acceptance for the biofeedback system was low, mostly because of connectivity and comfort problems during exercising.
CONCLUSIONS:
The biofeedback system was able to significantly improve perceived disability and back extensor muscle endurance in older people with subacute low back pain. As the user-acceptance issues were mostly based on technical reasons, higher levels of comfort and dependability of the system could provide an effective method to perform bridging exercises to alleviate the consequences of episodes of low back pain.
Introduction
Based on a large systematic review including data from 54 countries, low back pain (LBP) has a one-year incidence of first-ever low back pain from 6.3% to 15.4% and a mean lifetime prevalence of nearly 40% [1]. This results in LBP being the worldwide leading cause for life years lived with disability (YLD) [2]. Additionally, LBP has a mean point prevalence of 18.3% [1] which means that at any given point in time nearly 1 in 5 adults suffers from the consequences of LBP. There is evidence that LBP causes a great socioeconomic burden, mainly due to a large number of work days lost, but also due to an excessive use of therapeutic services [3]. This burden seems to be growing, in spite of technological advances in diagnostics and intervention [3]. For the management of subacute as well as chronic LBP, several guidelines recommend a combination of pain management, manual therapy, and early active therapy including exercises [4, 5]. Additionally, group exercises can provide the same effectiveness as One-on-One therapy sessions while being potentially more cost-effective [6]. Activity-enhancing concepts seem to be especially important in an older population. While there is some evidence that severe LBP prevalence is increasing with age [7], a systematic review by Taylor et al. (2014) reported that in older people of 70 + years, higher levels of strength in comparison to other individuals in the same age had a protective effect on the occurrence of LBP episodes [8]. Similarly, Wong et al. (2017) reported that strength exercises lowered the risk for occurrences of LBP in older men aged 65 + [9]. However, the management of LBP in older people is rarely evaluated in scientific studies [10].
Modern technical innovations like biofeedback devices open up new potentials in exercise therapy. Biofeedback provides information via two different strategies, direct feedback or transformed feedback [11]. Common biofeedback applications include heartrate monitoring, electromyography (EMG) feedback or biomechanical feedback of movements. Feedback on posture or forces are directly presented as measured values or indirectly using visual, sound or vibration signals [11]. Biofeedback (BF) technologies provide new opportunities to enhance efficacy as well as long-term motivation in LBP exercises. A recent randomized controlled trial (RCT) by Kent et al. (2015) using body-worn sensors able to provide visual, audio and vibration feedback while exercising as well as in daily life of patients with chronic LBP lead to significantly superior results in the BF group regarding activity limitations and pain intensity compared to standard care [12]. Additionally, a cost-effectiveness analysis of the intervention could demonstrate a high economic effectiveness [13]. In another study by Ahmed et al. (2016), an EMG-based system used for BF during trunk stabilization exercises showed significantly higher improvements in functional disability and pain reduction compared to an exercise group without the BF [14]. A systematic review (SR) conducted by Matheve et al. (2017) could further demonstrate the general effectiveness of BF-based interventions in patients with LBP, though the SR could not observe significant differences when BF was the only difference between intervention and control group [15]. Using force platforms (FP) as a mean for providing biofeedback is potentially one possible form of providing biofeedback in managing LBP.
In principle, FPs measure the weight distribution in a given position and are combined with a visual, auditory or other signal to provide feedback for the user [11]. Zijstra et al. (2010) evaluated the use of BF for training balance and mobility in older people in a systematic review [16]. Though they did not specifically limited their review onto the use of FP, all included studies that evaluated either standing balance or transfer training used a combination of FP and visual FB. While these studies found no significant group differences in stroke rehabilitation, training balance in frail older adults demonstrated significant differences between intervention and control groups. While these results highlight the general applicability of FPBF, it is unclear if this form of BF can be used in the rehabilitation of LBP, too.
Muscular imbalance is frequently found in patients with LBP and often discussed as a potential cause for recurrent LBP [17]. Also, muscular imbalance of the trunk muscles is discussed to lead to an asymmetric execution of trunk movements [17, 18] and repositioning after movement [19]. Based on this thought, exercise concepts for patients with LBP should include retraining muscular symmetry to reduce the negative effects of this condition. In this, BF-based exercising of symmetrical activation of trunk muscles could potentially help LBP-patients in regaining a more symmetrical activation of their trunk muscles and further enhance the efficacy of exercising after episodes of LBP.
Bridging exercises are a commonly used exercise modality for the rehabilitation of LBP. They are relatively easy to execute and have shown to effectively target trunk muscles [20]. However, research on bridging exercises seems to focus on activation patterns [21–23] and muscle thickness [24, 25]. However, symmetric trunk activation in a lying position is difficult to observe for PTs. Therefore, providing BF about the symmetry of the body position could potentially enhance the performance of bridging exercises by providing visual feedback. However, to the knowledge of the authors, no studies on this topic have been published.
