
Abstract
PURPOSE:
The primary aim of this study was to determine the feasibility of conducting a randomised controlled trial (RCT) to evaluate the effectiveness of kinesiology tape (KT) and usual care versus usual care alone in the treatment of breast lymphoedema (BLE).
METHODS:
Fourteen participants with BLE were randomly assigned to either the KT and usual care group or usual care alone group. Both groups received three sessions of manual lymphatic drainage (MLD) once per week for three weeks, with the KT group additionally wearing the KT for two seven-day periods in between MLD sessions. Safety and acceptability of the KT were assessed by recording adverse events, skin changes and compliance with KT. Outcomes included were: ease of recruitment, attrition and acceptability of KT, percentage breast tissue water, patient-reported breast heaviness/fullness, breast discomfort and breast redness.
RESULTS:
Recruitment for this study was an average of 2.8 participants per month. There were no dropouts from either group. No adverse events or major skin side effects were recorded in either group. Minor skin redness was the most common dermal change (n = 5). Compliance with KT was excellent. Percentage tissue water in the worst affected breast quadrant reduced, on average, by 15.14% and 10.43% in both the KT group and the usual care group respectively.
CONCLUSION:
This feasibility RCT into the use of KT in BLE has shown that recruitment to a larger scale RCT is feasible. It has been demonstrated that KT is a safe and acceptable intervention with no adverse events and minor dermal changes. A large, multi-centred RCT is now necessary to accurately assess the effect of KT in BLE.
Introduction
Breast lymphoedema (BLE), sometimes termed breast oedema, is a lesser-known sequela of breast cancer treatments than upper limb lymphoedema. Like upper limb lymphoedema, BLE is an often chronic condition, characterised by swelling of the affected breast, which is perhaps not surprising as the breast and ipsilateral arm share the same lymphatic drainage routes [1]. BLE can be attributed, in part, to the growing number of breast-conserving (non-mastectomy) surgeries such as wide local excisions (WLE) and sentinel node biopsies (SLNB) performed each year [2]. The incidence of BLE has been reported in the literature as ranging from 0 to 90.4% across twenty-eight studies in a systematic review [3].
Lymphoedema of the breast causes problematic symptoms such as breast heaviness, redness and discomfort, with the latter symptom being reported in up to 69% of cases [4]. Indeed, in a survey by Gho and colleagues, bra discomfort was reported by 92.3% of participants who had lymphoedema [5]. Unlike upper limb lymphoedema, those with chronic BLE may experience severe pain and discomfort [6]. Pain due to severe tension of the lymphoedematous breast has also been documented in a case study [7]. BLE may also cause an unsatisfactory cosmetic appearance which can influence quality of life (QoL) [3]. Indeed, due to increasing numbers of breast cancer survivors, unwanted side effects of treatment such as BLE are beginning to demand the attention of clinicians. However, there is a dearth of evidence specifically describing and quantifying the impact of BLE on quality of life. Linnit and Young explored the psychological impact of BLE and noted its negative impact on family relationships as women reported fear of holding their children too close ‘in case they knock it’ and reported feeling too embarrassed to get close to their partners [8].
Certain risk factors for the development of BLE have been identified in the literature. Recently, axillary surgery is noted as a primary risk factor for BLE [9, 10] and incidences of 70% and 79% have been reported in those who have had axillary node clearance (ANC) surgery and radiotherapy to the affected breast [11, 12]. Increased body mass index (BMI) and upper outer quadrant tumour site were found to correlate with BLE in a study by Goffman and colleagues [13]. A bra cup size of ‘C’ or more was reported to be a further risk factor [10, 14]. Radiotherapy dose of ≥40 Gy has also been stated to increase breast volume [15]. Recipients of a photon boost, in a study by Keleman et al, were significantly more likely to develop breast oedema than those who received an electron boost (p < 0.005) [16].
