
Abstract
BACKGROUND:
Immediate rehabilitation is increasingly used for tendon injuries, but complete single-leg heel raise recovery after injury remains uncommon.
PURPOSE:
This study primarily determined if immediate versus traditional rehabilitation resulted in better single-leg heel raise recovery against the physiological reference, and compared performance recovery against the non-injured limb. The study also explored if clinical parameters at 4, 8, and 12 weeks post-tenorrhaphy are predictors of more single-leg heel raises at week 12 in recreational soccer players.
METHOD:
Twenty-six amateur soccer players (43.2±10.1 years-old, BMI 29.5±3.9 kg/m2) underwent rehabilitation using early or traditional rehabilitation following Dresden tenorrhaphy of the Achilles tendon. The main outcome was the single-leg heel raise repetitions.
RESULTS:
Immediate rehabilitation resulted in significantly more single-leg heel raises than traditional rehabilitation (p < 0.001). Performance capacity compared to the physiological reference was significantly greater for immediate rehabilitation (p < 0.001) but significantly lower for traditional rehabilitation (p < 0.001). Only immediate rehabilitation recovered single-leg heel raise capacity as compared to the non-injured limb (p = 0.217). The beta coefficients for weight and dorsiflexion range of motion at week 12 were respectively – 0.81±0.25 and 1.86±0.61.
CONCLUSIONS
Immediate AT tenorrhaphy rehabilitation more quickly recovers reference values and approximates non-injured-limb values for single-leg heel raise capacity after a 12-week physical therapy program. Dorsiflexion range of motion at week 12 and weight were predictors for more single-leg heel raise repetitions at week 12.
Introduction
Two of the most frequent complications resulting from tenorrhaphy for Achilles tendon (AT) repair are the delayed and reduced ability to perform single-leg heel raises [1–6]. Traditionally, this ability has been measured through the single-leg heel raise test [1, 7–11], with post-operative performance deficits ranging between 12% and 48% a year after treatment [11, 12]. These deficits could potentially be modified by early rehabilitation programs [13–15], which introduce mobility and/or weight bearing within the first weeks after surgery [16, 17]. In contrast, traditional rehabilitation programs do not introduce mobility and weight bearing within the first weeks to protect the repairs made through AT surgery [17].
The single-leg heel raise test is defined as repeated concentric and eccentric monopodal movements of the plantar-flexor mechanism. Specifically, the knee is kept extended; balance is assisted by a single finger, and the patient performs the maximum possible range of ankle plantar-flexion with the goal of achieving the greatest displacement of vertical central body mass [9]. The single-leg heel raise test is one of the most important clinical tools for assessing plantar-flexor strength following tenorrhaphy of the AT and is a clinical approximation of the repetitive behavior performed by the plantar-flexor mechanism during different daily motor tasks [1]. This simple test for detecting a deficit in plantar-flexor strength [10] has adequate validity and reliable, with an interclass-correlation coefficient between 0.78 and 0.85 [1]. Lundford & Perry [9] described the following normal parameters for the single-leg heel raise test in a population aged 27.9±11.1 years-old: between 26 and 30 repetitions to obtain a confidence interval of 99%; a range of 6 to 70 repetitions; an arithmetic mean of 25 repetitions; a median of 26 repetitions; and a mode of 29 repetitions [9]. Nevertheless, other authors have determined that, in a sedentary population and starting at 20 years-old, there is an inverse relationship between age and the number of repetitions, with an average of 20 repetitions serving as a reference for adults [18]. These referenced disparities were identified in a systemic review by Herbert-Losier et al. [7], who did not determine any final normal values. Nevertheless, the mean of 25 repetitions described by Lunsford & Perry [9] was accepted as a clinical approximation in the adult population [7].