We therefore developed a BF-system consisting of two commercially available FPs and a tablet for providing visual feedback while performing bridging exercises. We here present the results of a randomized, controlled trial (RCT) to evaluate the effectiveness of bridging exercises with additional visual biofeedback for assisting exercise performance in the treatment of LBP patients. As the primary outcome, we defined the perceived disability due to LBP as measured with the Oswestry Disability Index (ODI). Secondary outcome parameters included additional questionnaires on perceived disability, isometric trunk strength and endurance, mobility, fall risk, and sleep quality, as well as the usability and user acceptance of the biofeedback system.
Methods
Design
We conducted a 3-armed RCT with biofeedback exercises (BF), standard exercises (SC) and control group with no intervention (C). Participants aged 65 or older with subacute or chronic LBP were included.
Recruitment and randomization
Participants were recruited through leaflets placed in local pharmacies, senior activity centers and GP's offices. These leaflets contained a short description of the planned study as well as the expected time each participant would need to commit to the study and contact information of the principal investigator (PI). Those who were interested in participating could contact the PI by telephone or email. Potential participants received a detailed written study information and additionally were verbally informed about the study via telephone before the study started. During this phone call, the PI screened for inclusion and exclusion criteria using a standardized checklist. Inclusion criteria were an age of 65 years or older and either subacute or chronic LBP. Exclusion criteria were any self-reported or apparent present affective or cognitive diseases, participation in another intervention study, legal care, immobility, recent surgical intervention, acute herniated disc or spinal tumor, and no written consent. All exclusion criteria were judged based on the report of the participants, in cases where they were not able to give a clear answer, we asked for clarification of these issues by their family doctor or a specialist. Surgical intervention were defined as recent when the procedure was performed during the past 4 weeks prior to the study or if the participant was limited in their mobility because of the surgery.