In contrast to the uncomplicated circumferential measurements of upper limb lymphoedema using a tape measure, the clinical assessment of BLE in everyday practice is more difficult. Owing to the lack of availability of objective measurement tools for BLE, clinicians have had to rely on observation [4, 13] clinical photography [17] or patient self-report [6, 18]. Objective measures such as bioimpedance [19] and ultrasound [11] have been investigated but are not widely available in smaller centres. A relatively novel method of assessing local tissue water/swelling is the Moisture Meter-D (MMD) (Delfin Technologies Ltd, Finland) [20]. This tool, which transmits an electromagnetic wave of 300 MHz into an open-ended coaxial probe, is used to non-invasively measure skin and upper subcutis tissue dielectric constant (TDC) [21]. TDC is directly proportional to tissue water content and so a percentage water reading can be read from the screen. A study by Johansson and colleagues defined breast oedema as a TDC ratio exceeding 1.4:1 between the affected and healthy breast [22]. In practice this means that the tissue water in the affected breast skin and upper subcutis is 40% higher than in the contralateral breast. A compact version of the MMD, the Moisture Meter-D Compact (MMDC), is now being used in clinical practice [23]. It is a hand-held unit with a display showing percentage water rather than the TDC values directly [24]. There has been extensive research into TDC as an outcome measure in lymphoedema [19, 26] including reliability in upper limb lymphoedema [19, 24]. There has also been validation of the MMD to assess changes of tissue water in skin and subcutaneous fat [27]. There are no reliability or validity studies on the MMDC in BLE.
A combined treatment approach for BLE typically includes skin care education, a type of gentle massage, manual lymphatic drainage (MLD) and the use of compression bras [28]. A type of medical tape called kinesiology tape (KT) has gained popularity in the treatment of BLE in the past number of years [8]. Kinesiology taping, commonly called K-taping, was first developed in Japan in the 1970 s by Dr Kenzo Kase, with the treatment being introduced to Europe in the late 1990 s [29]. It is theorised that this form of taping reduces local swelling and pain and improves muscle activity in lymphoedema [1], especially in the management of truncal oedema where treatment options are more limited [30].
The evidence for the use of KT in lymphoedema is limited. Two recent systematic reviews [31, 32] that included seven lymphoedema studies reported that there was ‘inconclusive evidence’ to support the use of KT in the management of lymphoedema. Gatt et al. [32], in a meta-analysis, compared KT to compression bandaging/garments for upper limb lymphoedema. From the pooled data of five studies these authors concluded that there was no significant difference between KT and compression bandaging/garments in terms of limb volume [Weighted Mean Difference (WMD) –205.33 mL, Confidence Interval (CI) (–454.69 to 44.04) P = 0.11]. No randomised controlled trials (RCT’s), have been identified that examine the use of KT in BLE. Case reports on KT for the treatment of upper limb lymphoedema in three patients showed reduction in excess limb size and reduction in symptoms including fullness, tightness and discomfort [33]. A single centre non-randomised trial highlighted the safety of KT and increased functionality of the upper limb (p < 0.001) post KT intervention but no significant reduction in limb volume [34] Finnerty and colleagues note the relatively inexpensive nature of a roll of KT in the management of breast and truncal swelling when compared to compression garments [1]. The need for a fully-powered RCT is evident, however, before a large-scale study can be done a feasibility RCT should be conducted [35]. The aim of a fully powered RCT would be to assess the effectiveness of KT in the management of BLE. However, the primary objective of this feasibility RCT was to explore the feasibility of the recruitment of outpatients with BLE to a single centre. Secondary objectives included: 1. determining the safety and acceptability of KT by questioning of participants and reporting any adverse events post intervention; 2. investigating the utility of the MMDC as a diagnostic indicator of BLE at eligibility screening and as an objective measure of breast swelling and 3. conducting a preliminary analysis of the data to identify potential treatment effects of KT within and between groups.
Methods
Ethical approval
Ethical approval for this study was obtained from both the Institute of Nursing and Health Sciences Research Governance Filter Committee, Ulster University and the Clinical Research Ethics Committee, Cork University Hospital. Information leaflets were given to all participants and written informed consent was obtained from all participants included in the study. All procedures performed in this study involving human participants were in accordance with the ethical standards of the aforementioned institutional research committees and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Study design
This study was a single-centre feasibility RCT comparing KT and usual care to usual care alone in the management of BLE. One therapist treated the KT group and a different therapist treated the usual care alone group, to ensure continuity. Both groups received three sessions of MLD for twenty minutes, once per week, for three weeks, with the KT group additionally wearing the KT for two seven-day periods in between MLD sessions. A blinded independent assessor carried out baseline measurements at Visit 1 and follow-up assessments immediately post treatment (Visit 4) and six weeks post treatment (Visit 5) (Fig. 1).

Study timelines.
Participants were recruited from consultants, breast care clinical nurse specialists (CNS’s) and lymphoedema therapists within the hospital. Existing patients with BLE within the lymphoedema service were screened and informed of the study by post, by therapists independent of the study. Recruitment posters for the study were also placed at various locations within the hospital to allow self-referral.