Considering that the ability to perform a single-leg heel raise is commonly not recovered following AT tenorrhaphy [2–5], a number of authors have explored diverse factors associated with functional recovery after 6, 12, or more months [1, 19]. Moreover, the initial 12 weeks post-surgery have been described as the principal therapeutic window to obtain neuromuscular changes in the triceps-surae [15, 20], which is in conflict with the traditional rest period proposed by rehabilitation programs following AT tenorrhaphy [17, 21]. It was recently found that immediate AT tenorrhaphy rehabilitation (i.e., one day post-surgery) with introduced controlled weight bearing and mobilization achieved better medial gastrocnemius junction displacement after 12 weeks of training than did a traditional rehabilitation approach [22], but non-differences between isometric plantarflexion strength in a neutral position were found between these rehabilitation strategies [17]. These findings cast doubt on if better superficial muscle displacement improves plantar flexion strength, i.e., single-limb heel raise capacity. Unfortunately, early weight bearing and mobilization could have devastating clinical results, such as re-rupture and tendon lengthening due to excessive AT traction [6, 23]. As demonstrated, there is a lack of consensus regarding if immediate AT tenorrhaphy rehabilitation (i.e., controlled weight bearing and mobilization from day one post-surgery) results in an early ability to perform single-leg heel raises, recovery of the Lunsford & Perry’s [9] reference, or recovery in the non-injured leg to perform single-leg heel raises. Agreement is also absent as to the clinical parameters that could best predict performance in the single-leg heel raise test over a 12-week rehabilitation program following tenorrhaphy of a mid-substance AT rupture.
Due to the current status of this subject, the primary aim of this study was to determine if immediate rehabilitation results in the ability to perform single-leg heel raises earlier than traditional rehabilitation after AT tenorrhaphy. Additionally, secondary aims were to determinate if immediate and traditional rehabilitation programs recover the physiological reference for single-leg heel raise capacity, the single-leg heel raise capacity is recovered in the non-injured limb with immediate and traditional rehabilitation programs, and clinical parameters at 4, 8, and 12 weeks post-percutaneous tenorrhaphy of the AT are predictors of more single-leg heel raises at week 12 of rehabilitation (i.e., age, weight, body mass index [BMI], injury-surgery interval, isometric strength, AT total rupture score, calf circumference, difference between calf circumferences, dorsiflexion range of motion, difference between dorsiflexion ranges of motion, and visual analog scale for pain [VAS pain]). The hypotheses of this study were immediate rehabilitation would have a lower mean for single-leg heel raise repetitions at week 12 as compared with traditional rehabilitation after AT tenorrhaphy, immediate and traditional rehabilitation programs would generate a mean single-leg heel raise capacity lower than 25 repetitions, mean single-leg heel raises capacity would not be recovered in the non-injured limb, and predictive clinical parameters of more single-leg heel raises at 12 weeks post-rehabilitation would not be found at 4, 8, and 12 week post-tenorrhaphy of the AT.
Material and method
Study design
This was a randomized prospective study in amateur soccer players treated with unilateral percutaneous tenorrhaphy of the AT [22, 23]. Two rehabilitation groups were compared to evaluate the first three hypotheses. To investigate the fourth hypothesis, both rehabilitation groups were included in a regression model to determine the predictors of single-leg heel raise success one year after AT tenorrhaphy, as described in Bostick et al. [1] and Olsson et al. [11].
All of the participants underwent a 12-week rehabilitation program, with half following an early rehabilitation program and half following a traditional rehabilitation program. The study was carried out from 2014 to 2016 in the Biomechanics Unit of the Instituto Traumatologico (Santiago, Chile). Each participant provided written consent to be included in the study. This study was approved by the institutional review board of the Instituto Traumatologico (Santiago, Chile), in accordance with the Declaration of Helsinki.
Participants
Twenty-six amateur soccer players (Table 1) with a mid-substance AT rupture were treated by percutaneous tenorrhaphy using the Dresden procedure [17, 23]. All participants met the established eligibility criteria. The inclusion criteria were i) aged between 30 and 55 years old, ii) Achilles rupture during soccer practice, iii) Dresden repair procedure [22, 23], iv) history of intermittent exercise routine (>30 minutes of physical therapy, one or twice per week), v) first Achilles tendon injury, vi) mid-substance rupture, vii) injury-surgery interval≤ten days, viii) rehabilitation at Instituto Traumatologico (Santiago, Chile), and ix) physical therapy sessions three times per week. The exclusion criteria were i) history of tendinous injuries, ii) history of autoimmune diseases, iii) history of traumatic lower leg injury, iv) orthopedic alteration of lower leg, and v) steroid therapy dependence.