Subjects were randomly assigned to one of the three arms of the RCT, biofeedback exercises (BF, n = 20), standard exercises (SC, n = 20) and control group with no intervention (C, n = 20) (Fig. 1). Randomization was performed with drawing pre-prepared opaque envelopes containing the group assignment after inclusion and measuring all baseline data. This way, group assignment was not influenced by the results of the baseline measurements. Due to the nature of the intervention, neither participants nor the therapists leading the group interventions could be blinded. Two subjects withdrew their consent after allocation to the BF group. Sixteen more subjects were lost to follow-up. Reasons for this, as well as the complete enrollment and allocation process are shown in Fig. 1.
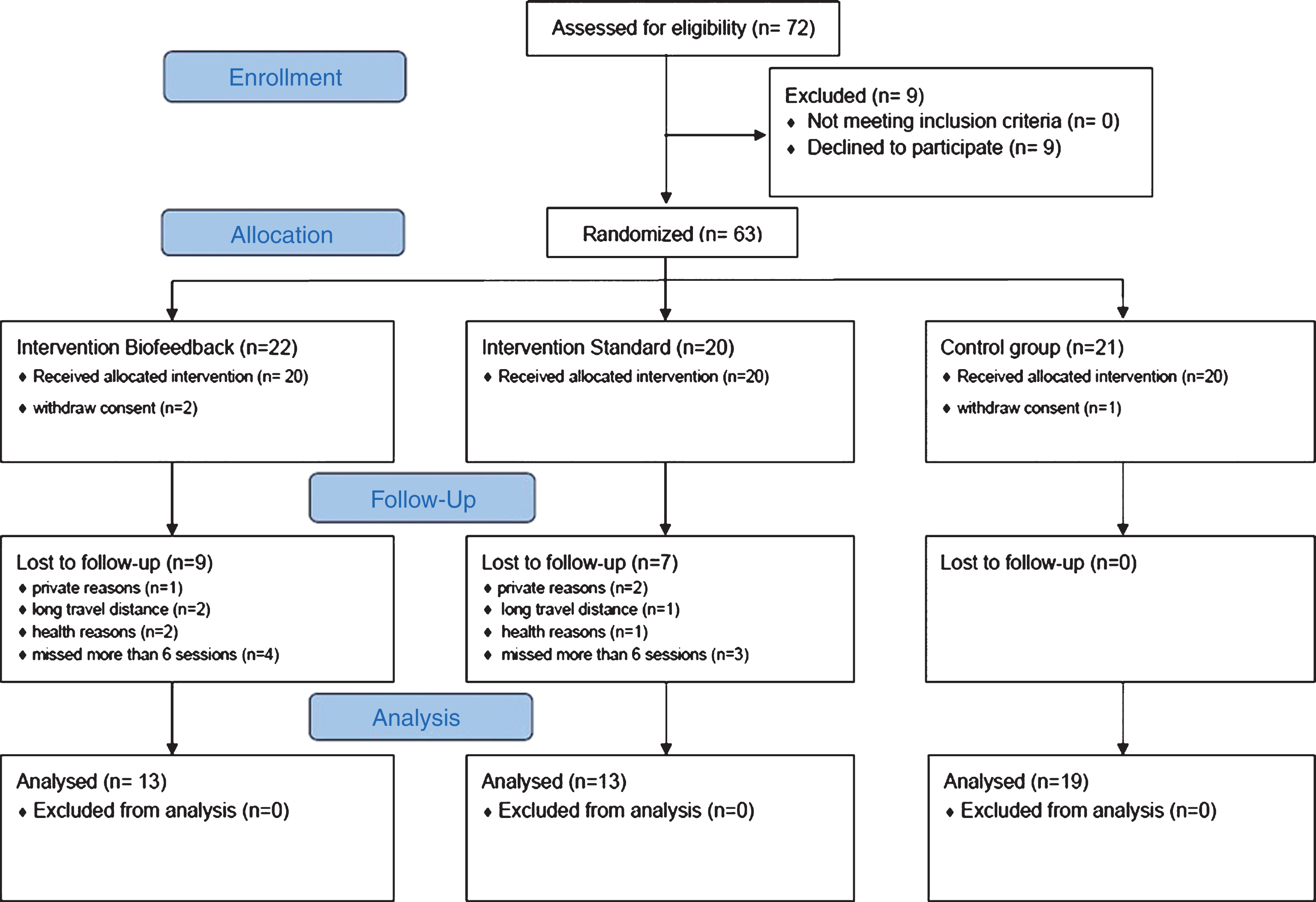
Flow diagram of enrollment and intervention.
Randomization was performed with drawing pre-prepared opaque envelopes containing the group assignment after inclusion and measuring all baseline data. This way, group assignment was not influenced by the results of the baseline measurements. Due to the nature of the intervention, neither participants nor the therapists leading the group interventions could be blinded. Two subjects withdrew their consent after allocation to the BF group. Sixteen more subjects were lost to follow-up. Reasons for these as well as the complete enrollment and allocation process are shown in Fig. 1.
Both intervention groups performed identical bridging exercises twice a week, 30 min per session, over a total period of 12 weeks. The SC group performed the exercises on a sports mat while the BF group trained on Wii Balance Boards (one for the feet, one for the shoulders), receiving feedback on a Samsung Galaxy Tab 2 tablet attached to a tripod in front of the foot Balance Board (Fig. 2).
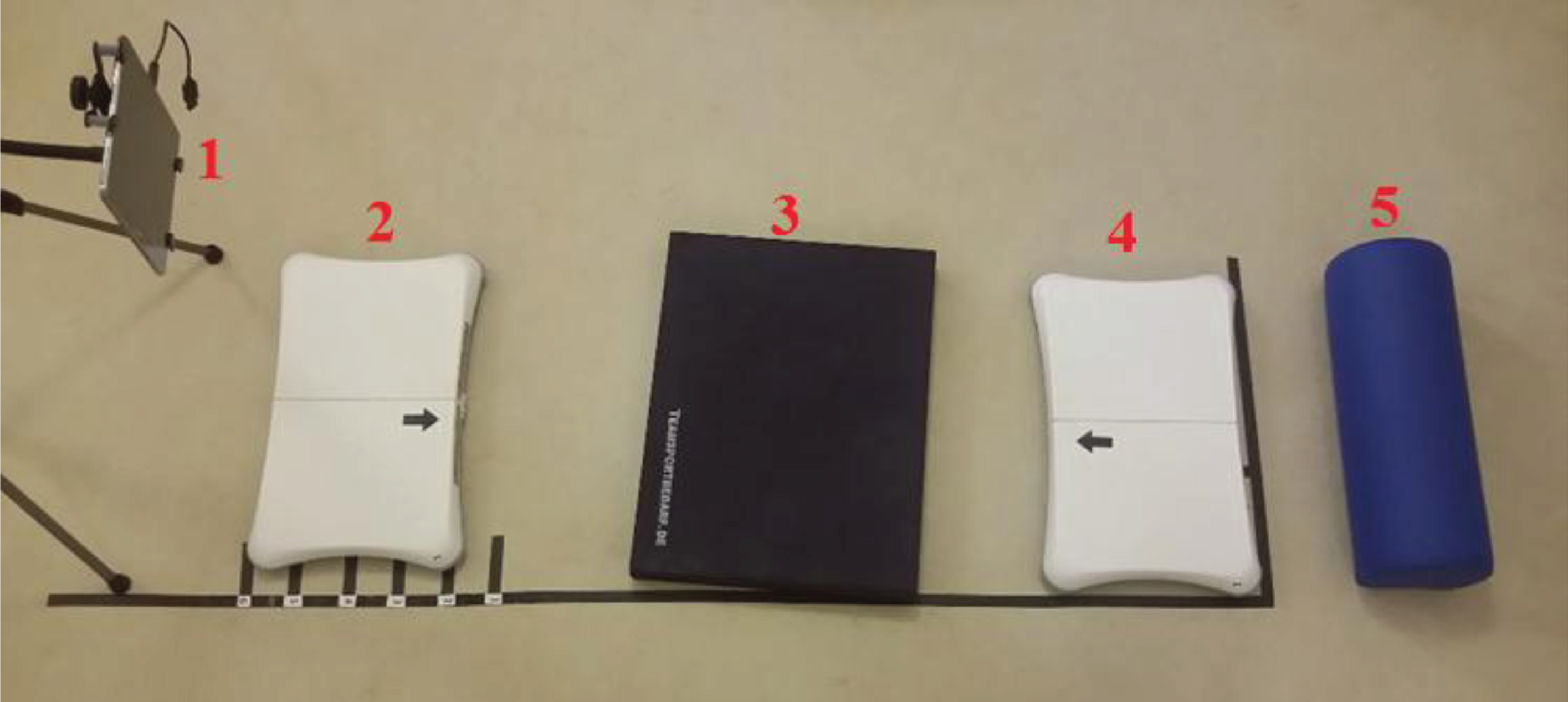
Setup of the devices in the biofeedback group. 1 = Tablet mounted to tripod; 2 = Balance Board for the feet; 3 = bolster to rest the pelvis; 4 = Balance Board for shoulders; 5 = Pillow.