Eligible participants were adults aged 18–80, with unilateral breast disease, who were at least six weeks post breast surgery including SLNB/WLE and/or ANC, at least four weeks post radiotherapy to the affected breast and who were willing to travel to the centre five times throughout the study. It was decided not to have an upper limit on time since breast surgery to maximise recruitment. Participants were also required to have BLE as defined by a ratio of ≥1.1:1% tissue water between the affected and unaffected breast, in at least one breast quadrant, measured by the MMDC. Patients were excluded if they had undergone previous mastectomy/bilateral mastectomies, had KT to the affected breast in the three months preceding the study, were allergic to KT (subject to patch test), were pregnant, were on antibiotics for the treatment of cellulitis, were cognitively impaired, had stage IV cancer/widespread metastatic disease or had a breast reconstruction without nipple reconstruction.
Setting
The trial took place in the regional cancer centre of a university hospital in the south of Ireland.
Procedure
Participants who confirmed an interest in taking part in the study were screened for eligibility by the independent assessor at Visit 1. The MMDC was used to confirm the presence of BLE. If eligible, participants were provided with a 2 cm×2 cm square of KT. Participants were instructed to put the patch of KT on the healthy breast 24 hours before Visit 2.
Randomisation
Randomisation occurred after a cooling-off period of one week. Participants were randomised by an independent therapist using a computerised random number sequence (generated by the independent therapist), which determined the participant allocations to either KT or usual care group, in groups of four [36]. The independent therapist was unaware of the size of the blocks.
Interventions
The intervention group received KT and usual care. Usual care management of BLE included skin care education, MLD and information on how to obtain compression bras. KT was applied to cover all the affected breast in a criss-cross pattern, from just below the inferior clavicle to the end of the breast and as far as the lateral edge of the sternum on Visit 2, in 1.25 cm wide strips. This was done by an experienced senior physiotherapist trained in KT for lymphoedema, taking care to avoid the nipple with the tape.
KT was applied on Visit 2 and reapplied on Visit 3. Participants were asked to leave the KT on the affected breast for these two seven-day periods, if comfortable and to remove the KT independently on the morning of Visits 3 and 4. This protocol is based on that of Finnerty and colleagues in their audit on the use of KT for breast oedema [1]. On Visit 4 participants received MLD alone.
The control group received the exact same usual care as the intervention group, without the application of KT.
Outcome measures
Primary outcomes
2.8.1.1 Feasibility of recruitment to intervention. The number of participants suitable for recruitment and the number of actual volunteers was recorded. Any differences in retention between the control and the intervention groups were also noted.
2.8.1.2 Safety and acceptability of KT in BLE. The safety of the KT was identified by the detailed recording of any adverse events to both patch testing and KT intervention group. This included dermal changes such as peeling skin, skin lesions/blisters, redness and broken skin in the affected breast [34]. Participants were instructed to remove the tape immediately if any visual or sensory irritation occurred. Participants were also free to remove the tape before the seven-day intervention period was complete, if uncomfortable. Adverse events were recorded weekly by the treating therapist to ensure the assessor remained blinded.
Acceptability of the KT was investigated via standardised questioning of the participants on Visits 3 and 4 and by monitoring compliance during the intervention period. Standardised questioning included three questions on the comfort of the tape, effect on skin and whether the participant had any concerns about the tape while in place. Compliance was monitored by recording the number of days for which the tape was worn and the reason(s) for removing the tape.
Secondary outcomes
2.8.2.1 Percentage tissue water (Breast swelling). The MMDC measures TDC in the skin and subcutis non-invasively and locally in a few seconds. The TDC is converted into water percentage on a scale from 0 to 100% and is displayed on the LCD screen [23]. The breast was divided into four quadrants, using a skin-friendly marker, the edge of a laminated card and the nipple as the mid-point and the MMDC probe was placed in the middle of each quadrant. The edge of the probe lay 1 cm from the areola as per procedure described by Johansson et al. [22]. The same device was used for all tests.
To determine eligibility for the trial the assessor repeated the above procedure for both the healthy and affected breast in the same subject. A ratio of ≥1.1:1 between the affected and healthy breast in any one quadrant was used as an indicator of BLE. This is lower than the ratio of ≥1.4:1 by Johansson and colleagues [22] to include those with even mild breast swelling into the study. Any positive or negative practical issues related to the use of the MMDC were recorded by the independent assessor.
2.8.2.2 Patient-reported outcomes. Breast heaviness/fullness, discomfort and redness were assessed on 10 cm visual analogue scales (VAS) [6, 37].
