
Abstract
Frozen Shoulder remains one of the most misunderstood pathologies to affect the shoulder joint. Frozen Shoulder is characterised by pain, loss of active and passive range of motion especially in flexion and external rotation with normal radiological findings undergoing three stages of presentation: initial pain, stiffness and near full resolution with time. Current treatment options include manual physiotherapy techniques, injection therapy, manipulation under anaesthetic and surgical release of shoulder capsule. Presently there remains a paucity of significant research supporting the sole use of any of these techniques in the treatment of frozen shoulder. Future studies should incorporate larger subject populations with closely related symptoms and be multicentred across a larger geographical area.
Keywords
Introduction
The Gleno-humeral joint is classified as a ball and socket joint formed by the articulation of the rounded head of the humerus and the shallow glenoid cavity of the Scapula. Architecturally the joint has sacrificed much of its stability for mobility, such that it exhibits six degrees of freedom [35]. Consequently, the Gleno-humeral joint may be exposed to different mechanisms of traumatic and non-traumatic related injuries such as dislocation, fracture, tendon and ligament injury [21, 27]. One injury which may have its origins in one or both mechanisms of injury, and remains very misunderstood, is the “Frozen Shoulder”.
Frozen Shoulder is characterised by pain, loss of active and passive range of motion especially in flexion and external rotation with normal radiological findings undergoing three stages of clinical presentation: initial pain, stiffness and near full resolution with time [3, 29]. Previously, researchers have attempted to capture the nature of this injury by assigning descriptive terminology and by highlighting the principle symptom and potential underlying pathology. Codman [12] originally coined the term “Frozen Shoulder” based on the belief that this was a self-limiting pathology which would reverse itself over time and was later sub-categorised into Primary Idiopathic and Secondary Traumatic Frozen Shoulder [25].
Neviaser (1945) suggested the term “Adhesive Capsulitis” based on the premise that the shoulder capsule was adhered to the humeral head. However, later evidence indicated the absence of such “adhesions” and proposed instead that the capsule underwent synovial thickening and progressive contracture [44]. To address the lack of agreement on a consensus definition and classification of frozen shoulder, 211 members of the American Shoulder and Elbow Surgeons were surveyed [51]. Having received 85% agreement, they advanced Lungburg’s classification (1969) by expanding upon the Secondary classification category to include systemic, extrinsic and intrinsic frozen shoulder types of known aetiology (see Fig. 1). More recently the term “The Frozen Shoulder Contracture Syndrome” (FSCS) [15] has been utilised to describe this condition more succinctly based on the two most prevalent descriptors of this injury as described previously [7, 49] and will be used for the remainder of this review.