The Wii Balance Board (Nintendo, Kyoto, Japan) was originally designed to provide real-time feedback during gaming. However, compared to Force Plates, it demonstrates good validity in terms of standing balance [26].
All subjects in both intervention groups executed 16 different variations of bridging exercises in supine position, with hips flexed at a 45-degree angle and the knees at a 90-degree angle. The 16 different exercises consisted of basic bridging exercises who were combined with changes in the hip abduction angle as well as hip, feet and arm movements which all have shown to change the activation patterns of the trunk muscles in bridging exercises [19, 26]. These combinations resulted in the 16 different exercises who were, after teaching each patient the core elements of bridging, performed in a randomized order at each session. Additionally, the ratio between exercising and resting time between each exercise was progressively changed. At the start of the intervention, each exercise cycle lasted for 20 seconds followed by a 60 sec. resting period. The duration of the exercises was then increased by 10 sec. every four weeks, while the resting period was decreased for the same amount.
At the start of each exercise cycle, the pelvis was lifted off the ground while performing an abdominal drawing-in maneuver (ADIM). This maneuver aims at co-activating the deep trunk muscles of the back and abdomen [27] to stabilize the lumbar spine during movements. This maneuver has already demonstrated a significant effectiveness in reducing pain intensity and functional ability in patients with LBP [28]. A specially trained instructor supervised all exercises. Instructions of all 16 exercises were standardized based on a written standardized protocol.
Subjects in the BF group saw their center of pressure in each FP represented by a small white dot within the larger blue circles (Fig. 3) displayed on the tablet. A shift of a subject’s center of pressure caused the dot to move in that direction. The bottom circle represented the center of pressure for the feet, while the upper circle displayed it for the shoulder region. Subjects were instructed to maintain both dots as centered as possible to enable a symmetrical execution of the exercise. For example, lowering the pelvis on one side would lead to a rotation of the trunk and pelvis. Consequently, the dots would move to the side the pelvis was lowered, indicating an asymmetrical position to the subject and enabling him/ her to correct the position.