Statistical analysis
Descriptive statistics were used to present baseline data, e.g. percentages for nominal variables (e.g. affected breast) and means and standard deviation (SD) for continuous variables (e.g. % tissue water, VAS). The mean % tissue water in the affected breast, the worst affected breast quadrant for both groups and the VAS scores at baseline, post-treatment and at six-week follow-up are presented graphically. Statistical Package for the Social Sciences (SPSS) software, Version 23.0.0 was used to analyse data and graphs were formulated using Microsoft Excel software.
Results
All the participants were female and the average age was 59 years (range from 34 to 74). Table 1 shows detailed demographic and clinical data for both groups.
Comparison of participant details in the KT group and the standard care group.
Comparison of participant details in the KT group and the standard care group.
WLE = Wide local excision; ANC = Axillary node clearance; SLNB = Sentinel node biopsy; BMI = Body mass index; Gy = Gray
Seventeen participants were screened for eligibility, three were excluded (two did not meet the ≥1.1 ratio of BLE required and one did not have a nipple on the affected breast). Therefore, fourteen participants were randomised to either the KT or usual care group, each group having seven participants (Fig. 2).
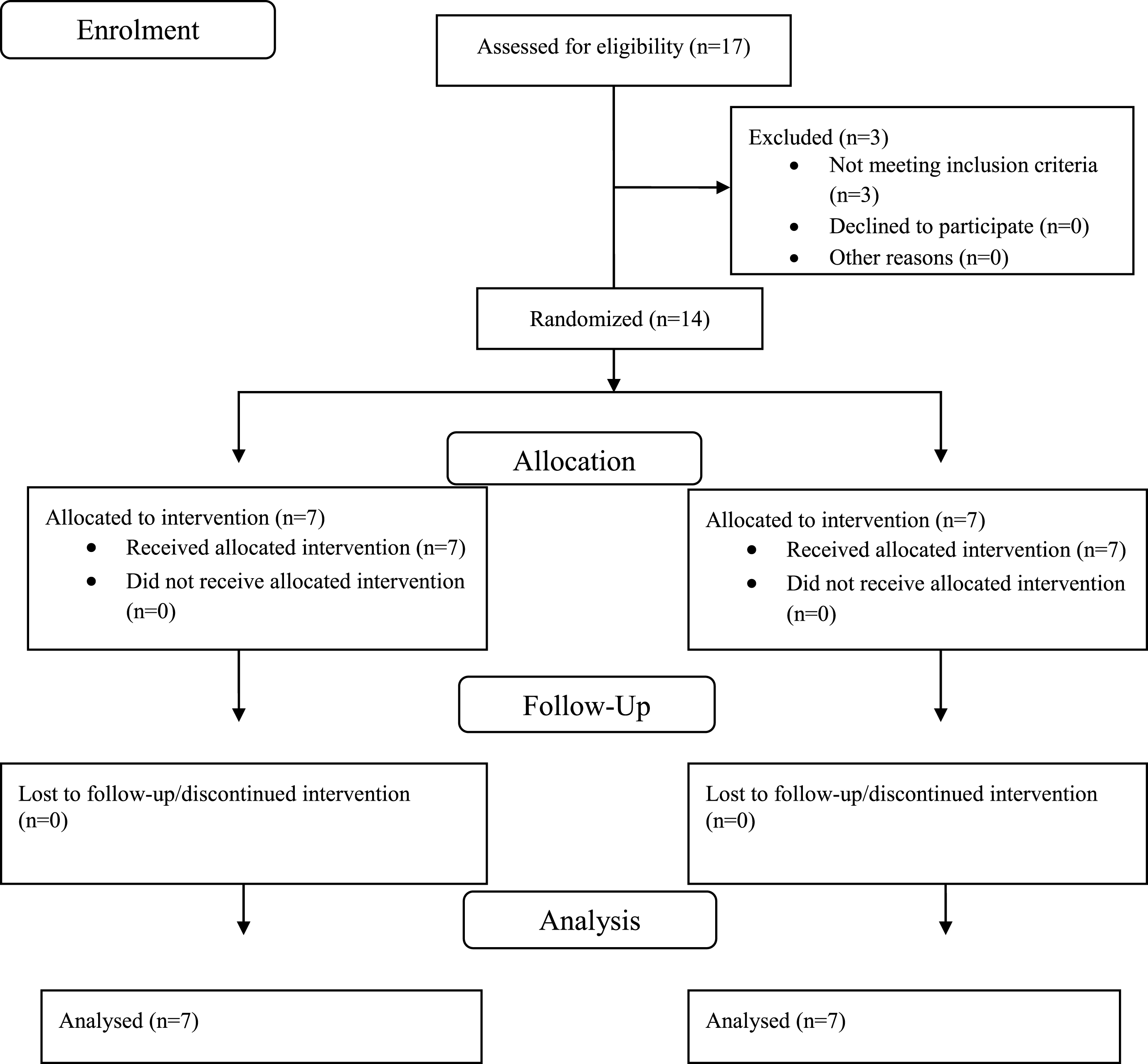
Consort flow diagram for trial.