Basal patient characteristics
Basal patient characteristics
Standard deviation (sd), Body mass index (BMI).
The sample size was estimated “a priori” employing a large effect size of 1.01 [17], alpha error probability of 0.05, statistical power probability of 0.80, allocation ratio of 1 and 20% of dropout using G*Power software (version 3.1.9.2; Universitat Dusseldorf, Dusseldorf,, Germany). Initially, 39 patients were assessed for inclusion criteria being 9 patients excluded due history of traumatic lower leg injury. After that, 30 patients were allocated in one of two rehabilitations groups through simple randomization by 1 to 1 ratio. Four patients (13.3%) were dropout during the follow up due they did not assist to the rehabilitation after the fourth week (labor reasons). The numbers used to allocate patients were generated through computerised random number by Matlab software (Mathwork, inc, USA).
The same orthopaedic surgeon (H.H.) performed percutaneous tenorrhaphy on all patients using FiberWire Suture No. 2.0 (Arthrex Inc., Naples, FL, USA). A minimally invasive posteromedial incision (2 cm length) was made 3 cm above the proximal end of the tendon rupture. Special care was taken to preserve the paratenon by performing an aperture between the superficial fascia and Achilles paratenon. Through the aperture, two Dresden instruments were positioned at the lateral and medial borders of the distal tendon end, approximately 1.5 cm from the calcaneal tuberosity border. The first suture was passed distally from the medial to the lateral plane through the distal inner diameter of the Dresden instruments. A second suture was passed parallel to and 1 cm proximal to the first suture, from the medial to lateral plane through the proximal inner diameter of the Dresden instruments. Then, the instruments were pulled proximally until the suture ends appeared by the posteromedial incision. To check that the distal sutures were firmly placed, the medial and lateral sutures were pulled until achieving full ankle plantarflexion. The sutures were strained with enough tension to achieve resting contralateral plantarflexion. Finally, the sutures were tied with three simple knots [22].
Intervention
Two rehabilitations models were used, the immediate and traditional models as show the Table 2, and previously was detailed by De la Fuente et al. [17]. In summary, both rehabilitation models consisted of three phases of four weeks each one until the week twelve.
Rehabilitation models used in the study
Rehabilitation models used in the study
In the first phase (days 1–28), both patient groups received inpatient education of basic care and wound/tendon protection. The traditional-rehabilitation group was immobilized with fixed cam walker boot indicating no weight bearing for the first 28 days post-tenorrhaphy, and toe movement were gave to diminish the risk of thrombus as home exercises. In parallel, the immediate-rehabilitation group began physical therapy (three times weekly, 1.5 h each session) from day 1 post-surgery performing controlled range of motion exercises (mobilization in plantarflexion), gait training using crutches as tolerated based on pain and ankle inflammation with restriction of the dorsalflexion movement through articulated cam walker boot, and deep ankle muscle activation exercises without contraction of triceps surae [17]. In the first phase, all immediate-rehabilitation patients were treated by the same physical therapist in the biomechanics unit (C.F.).
The second phase (days 29–56) involved care education, tendon protection, controlled stretching, isometric and concentric strengthening, and gait training with crutches with weight bearing tolerated based on pain and ankle inflammation. All patients received physical therapy treatment (three times weekly, 1.5 h each session), with sessions administered in the physical therapy unit by the same, second physical therapist of the foot and ankle team (R.P.) [17]. Patients advanced from the first to the second phase if they could tolerate gait with crutches without experience of pain and secondary inflammation due weight bearing, could perform active plantar-flexion exercises, did not have a local infection, and had the wound suture removed [17]. All patients progressed without delay.
The third phase (days 57–84) incorporated principles of care education, stretching, and controlled eccentric and plyometric strengthening and gait training without crutches [17]. Immediate- and traditional-rehabilitation patients progressed from the second phase to the third phase if they could tolerate full weight bearing without crutches and could support a 1-legged plantigrade position, have been progressed all patients without delay [17]. All interventions were performed in the physical therapy unit by the physiotherapist of the foot and ankle team (R.P.).