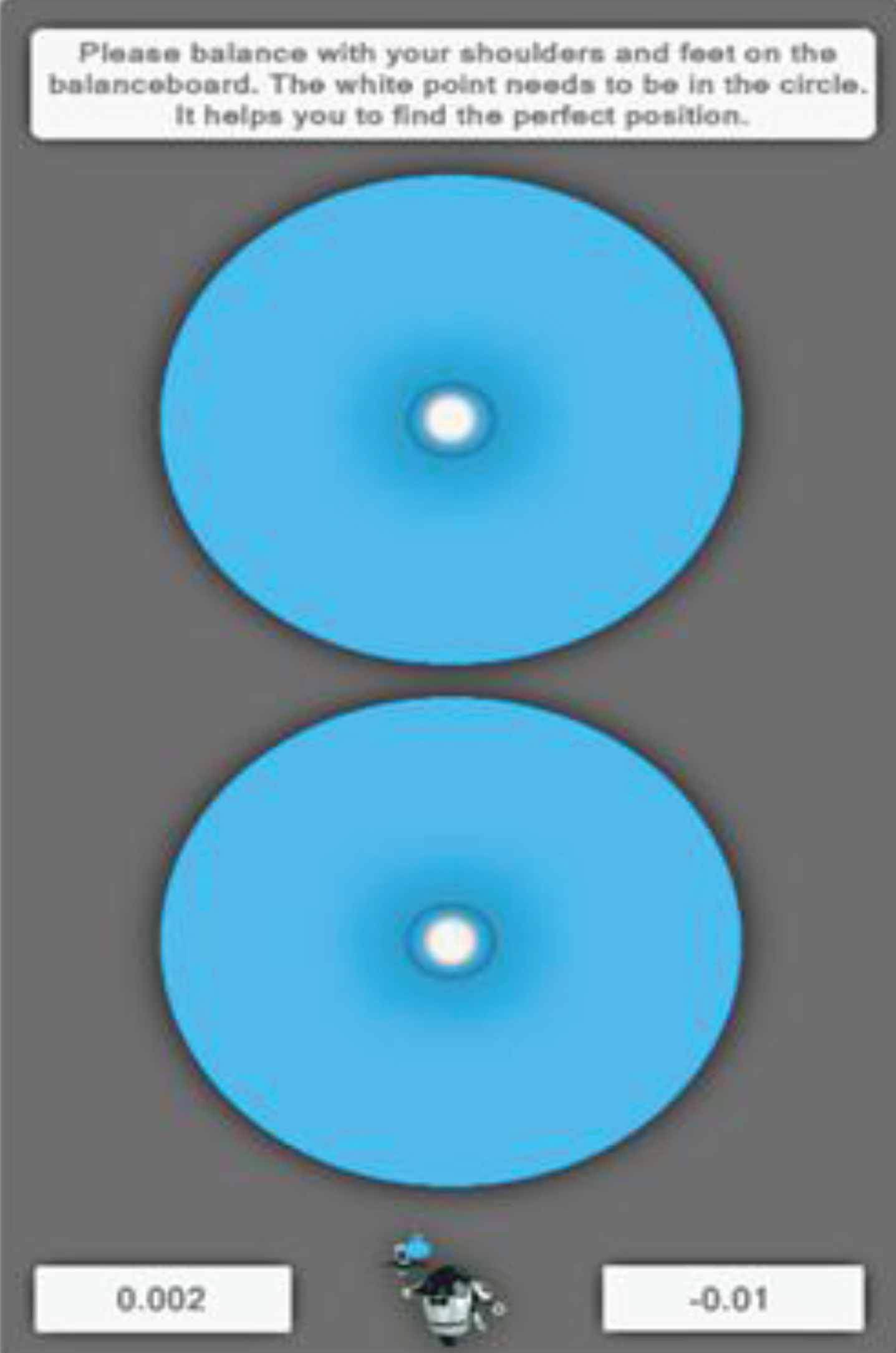
User interface of the biofeedback group.
Prior to the start of the intervention, information was collected on sociodemographic data, average daily H2O consumption, and severity of back pain by a set of validated questionnaires and functional test. Additionally, participants were asked about their 1) subjective estimated hearing and visual ability, 2) fine motor skills, 3) general well-being, and 4) mobility. Furthermore, the participants’ level of technology acceptance was assessed with questions about 1) general attitude towards technology, 2) use of personal computers, tablets or smartphones, 3) use of mobile phones, and 4) online activities over the last 30 days.
For pain measurements, the Oswestry Disability Index (ODI) [29], the Hannover Functional Questionnaire in ambulatory diagnosis of functional disability caused by backache (HFQ) [30], and the Roland-Morris Disability Questionnaire (RMDQ) [31] were used. The translated and validated German versions of the ODI [32] and the RMDQ [33] were used. Sleep quality was measured with the Pittsburgh Sleep Quality Index (PSQI) [34]. Fall risk was assessed with the Four Square Step Test (FSST) [35] and the Five Times Sit to Stand Test (5T-STS) [36]. Isometric strength measurements of the lateral and anterior trunk flexion were performed with a handheld dynamometer (Sauter FK 1k, Balingen, Germany) in an upright, sitting posture. Muscular endurance of spinal erector muscles was measured with the Biering-Sørensen test (BST) [37]. All measurements were performed by the principal investigator (FF).
All tests were repeated at the end of the intervention period. Additionally, the BF group evaluated the biofeedback device with the User Experience Questionnaire (UEQ) [38]. Another questionnaire developed by the research team was used to evaluate perceived motivation and enjoyment, as well as efficiency during the exercises.
We excluded subjects from the study analysis when they missed more than six exercise sessions. Session adherence was documented with the help of a session protocol filled out by the instructor at each session.
The study was approved by the Ethics Committee of the Charité Universitätsmedizin Berlin (EA4/008/16).
Statistical analysis
All interval-scaled baseline was tested for normal distribution using the Kolmogorov-Smirnoff (KS)-Test. Descriptive statistics of these data were derived as mean or median values based on the results of these tests and tested for significant differences between the three groups using an ANOVA or Kruskal-Wallis test. Prerequisites for both tests were performed as needed. For testing the effectiveness of the intervention, the change score was calculated for each variable and tested again for normal or non-normal distribution before performing ANOVA or Kruskal-Wallis statistics.