Of the seventeen people assessed for eligibility over the five-month recruitment period, fifteen were recruited from lymphoedema therapists within the hospital who invited existing patients of their service for eligibility testing. Two were recruited from breast care CNS’s within the hospital. No patients were recruited from consultants or by self-referral from study posters. The average recruitment rate was 2.8 participants per month. There were no differences in retention between the intervention and control groups, with no dropouts from either group.
Safety and acceptability of kinesiology tape
There were no adverse events in either the KT group or usual care group. There were no adverse reactions to the patch testing, therefore all the participants who were patch-tested took part in the intervention group. There were no major skin side effects. Skin redness was the most commonly reported dermal change amongst the intervention group (n = 5). One of the participants had to remove a small portion of tape from the superior part of the breast because of a small blister (∼2 mm) on day five of the second week. This resulted in a small area of broken skin which closed over after one day.
Five out of the seven participants in the first week and six out of the seven participants in the second week wore the tape continually, with no difficulty. The remaining participants noted some irritation and mild itchiness where the KT was loosening at the edges at day six of each week and removed these small sections. Overall KT compliance was 95 out of 98 potential days of usage (96.9%). Five out of the seven participants reported the KT to be comfortable while in place, with three stating that it felt supportive at the breast. Those that reported the tape to be uncomfortable found this to be so toward the end of the seven-day period when the tape began to loosen.
Moisture MeterD compact
The MMDC was found to be a user-friendly, useful instrument to assess and quantify breast swelling. All fourteen participants in this study recorded a ratio of ≥1.4:1 between the affected and healthy breast in at least one breast quadrant.
Percentage tissue water