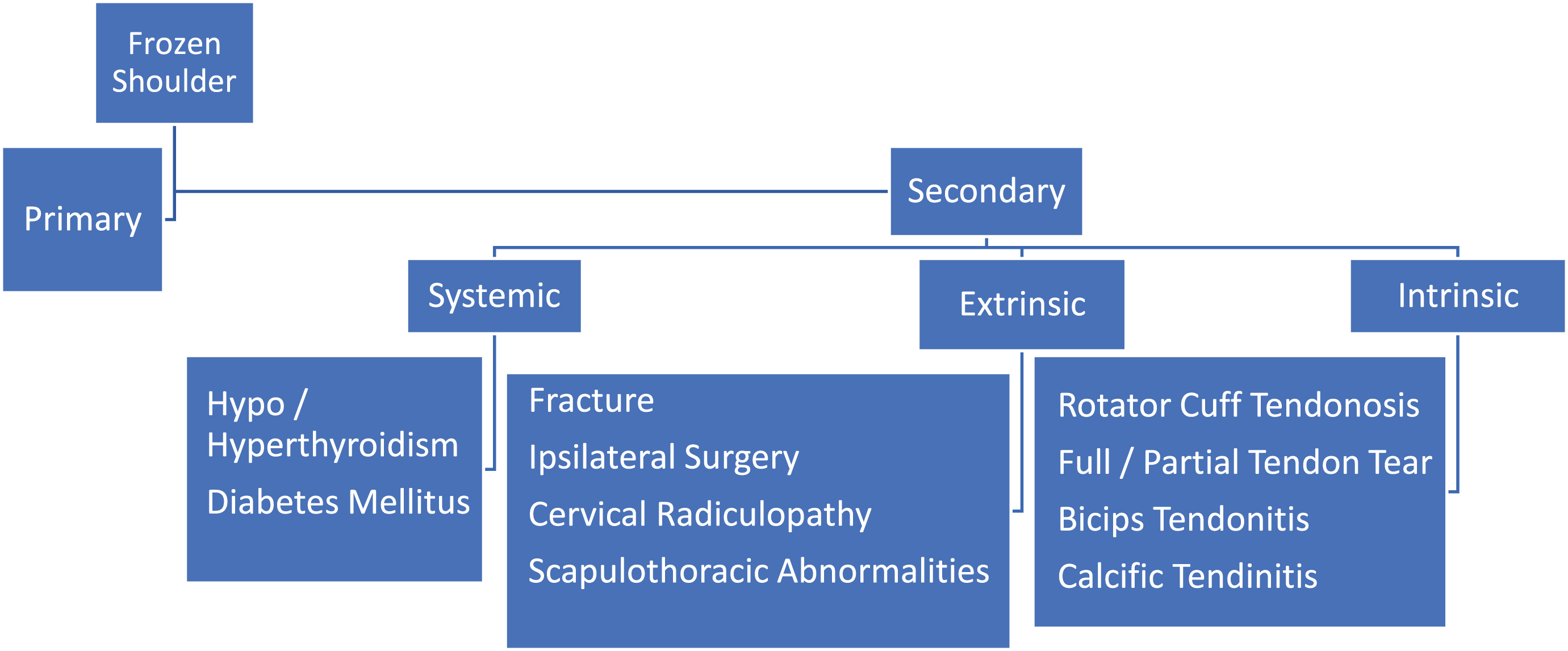
Zuckerman and Rokito Classification of Frozen Shoulder (2011).
There is a paucity of reliable or accurate prevalence data within the general population due to the complexity of this condition. Poorly designed quasi-experimental studies with small heterogenous populations and improper classification of the various stages of the disease has resulted in poor quality research. However, overall incidence of shoulder complaints in General Practice has been reported between 9.5–14.2% per one thousand patients [28] with rotator cuff related diseases estimated at 60–70% of all shoulder lesions [4]. The most recent prevalence rates identified for FSCS were between 2–5% of the general population with women (10.1%) affected more than men (8.2%) [3, 42]. The mean age onset was 53.4 years with 20% exhibiting bilateral symptoms [18]. Pre-existing disease states such as diabetes mellitus and hypo/hyperthyroidism are high risk factors for developing FSCS and are also prognostic indicators of poor outcome with this condition with a prevalence rate reported to be between 4.3% and 38% respectively [1, 2].
The duration of FSCS remains unclear. Grey (1978, cited in [46]) proposed the Natural History Theory to explain how FSCS presented. This theory suggested that FSCS did not require any intervention as it was foremost “self-limiting” and would resolve fully with time after it had passed through the pain, freezing and thawing phases respectively. However subsequent scientific analysis of the literature examining this theory of progression could find no research evidence to support its existence [46]. The average duration of FSCS has been reported in the literature to last from 4 months to 30.1–36 months [47]. However, there is some evidence to suggest that the longer the frozen phase the more likely the recovery phase will be extended [15] and in some instances residual functional loss may last up to 4.4 years [18].
Pathogenesis
Limited progress has been made in establishing the underlying pathology of FSCS which may explain the difficulty in reaching a comprehensive diagnosis. Histological and immunocytochemical analysis have indicated that the gleno-humeral joint capsule and coraco-humeral ligament within the Rotator Interval (see Fig. 2) may undergo pathological changes similar to Dupuytren’s Contracture [6, 44]. Inflammatory mast cells, prolific fibroblastic cell activity, neurogenesis, neovascularisation and T/B cells have been identified in recalcitrant biopsied tissues [6, 48]. These findings not only support the theory that FSCS is a both a chronic inflammatory condition and a fibrotic condition but may also be immunomodulated [18]. On a macroscopic level surgical intervention studies have found the coraco-humeral ligament and the rotator interval in a contracted state with reduced laxity of the inferior axillary fold. Surgical release of these contractures led to immediate improvement in gleno-humeral external rotation and subsequent pain relief by eliminating the “check rein” hold on this movement [26, 34].