User acceptance was compared between both interventions and compared using either the Chi2 or the Wilcoxon Test.
Statistical analysis of data was performed using Excel and IBM SPSS Statistics 22.
Results
Effectiveness of the intervention
Details of the participants’ enrollment process are shown in Fig. 1. The study included 62 participants (44f, 18 m) with subacute LBP. For an overview about baseline data please refer to Table 1. Age, weight and BMI showed normal distribution while height of the subjects did not. The majority of the participants were retired (54) and lived independently (60). Attitude towards technology was positive in 51 cases, neutral in nine and negative in two subjects. The perceived health of all participants was good or very good in 40 participants. Perceived mobility was rated good or very good in 44 participants. Of the conducted measurements at baseline, only the ODI and the PSQI were normally distributed. Over the course of the study, 17 subjects dropped out of the study. The main reason for this was a delay of the investigation due to technical reasons, which led to conflicts with the patients’ personal agenda. No adverse events occurred while exercising. None of the tested parameters showed significant differences between the groups at baseline.
Sociodemographic and baseline data of all participants (n = 62)
Sociodemographic and baseline data of all participants (n = 62)
Abbr.: 5T-STS: 5-times sit-to-stand test; BF: biofeedback; BST: Biering-Sørensen test; C: control group; FSST: Four Square Step Test; ODI: Oswestry Disability Index; PSQI: Pittsburgh Sleep Quality Index; RMDQ: Roland-Morris-Disability Questionnaire; SC: standard care. 1mean values. 2median values.
Tests for the change scores revealed a general tendency for nonparametric distribution. We therefore decided to perform the Kruskal-Wallis test for all variables to allow for better interpretability of the results. Significant differences between the three groups could be observed for the ODI (H(2) = 8.085, p = 0.018), isometric strength testing of left lateral flexion of the torso (H(2) = 9.441, p = 0.009) and the BST (H(2) = 12.025, p = 0.002).
For all significant results, pairwise comparison tests were performed post-hoc using Dunn’s (1964) procedure with a Bonferroni correction for multiple comparisons [39]. This post hoc analysis resulted in the identification of statistically significant differences between the three groups as shown in Table 2. Adjusted p-values are presented.
Results of pre- and post- measurements of the applied instruments
Abbr.: 5T-STS: 5-times sit-to-stand test; BF: biofeedback; BST: Biering-Sørensen test; C: control group; FSST: Four Square Step Test; HFQ: Hannover Functional Questionnaire; K-W Test: Kruskall-Wallis test; ODI: Oswestry Disability Index; PSQI: Pittsburgh Sleep Quality Index; RMDQ: Roland-Morris-Disability Questionnaire; SC: standard care. 1mean values. 2median values. *Significant difference between groups.
Based on this analysis, change in ODI was significantly higher in the SC group in comparison to the control group. Isometric trunk flexion to the left side was significantly enhanced in the BF group compared to the control group. Finally, the BST was significantly improved in the BF group compared to the control group as well as the SC group.
Because of these somehow inconsistent results, we decided to perform a post-hoc-analysis for comparing the change scores of both intervention groups to the control group. Therefore, we pooled the data from the BF and the SC group and performed a Mann-Whitney-U-Test for non-parametric comparison of two groups. Results of this analysis for all variables are displayed in Table 3.
In-between differences for statistically significant results of the Kruskal-Wallis-Test
Abbr.: BST: Biering-Sørensen test, n.s.: not significant, ODI: Oswestry Disability Index.
Again, the ODI was significantly improved in the group receiving the intervention in comparison to the control group (p = 0.035). Both the other questionnaires on disability due to LBP (RDMQ, FFbH) revealed no significant differences between the two groups. In addition to the ODI, all isometric strength measurements were found to be significantly more improved when comparing their results to the control group (Table 4).
Comparison of intervention and control group (median (IQR) values)
Abbr.: 5T-STS: 5-times sit-to-stand test; BF: biofeedback; BST: Biering-Sørensen test; C: control group; FSST: Four Square Step Test; HFQ: Hannover Functional Questionnaire; M-W Test: Mann-Whitney-U-test; ODI: Oswestry Disability Index; PSQI: Pittsburgh Sleep Quality Index; RMDQ: Roland-Morris-Disability Questionnaire; SC: standard care. *Significant difference between groups.
As can be seen, the ODI as well as all isometric strength measurements revealed significantly higher results when comparing the pooled data of both intervention groups with the control group.
Subjects in the BF group found the exercise program significantly less motivating (p = 0.024) than the standard intervention group. However, for experiencing fun and enjoyment while performing the exercises and the perceived efficiency of the exercises themselves, no significant differences between both intervention groups were found. The intensity of the exercises was rated as “moderate” by 27.3% and as “just right” by 72.2% of the standard intervention group and “just right” by 100% of the BF group.