The worst affected/most swollen breast quadrant for thirteen out of fourteen participants was either of the dependent quadrants at the lower section of the breast. The average percentage swelling in the worst affected breast quadrant for the KT group was 65.57% (±12.67) and for the usual care group was 69.43% (±8.73). Both the KT group and the usual care group showed improvements in breast swelling immediately post treatment with average reductions of 15.14% and 10.43% respectively in the most affected quadrant. However, though improvements had been lost for both groups at six-week follow-up, swelling had not yet returned to baseline levels (Fig. 3).
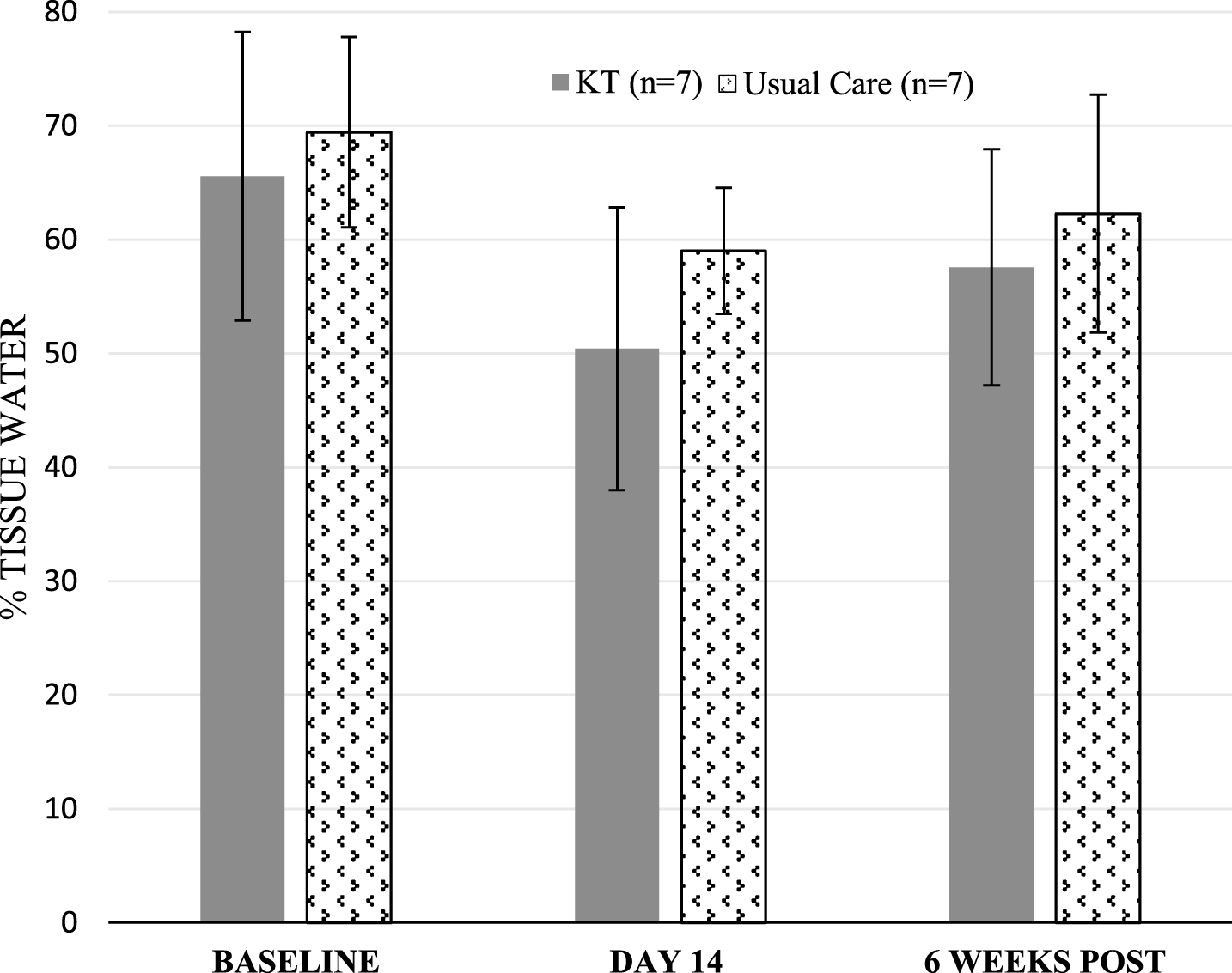
Mean % tissue water in the worst affected breast quadrant. Error bars displayed denote standard deviation (SD).
The total average breast swelling in the affected breast for the KT group at baseline was 49.54% (±6.71) and for the usual care group was 57.79% (±8.53). Total breast swelling in both groups had reduced immediately post treatment by an average of 4.61% and 4.04% respectively. Again, total average breast swelling had increased at six-week follow-up but had not returned to baseline levels (Fig. 4).
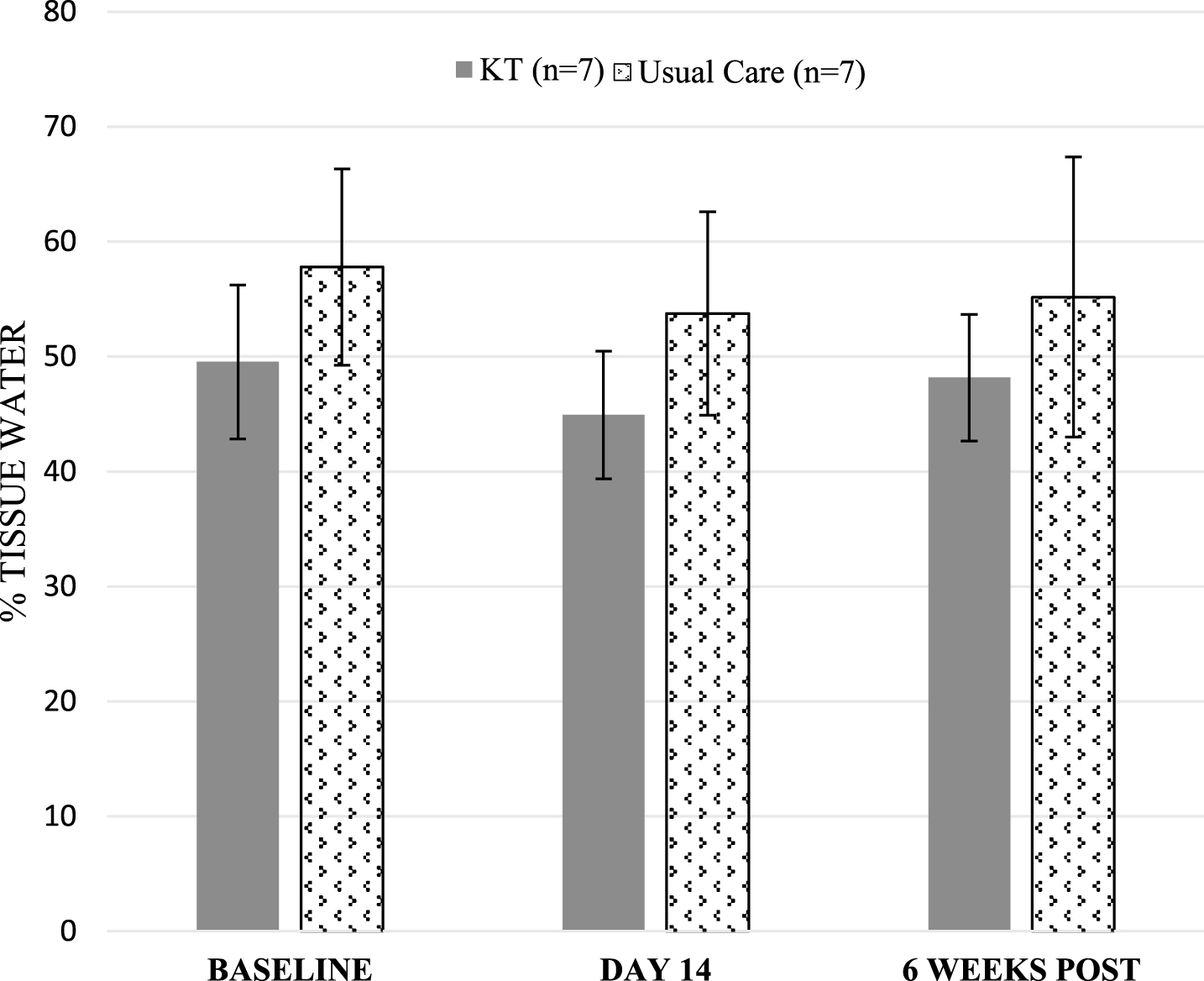
Mean % tissue water (breast swelling) in the whole affected breast. Error bars displayed denote standard deviation (SD).
Patient-reported breast heaviness/fullness decreased on average for both groups from baseline to immediately post-treatment (1.23 in KT group and 0.53 in usual care group) and were higher than baseline levels at six-week follow-up. Self-reported breast discomfort reduced on average by 3.47 and 1.76 for the KT and usual care groups respectively, from baseline to immediately post treatment. However, these average VAS scores had not returned to baseline levels at six-week follow-up. Participants in both groups did not rate breast redness as a problematic symptom with average scores ranging from 0.42 to 1.51 (Table 2).
Mean VAS scores for KT and Usual Care Group including standard deviation (SD)
Mean VAS scores for KT and Usual Care Group including standard deviation (SD)