Basal patient characteristics
Age, height, weight, BMI, and the injury-surgery interval (i.e., time between receiving the injury and surgical intervention) were recorded for all patients.
Single-leg heel raise capacity
The single-leg heel raise test considered the maximum number of heel lifts with the knee extended in a standing position [9]. The patients were allowed to use one finger to maintain balance, and the test was performed on a flat surface for one minute at the end of week 12 post-tenorrhaphy.
AT rupture score
The score was registered according to Nilsson-Helander et al. [24], with weeks 4, 8, and 12 of rehabilitation taken into consideration.
Calf circumference
Calf circumference was measured at weeks 4, 8, and 12 of rehabilitation at the widest point in the injured leg while in a bipedal posture, according to Saxena et al. [19].
Difference between calf circumferences
The absolute difference was calculated between the calf circumferences of the non-injured and injured legs at weeks 4, 8, and 12 of rehabilitation.
Dorsiflexion range of motion
Dorsiflexion range of motion was measured at weeks 4, 8, and 12 of rehabilitation in a supine position with 90° of knee flexion [16, 17].
Difference between dorsiflexion ranges of motion
The absolute difference was calculated between the dorsiflexion ranges of motion of the non-injured and injured legs at weeks 4, 8, and 12 of rehabilitation.
Isometric plantar-flexion strength
Isometric plantar-flexion strength was determined at weeks 4, 8, and 12 of rehabilitation with knee flexion at 90° and the ankle in a neutral position [16, 17]. Plantar-flexion strength was recorded by an S-type load cell (Intertecnology Inc., Toronto, Canada) at the metatarsal level [16, 17].
Difference between isometric plantar-flexion strengths
The absolute difference was calculated between isometric plantar-flexion strengths for the injured and non-injured legs at weeks 4, 8, and 12 of rehabilitation. The isometric plantar strength of the non-injured leg was measured seven hours prior to surgical intervention.
VAS pain
VAS pain was measured at weeks 4, 8, and 12 of rehabilitation by a numerical scale graded from zero to ten through (continuous scale in centimeters), with zero representing a lack of pain and ten a maximum amount of pain [16].
All measurements were performed in the biomechanics unit by the same physical therapist (C.D.).
Statistical analysis
Descriptive statistics were used to assess the recorded data, which were reported as the arithmetic mean±standard deviation. Normal distribution, the homoscedasticity of regression residuals, and independence were corroborated using the Shapiro-Wilk, Cameron & Trivedi’s decomposition, and Durbin-Watson tests, respectively. To compare the means of single-leg heel raises between groups and to assess the null-hypothesis (i.e., H0: μtraditionalgroup > μimmediategroup), a one-tailed, non-paired t-test was used. To compare the means of single-leg heel raises against Lunsford & Perry’s reference and to assess the null-hypothesis (i.e., H0: μtraditionalgroup <25), a one-tailed, single-sample t-test was used. To compare the means of single-leg heel raises between groups and between injured/non-injured limbs, as well as to assess the null-hypothesis (i.e., H0: μnon - injured limb > μtraditional/immediategroup), a one-tailed, non-paired t-test was used.
To determine which independent variables were relevant for the model, univariate analysis was conducted on the following variables: age, height, weight, BMI, injury-surgery interval, AT total rupture score, calf circumference, difference between calf circumferences, dorsiflexion range of motion, difference between dorsiflexion ranges of motion, isometric plantar-flexion strength, difference between isometric plantar-flexion strengths, and VAS pain. Only those variables with an alpha level of 5% and an absolute correlation coefficient greater than or equal to 0.25 were considered, according to Bostick et al. [1] and Olsson et al. [11].