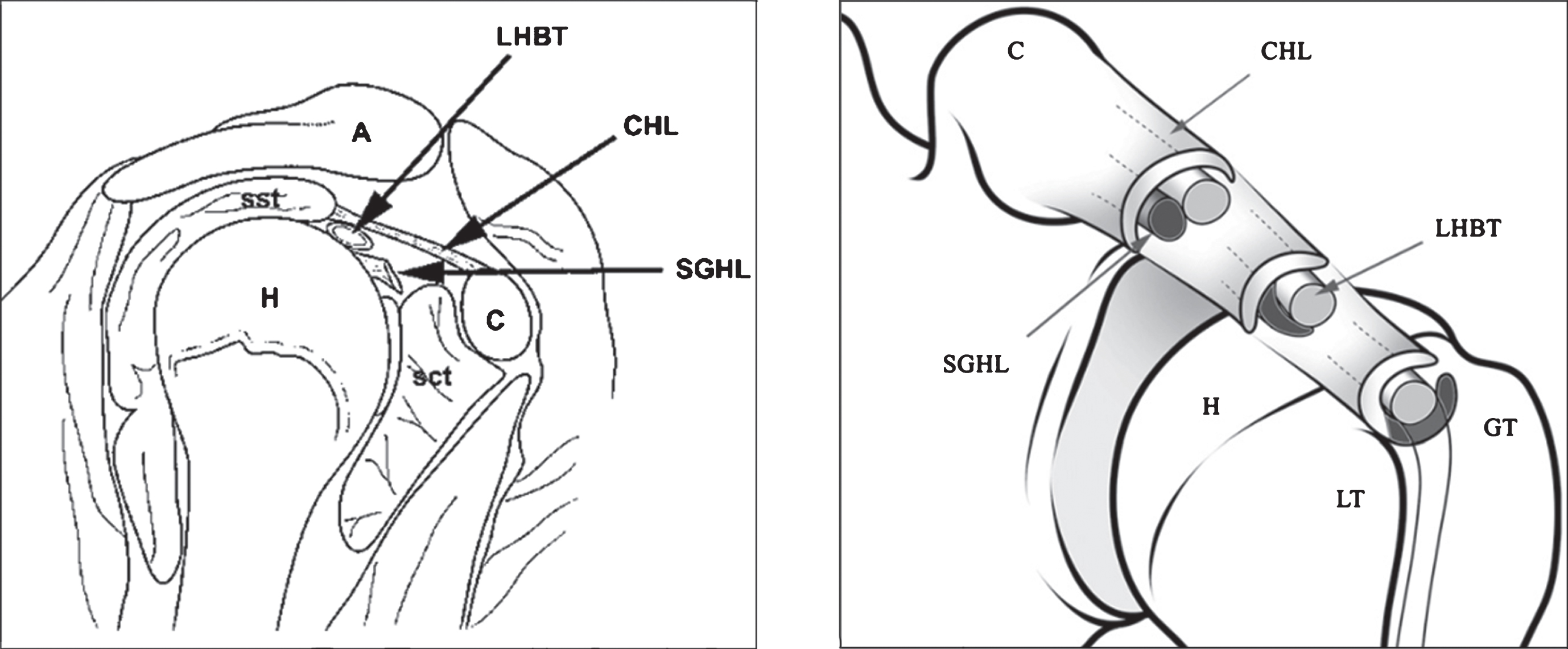
The Glenohumeral Joint & Rotator Interval, LHBT-Long head of Biceps tendon; CHL – Coracohumeral ligament; SGHL-Superior Glenohumeral ligament; H-Humerus; Sct-Subscapularis tendon; Sst-Supraspinatus tendon; C-Coracoid process; A-Acromion; LT-Lesser tubercle of the Humerus; GT-Greater tubercle of the Humerus. (Figure taken from Lee et al. (2007), MRI of the rotator interval of the shoulder, Clinical Radiology 62, 416-423. Reproduced with permission from The Royal College of Radiologists.)
FSCS can vary in severity from mild pain and less restrictive movement to severe pain with resultant loss in shoulder movement in multiple planes depending on the severity of the pain [26]. FSCS is predominantly diagnosed based on the patient’s medical history, radiological exclusion of intra-articular fractures, loose bodies and acromio-clavicular osteoarthritis or rheumatoid arthritis. Magnetic resonance imaging may also have a role to play in the diagnosis of FSCS due to its ability to detect specific abnormalities in the shoulder joint such as thickening of the coraco-humeral ligament and rotator interval, obliteration of the sub-coracoid fat triangle and finally synovitis-like changes around the long head of the biceps brachii tendon [50]. However, this method of assessment may not be available to all patients.
More practically the Coracoid pain test as a pathognomonic sign of FSCS in which digital pressure on the coracoid process produced pain in 96% of patients with FSCS [8]. Symptoms may also be evaluated comparatively with Codman’s [12] Frozen Shoulder diagnostic triage (points 1–7) which still holds true today and/or those previously suggested [43], (points 8–10) (see Table 1).