The primary aim of this study was to examine the feasibility of conducting an RCT to evaluate the effectiveness of KT and usual care versus usual care alone in the treatment of BLE, including issues surrounding patient recruitment, safety and acceptability of KT and outcome measurement. Considering incidences of up to 90.4% for BLE have been reported in the literature [3], the recruitment rate of 2.8 participants per month for this feasibility study was relatively low. Potential reasons for this are that in busy clinics, diagnostic evaluation of lymphoedema is largely focused on the upper limb [6] and information on the assessment and treatment of BLE is lacking [38]. All the participants in this study reported breast discomfort as a problem. Therefore, the targeted direct recruitment of participants via breast cancer support organisations, with greater emphasis on breast discomfort, may yield larger numbers for eligibility screening and thus a higher recruitment rate.
This is the first feasibility RCT to explore the safety and acceptability of KT in BLE. Previous RCT’s have explored effectiveness and safety issues related to KT [37, 39–42] and one non-randomised trial examined the safety of KT [34]. However, these studies focused on upper limb lymphoedema only. While there were no dropouts from the KT group in the current study, previous studies have reported attrition rates of 10–21% because of dermal problems and allergic skin reactions to KT [32]. The risk of allergic reaction to KT was mitigated in this study by patch testing the breast tissue for 24 hours.
Wound formation was noted as a side effect in one pilot study, however details of the location, type and extent of wounds from KT were not described [37]. The authors reasoned that removal of KT is a two-handed activity and participants removed the tape by themselves at home with the unaffected arm. In the current study, a 2 mm blister was the worst dermal change noted on day 12. The KT was removed safely by each participant as they had two free hands. Intervention time for the pilot study should also be noted: five times per week for four weeks [37], which is more intensive than the current study. This may also account for the high level of wound formations.