Phenomena of multicollinearity were corroborated with a variance inflation factor greater than or equal to 10 or a statistically significant (p < 0.05) lineal relationship determined by analyzing matrix dispersion (Fig. 1). For variables of multicollinearity, the model maintained the variable that obtained the greatest correlation coefficient in relation to the independent variable. Therefore, a predictive multivariate regression model was developed based on Y =β1X1+β2X2+ ... +βnXn, which was used to describe the determination coefficient of the regression, the adjusted determination coefficient, the β coefficients of the regression, standard deviation, and each confidence interval at 95%. All statistical analyses were performed using the STATA 12.0 software (Stata Corp., College Station, Texas, USA).
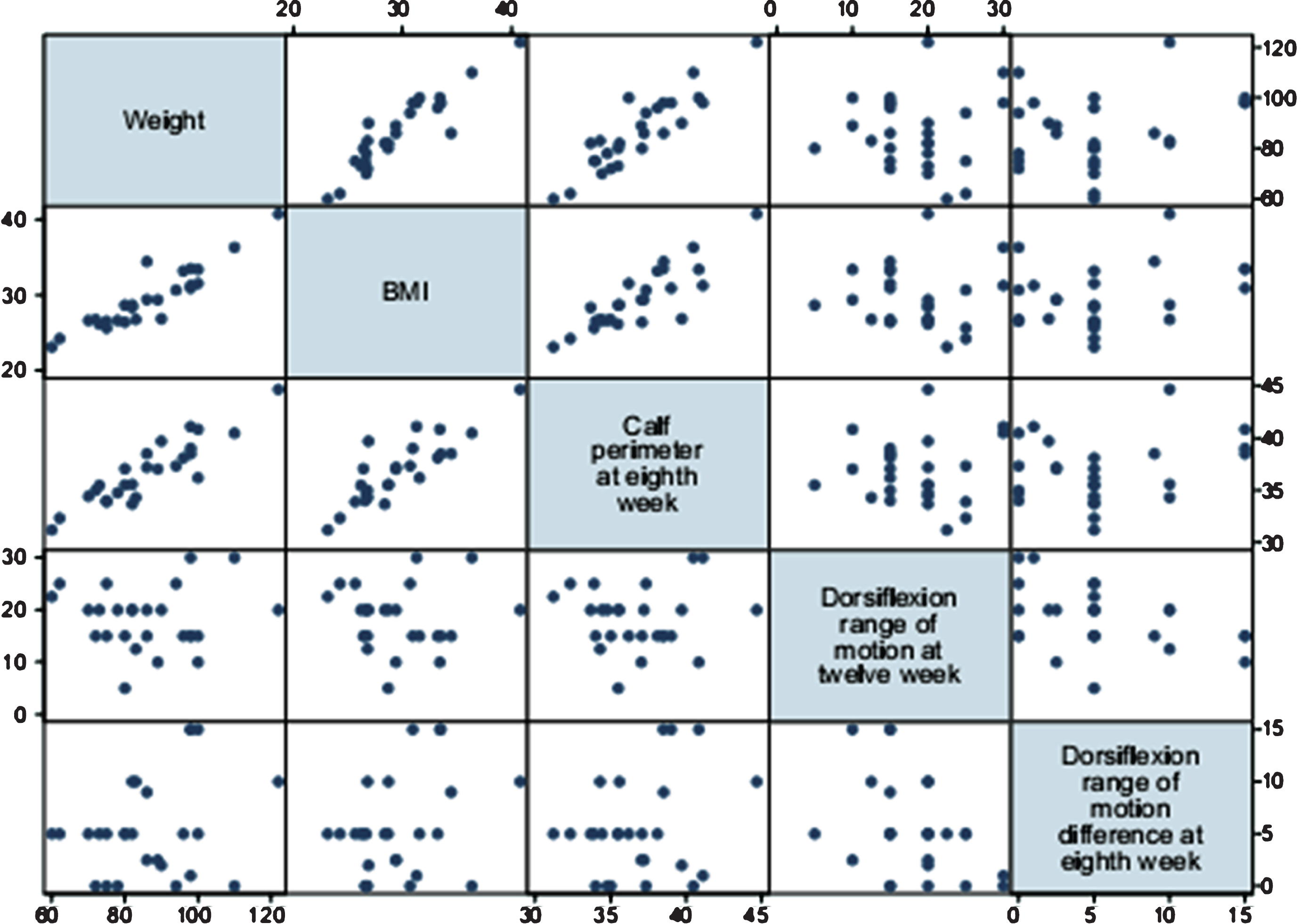
Multicollinearity analysis (matrix dispersion). BMI = Body mass index.