Codman’s Diagnostic Triage (1934) [23]
Codman’s Diagnostic Triage (1934) [23]
Clinicians are strongly advised to utilise only validated outcome measures in the management of patients with FSCS [22, 41]. Disability of Arm Shoulder and Hand (DASH) [20], Shoulder and Pain Disability Index (SPadi) [5] and the American Shoulder and Elbow Surgeons patient self-report questionnaire [36] are the most frequently utilised and investigated upper limb outcome measures and have undergone the scrutiny of systematic reviews [16, 37]. Although these instruments are widely used there remains conflicting evidence in the interpretation of their scoring systems. Despite this limitation the DASH has received the best ratings for its clinimetric properties [4].
Previous research has attempted to present the clinical staging of FSCS according to either clinical presentation, histological biopsies and or arthroscopic findings [15, 32] but when combined permit a more expanded clinical staging scheme based on the hypothesis that correlations exist between the clinical stages and histological findings of FSCS (see Table 2).
Combined clinical staging of FSCS Neviaser et al. [32] and Faryniarz et al. (2012)
Combined clinical staging of FSCS Neviaser et al. [32] and Faryniarz et al. (2012)
At present the optimal treatment for FSCS remains elusive. Many conservative and invasive interventions have been described in the literature [26, 38]. Elective neglect, intra-articular cortico-steroid injections, heating and electrical modalities, manipulation under aesthetic, manual therapy, flexibility exercises and finally patient education have all been investigated with mixed results [22]. The capacity to achieve high level evidential support for a treatment modality has been hampered by an inability to clearly define the pathogenesis of the condition at a universal level. Consequently, poorly designed studies fail to capture the long-term effects of a treatment due to short term follow up protocols and failure to consider the presentation stage of the condition [26]. Presently there is strong level 1 and 2 evidence to support the use of intra-articular corticosteroid injection combined with shoulder mobility and stretching to produce short-term (4–6 weeks) pain relief and improved shoulder function [9, 45]. The estimated the economic burden due to FSCS is 4521 euro per patient of which 50% were due to absenteeism during the first quarter, amounting to 38% of the total physiotherapy working hours [19]. Elective or supervised neglect approach involves the conscious decision not to intervene conservatively or invasively but rather play a waiting game and let the FSCS reverse itself over time. Though this method may be viewed as controversial, elective neglect may have an economic saving when coupled with an effective patient educational program with improved outcome scores of 89% near-normal shoulder function (supervised neglect group) versus 63% (Stretching group) after 24 months follow up [13]. Patient education should include an accurate description of the stages of the disease and encourage early activity modification within the patients’ pain limits [22].
Joint mobilization techniques (level II evidence) and electrotherapeutic modalities such as shortwave diathermy (level II evidence), electroacupuncture (Level II evidence) and ultrasound (Level II evidence) are reported to have aided in the treatment of FSCS but the importance of their impact on improving functional outcomes remains weak (Grade C) as most studies are of a multi treatment design coupled with either flexibility or joint mobilizations versus no treatment [10, 17].
When conservative treatment fails manipulation under anaesthetic (MUA), arthrographic distension and capsular release are frequently the next stage of intervention-based treatment and within the United Kingdom are reported to range in cost from £425 (MUA) to £2511 (Capsular release) despite weak evidential research to substantiate their implementation [26].
Conclusion
Frozen Shoulder Contracture Syndrome is a condition in which the shoulder is stiff, painful, and has limited motion in all directions. It is a challenging disease to classify and treat optimally due to the multistage presentation and timing of its physical symptoms. Due to its presentation during the mid-fifties age bracket it is commonly referred to as “The Fifty-Year Shoulder”. It is unclear what the most effective treatment is to reverse its clinical presentation. There may be short term benefit for patients with FSCS, of less than six months, to receive a corticosteroid injection prior to the implementation of a home-based rehabilitation program consisting of low grade flexibility exercises. There is poor quality research to support the continuing use of electrotherapeutic modalities, manual therapy and surgical intervention in these patient populations, yet they are ongoing at a cost to the exchequer. At present there are clearly gaps in our knowledge and understanding of the pathogenesis of FSCS. Future research in this area should be designed around a universal classification system with randomised patient groups receiving a concise package of care measured by appropriate patient recorded shoulder outcome measures.
Conflict of interest
None to report.