An audit on the use of KT for breast oedema, with ten participants, provides some useful comparisons with the current study as intervention times for KT were the same [1]. In the audit four participants reported a slightly pink colour to the breast when the tape was removed, while in the current study the incidence of skin changes was higher at five out of seven participants. Mild itchiness was reported at the edges of the tape, where it was loosening, by two participants at day six, a result that was reflected by one participant in the audit [1]. Shortening the treatment period to five instead of seven days in a future RCT may offset this mild dermal change. Compliance was excellent in the current study at 96.9%, with all participants able to wear most of the KT for the two seven-day application periods. Compliance with KT in the audit group, while stated to be recorded with questionnaires, was not discussed in the results [1].
A strength of this study was the use of an objective measurement tool, the MMDC, to quantify BLE. The lack of good quality research into interventions for BLE may be, in part, due to the absence of objective measures. This over-reliance on subjective measures has served as a limitation in previous studies of BLE [1, 43] and as a barrier to the effective management of BLE in clinical practice. While extensive work has been completed to validate MMD (the predecessor of the MMDC) further studies are needed into the reliability and validity of the MMDC. This feasibility study has demonstrated its usefulness in clinical practice as a quick, portable, non-invasive measure of tissue swelling of the breast, which to date, has been difficult to measure objectively. The TDC ratio of ≥1.4:1 between the affected and healthy breast suggested by Johansson et al. [22] appears to be a good indicator of BLE in this study, with all participants reaching this ratio in at least one quadrant of the breast. In this study, the most swollen breast quadrant in thirteen out of the fourteen participants was either of the lower, dependent quadrants of the breast. This occurrence has been noted elsewhere [4, 44].
While the primary aims of this study are to assess the safety, feasibility and acceptability of KT in BLE, preliminary results suggest that swelling in the worst affected quadrant and in the total affected breast tended to improve with both interventions and at six-week follow-up had not returned to baseline levels. This is a welcome result for patients with BLE, who also reflected this in their breast discomfort VAS scores. Educating patients with BLE on regular simple lymphatic drainage (SLD) of the breast (a type of self-MLD), may help to maintain the reductions in breast swelling for longer. A future RCT would be enhanced by inclusion of same, with compliance logs recorded by the participant at home.
In this single-centre study, the decision not to have an upper limit on time since breast surgery was taken to maximise recruitment. This meant participants ranged from 3.5 months to 11 years post-op. Therefore, those who were longer since surgery may have had more chronic lymphoedema. In a potential future multi-centre trial, an upper limit of 2 years post-op may see greater improvements for BLE interventions. However, even the participant who was 11 years post-op showed improvements in percentage tissue water and VAS scores. This indicates that even chronic BLE is treatable.
Limitations of this feasibility study include small sample size (n = 14). Due to time constraints, a five-month recruitment period was the maximum achievable. Efforts were made to capture participants’ experiences of the interventions by VAS scores, however no QoL outcome measurements were used. QoL measures such as the European Organisation for Research and Treatment of Cancer (EORTC) questionnaire or the SF-36 have been used in KT studies in the past [32]. Data on QoL of those with BLE is scarce and a future RCT would be enhanced by inclusion of QoL measures. The therapist carrying out the KT intervention recorded any adverse skin changes. This is a potential source of bias and would have been mitigated by the independent assessor recording these changes. Unfortunately, due to limited resources, this was not possible in this feasibility study.
This feasibility RCT into the use of KT in BLE has shown that recruitment to a larger scale RCT is feasible, although alternative strategies may be required to maximise recruitment such as focusing on patient support groups and extension of the five-month recruitment period. In this novel study, we have shown that KT is a safe and acceptable intervention with no adverse events other than minor dermal changes. Objective measurement of BLE by use of the MMDC has strengthened the results of this study but its reliability and validity has yet to be determined. A large, multi-centred RCT, which could include a component on MMDC reliability and validity, is now necessary to accurately assess the effect of KT in BLE
Conflict of interest
None to report.
Footnotes
Acknowledgments
A research bursary was awarded by the Southern Branch of the Irish Society of Chartered Physiotherapists, St. Stephen’s Green, Dublin 2, Ireland. The authors would also like to acknowledge the help of Gay Castles, Deputy Physiotherapy Manager, Cork University Hospital; Helen Murphy, Senior Occupational Therapist, Cork University Hospital; Dr Norma Relihan, Senior Lecturer in Breast Diseases, Cork University Hospital and Dr Darren Dahly, Principal Statistician and Senior Lecturer in Research Methods at Health Research Board Ireland, Clinical Research Facility, Cork.