The basal characteristics of the patients are summarized in Table 1, while the variables of the study are summarized in Table 3. The immediate-rehabilitation group had significantly better single-leg heel raise performance (41.2±19.0 repetitions, non-patients (0/13) failed to recover the single leg heel rise) than the traditional-rehabilitation group (10.0±13.8 repetitions, p < 0.001, 54% (7/13) of patients failed to recover the single leg heel rise). Single-leg heel raise performance as compared to the physiological reference was greater for the immediate-reference group (p < 0.001), but lower for the traditional-rehabilitation group (p < 0.001). Single-leg heel raise capacity as compared to the non-injured limb was recovered for the immediate-rehabilitation group (p = 0.217) but not for the traditional-rehabilitation group (p < 0.001).
Clinical and Single-leg heel rise results
Clinical and Single-leg heel rise results
Standard deviation (sd), Body mass index (BMI), Achilles tendon rupture score (ATRS), Visual analog scale for pain (VAS Pain), Dorsal-flexion (DF), Traditional group (TG), Immediate Group (IG).
Weight, BMI, and calf circumference at week 8, dorsiflexion range of motion at week 12, and the difference between dorsiflexion ranges of motion at week 8 were statistically significant (p < 0.05) and presented an absolute correlation coefficient >0.25 in relation to single-leg heel raise capacity. Weight, BMI, and calf circumference at week 8 showed multicollinearity (Fig. 1), where weight was the variable with the greatest correlation coefficient in relation to repetitions of single-leg heel raises (|r|= 0.486, p = 0.011). The predictive model for single-leg heel raise capacity at week 12 was determined by the following equation: (single-leg heel raise capacity) = 1.86 (dorsiflexion range of motion at week 12) – 0.81 (weight) + 32.08, as summarized in Table 4.
Regression results
Standard deviation (sd), Confidence interval of 95% (CI 95%), Coefficient of determination (R2).
The first 12-weeks after AT tenorrhaphy are temporally relevant for inducing changes in the muscle contraction strategies of the plantar-flexor mechanism [15, 20]. In amateur soccer players that received immediate rehabilitation, major displacement of the medial gastrocnemius junction is observable during isometric contraction [17]. In turn, patients that were immobilized and did not bear weight during the first weeks after AT tenorrhaphy evidenced a pathological major use of the deep plantar-flexors during maximal isometric contraction [25]. The literature frames these outcomes as issues of muscle force generation that are reflected by a delayed, reduced ability to perform single-leg heel raises [1–6]. In this study, all null-hypotheses were rejected, with the following specific findings: (1) as compared with traditional rehabilitation after AT tenorrhaphy, the mean for single-leg heel raise repetitions at week 12 is significantly greater for patients treated with immediate rehabilitation, (2) immediate rehabilitation allows patients to achieve a mean of 25 single-leg heel raise repetitions, (3) as compared to the non-injured limb, the repetition mean for single-leg heel raises is recovered using immediate rehabilitation, and (4) two post-tenorrhaphy clinical parameters of the AT were predictors of more single-leg heel raises at week 12 after AT tenorrhaphy.