The subjects raised several negative points for the biofeedback trainer, mostly related to connectivity problems between the boards and tablets. If disconnected, it had to be reconnected by the instructor of the session and the subject had to get off the affected boards, since the “connect”-buttons are located at the bottom side of the boards. Furthermore, in 34 documented instances no connection could be established between the boards and the tablets. Consequently, the subjects had to perform their training on the sports mat, similar to the standard intervention group. Another downside was the occasional sliding of the boards on the floor, which then had to be repositioned. Some users raised concerns about the comfort of the boards, especially the hard surface of the shoulder board was perceived as uncomfortable.
Based on the results of the UEQ, participants in the BF group rated the “Novelty” and “Perspicuity” domains as “above average” to “good”, while “Attractiveness”, “Efficiency”, “Dependability” and “Stimulation” were rated “below average” to “bad” (Fig. 4).
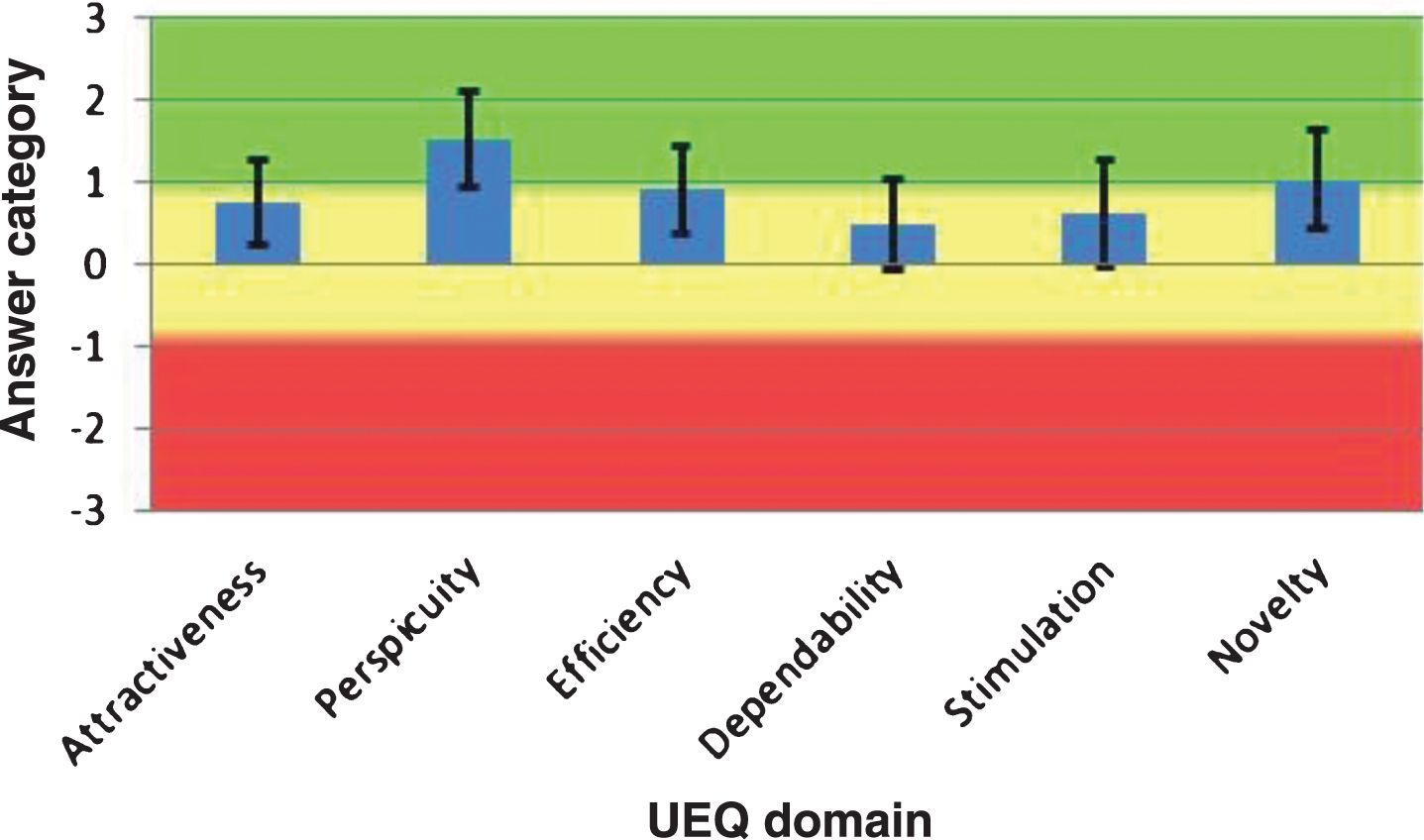
UEQ domains of the biofeedback device.
The presented study investigated the effectiveness of bridging exercises in a randomized controlled trial with older adults with subacute LBP. Exercises were either performed conventionally on a mat or with the help of a biofeedback device. The results in comparing the three groups regarding disability, sleep quality, function and isometric strength were very inconsistent and hard to interpret given the low number of participants as well as some methodological limitations in our study. First, the dropout rate of the study was rather high due to the delayed start of the study, leading to a potential population bias. However, despite the dropouts, the three groups were still comparable in all baseline parameters. Furthermore, no EMG measurements were performed to verify a symmetric or asymmetric recruitment of the paraspinal muscles and its correlation with the biofeedback signal of our device. These measurements were not conducted as the position of the participants and the electric signals of our device could have influenced the EMG signals. In the light of our results and the possibility that such measurements could have provided a conclusive explanation for the observed phenomenon, we see the need to solve these concerns in future studies. Third, we were not able to check for any additional interventions our subjects in all three groups were potentially receiving. Therefore, the question on whether a BF-assisted program for bridging exercises is more effective than performing these exercises conventionally cannot be answered. Although we found some evidence that the exercises themselves are effective in enhancing isometric core strength in all measured muscle groups, these findings can only be interpreted with caution due to multiple testing, the low number of participants and missing information on pain duration as an important indicator for chronic LBP in comparison to subacute back pain. Nevertheless, they still merit some further discussion. Recent investigations of the efficacy of bridging exercises were focused on activation patterns [21–23] and muscle thickness [24, 25]. Thus, to our knowledge this is the first analysis that demonstrates the ability of these exercises to improve core strength. Therefore, further research with a clear prospective design is needed to verify or reject the exploratory results of our analysis. Furthermore, improvement in strength measurements alone bear no clinical importance. However, our results regarding perceived disability due to LBP are, again, inconclusive. While the ODI was significantly improved when comparing intervention groups with the control group, both the RMDQ and the HDQ did not show any significant differences. Several possible reasons should be discussed in this context. First, the number of participants was relatively low and were not based on a sample size calculation. Thus, some inconsistency could be expected. Second, the intervention in or trial consisted solely of bridging exercises. While exercising shows a clear evidence in the treatment of LBP [40], it is recommended to include other intervention such as manual therapy into the therapy of LBP [5]. As the evidence in these guidelines further point out, the effectiveness of these interventions often apply to subgroups of LBP patients while others do not profit from them. In this case, a thoroughly diagnostic and treatment planning process is necessary to provide an optimal treatment program based in individual needs for each patient. Therefore, a significant reduction of perceived disability cannot be expected based on a single type of intervention in a heterogeneous population. Finally, the pre-intervention scores of all three instruments showed very low levels of perceived disability. Therefore, a further improvement was not expectable.
None of the measured parameters on mobility and sleeping quality could be improved significantly in any of the groups. As high baseline values for these factors were found, the margin for potential improvement was low. Future studies on this topic should therefore include patients with lower levels of sleep quality and overall mobility in order to be able to detect any potential improvements. A study performed by King et al. (1997) demonstrated some evidence that sleep quality in older adults can be improved with regular exercising [41]. However, the exercises in this study consisted mainly of endurance training while in our study isometric trunk exercises were provided. This could explain our lack of observed improvement of sleep quality.
Another point of concern in our study was the low level of user acceptance of the biofeedback system. Participants in the biofeedback group found the training less motivating than the standard care group. Reasons for this were reportedly connectivity and discomfort with the biofeedback trainer. The UEQ showed corresponding information and overall revealed a below average user experience. Based on these results, we cannot determine if changes in comfort and reliability of the system would lead to better training results. According to related usability research, dependability on a technological level is a basic requirement for the successful evaluation of technical systems providing exercise for older people [42]. As our system was not able to provide this level of stability, the low results of the UEQ are not surprising. Furthermore, the different surfaces for the two intervention groups could have an overall influence on the exercises beyond questions of comfort and technical reliability. However, as the exercises per se demonstrated a certain level of effectiveness, both the evaluation and refinement of the exercise regime itself as well as the technological development of the biofeedback system merits further consideration.
Conclusion
Bridging exercises resulted in increased isometric strength values of the core muscles in older adults with subacute low back pain. While the biofeedback system failed to demonstrate additional efficacy, the overall results suggest to integrate bridging exercises into LBP therapy programs.
Conflict of interest
All authors declare that they have no conflicts of interest or financial interests regarding the results of this study.
Footnotes
Acknowledgments
The study was conducted by the Geriatrics Research Group, Charité-Universitätsmedizin Berlin as part of the ALFRED project. ALFRED – Personal Interactive Assistant for Independent Living and Active Ageing – is a project funded by the Seventh Framework Programme of the European Commission under Grant Agreement No. 611218. Neither the European commission nor the partners in the ALFRED project had any influence in conducting, analyzing or presenting results from this study.