The early rehabilitation program translated into earlier and more single-leg heel raises than for traditional rehabilitation, as well as more single-leg heel raises than the physiological reference and a non-statistical difference compared to non-injured limb at week 12. These findings suggest that early, controlled weight bearing and mobilization during the first weeks after AT repair result in improved force generation of the plantar-flexors after 12 weeks of physical therapy such as the results in strength of the meta-analysis of McComark et al. [26] suggested improved more early in patients who experience functional rehabilitation. Also, this conclusion aligns with Wang’s hypothesis [15], which states that “the neuromechanical changes caused by postoperative immobilization, restrictions or limitation to foot/ankle are gave within the first 3 months after AT repair.” This hypothesis was proposed after finding pathological neuromuscular outcomes within a year after AT tenorrhaphy. The presently obtained results were also in accordance with Jielile et al. [27], who reported that patients could improve their single-leg heel raise performance being treated with a novel surgical technique coupled with early kinesiotherapy [27]. The current findings further support those of Olsson et al. [28], who found that 51% (41/81) of patients that underwent early intervention after surgery were able to perform the single heel-raise task at week 12 post-tenorrhaphy; these patients were significantly younger, more often male, and reported fewer symptoms than the remainder of the patient group. As postulated by Olsson et al. [28], early single-leg heel raise capacity appears to be an important achievement and reflects the general level of healing, thus influencing patient-reported outcomes of physical activity. Pending tasks for future research are to clarify if patients with an early recovery of single heel-raise capacity perform different daily motor tasks better and to determine the consequent economic and functional impacts, as well as effects on a return to sports.
The secondary finding of the present study contrasts with that reported by Bostick et al. [1], who determined that gender, single-leg heel raise repetitions at month six, physical function, and tendon pain while resting at month three were factors associated with a greater ability to perform the single-leg heel raise test one year after tenorrhaphy [1]. The present results also differ from the findings of Olsson et al. [28], who found that age was the principal factor associated with greater single-leg heel raise capacity after six months and one year of evolution [28]. The current study found that the first predictor for achieving more single-leg heel raises at week 12 was a greater dorsiflexion range of movement. This finding is in accordance with Saxena et al. [19], a study in which a greater range of movement was found to be a predictive parameter for a return to normal activities in patients with a tendinous pathology [19]. However, an altered force-length relationship following rehabilitation could arise from early, excessive dorsiflexion range of movement, which can cause AT lengthening [10, 23]. This alteration could lower the ability to generate force during propulsion tasks, such as while walking or during single-leg heel raises [6, 10]. These prior findings suggest that the presently proposed prediction model should consider the dorsiflexion range of movement with caution, particularly since the achieved greater dorsiflexion range of movement was controlled based on previous cadaveric results, an approach taken specifically to prevent early AT lengthening [22, 23].
The second predictor found in this study was body weight. From a neuromechanical perspective, repeated lifting of the center-of-mass against gravity would constitute an external workload for the plantar-flexor mechanism. This subsequently suggests that weight is an important variable to consider when calculating the mechanical load dose to be therapeutically administered in patients during rehabilitation. Regarding load control against gravity, different intra- and intermuscular strategies can therefore be used by the plantar-flexor mechanism, as according to the traits of each exercise (i.e., plantar-flexion range of movement, work cadence, posture for the center-of-mass as related to the axis of knee rotation, etc.). For example, anterior inclination of the trunk in combination with support for the superior extremities (used in rehabilitation as a sign of exercise progression) unloads the plantar-flexor mechanism since the center-of-mass is also supported by the upper extremity. This consequently diminishes the active plantar-flexor torque arising from the ankle during single-leg heel raise execution. Therefore, the posture adapted to perform the single-leg heel raise could result in more repetitions during the rehabilitation process, just as would be facilitated by weight loss during rehabilitation, which is in agreement with the obtained predictive equation. Future investigations need to develop better designs and progressions of therapeutic exercises for rehabilitation following tenorrhaphy of the AT.
One limitation of the present study is that the employed research model unfortunately not considered neurophysiological variables as muscular velocity conduction and electromyography activation patterns. These variables would be relevant for exploring the statistical importance of neuromuscular adaptions of the plantar-flexor to increase single-leg heel raise capacity. Future research should also address this point.
In conclusion, immediate rehabilitation of AT tenorrhaphy results in a quicker recovery of physiological reference values for single-leg heel raise capacity, as well as capacity values similar to the non-injured limb after a 12-week physical therapy program. Furthermore, dorsiflexion range of motion at week 12 and body weight were predictive factors for more single-leg heel raises at week 12 of rehabilitation following mid-substance percutaneous tenorrhaphy of the AT.
Conflict of interest
The authors declare no conflicts of interest.