
Abstract
BACKGROUND:
Fear of falling (FOF) is often reported post-hospitalization and has been associated with functional decline. Identifying the determinants of FOF during hospitalization and patients’ perception of FOF can help guide their managements. To inform a planned future intervention study, this study aimed to evaluate (1) the effects of acute hospitalization on FOF among older adults, (2) older adults’ perception of risk factors, interventions and coping strategies for FOF.
METHODS:
Thirty-two older inpatients were recruited in an acute teaching hospital. This was a mixed methods study. FOF was measured quantitatively using the Single-item question “Are you afraid of falling?” and Fall-Efficacy Scale-International (FES-I), self-reported for premorbid status (retrospectively), on admission and again at discharge. Patients with FOF completed a questionnaire exploring their perception of FOF, possible coping strategies and interventions they believed may help.
RESULTS:
No significant changes in FES-I scores were detected over time, suggesting acute hospitalization did not change FOF in this cohort. A change in FOF (FES-I) score was associated with the history of falls in previous year. Perceived risk factors included balance problems (n = 10), breathlessness (n = 5), reduced lower limb muscle strength (n = 5) and history of falls (n = 4). To cope with FOF, most would avoid activity, seek help and slow their pace. Exercises and education were perceived as effective interventions to reduce FOF.
CONCLUSIONS:
Fear of falling did not appear to develop or change during hospitalization. Patients had faith in education and exercise prescription as effective treatments for FOF post-hospitalization.
Introduction
Hospitalization can result in functional decline in older adults, subsequently leading to a higher risk of disability, institutionalization and mortality [1–3]. Fear of falling (FOF) affects mobility and ADL function post-hospitalization [4, 5], and is associated with future falls and institutionalization [6]. Management of FOF in hospital may help prevent negative consequences post-hospitalization. Previously, studies only measured FOF at one time point (during hospitalization), or studies compared admission-FOF to FOF once discharged home [5–7]. To date, no study has measured FOF related to hospitalization over time; i.e. premorbidly, during hospitalization and at discharge.
Before planning FOF management in hospital, understanding older adults’ perception of FOF is important; their beliefs, attitudes and the group norm may affect adherence to interventions [8]. In-patients’ perceptions are poorly understood, with most research exploring patient perceptions about FOF being conducted in older community-dwellers [9–11]. Information on fear of falling during hospitalization may help design a patient-relevant intervention for FOF, thereby increasing adherence.
Before designing an intervention for FOF, a small study was conducted to (1) explore suitable methods to measure the effect of acute hospitalization on FOF in older adults and (2) to explore their perception of contributing factors towards FOF, thus identifying possible effective interventions in hospital and after discharge.
Methods
Study design and study setting
This study was conducted in a 350-bedded acute teaching hospital in Ireland. A convenience sample was recruited during April and May 2018. The local ethical approval was obtained [ECM 4 (e) 07/03/18]. FOF was quantitatively measured as self-reported retrospectively for premorbid status, currently on admission and again at discharge. A questionnaire was used to evaluate participants’ FOF.
Selection of participants
Medical patients aged 65 years and older, admitted within the preceding 24 hours, with an anticipated hospital stay of ≥3 nights, admitted from and with planned discharge to home, were screened. Patients with significant cognitive impairment, or who were bedbound/chairbound premorbidly, or at end of life, or had an acute psychiatric illness, or were critically ill, were excluded. If the cognitive capacity of the patient was questionable, the researcher used the Six Item Cognitive Impairment Test to screen cognition, using the highly validated cut-off point of 10 to indicate cognitive impairment [12].
Study procedure and measurement instruments
Participants were identified using a daily medical admissions list, an Emergency Department list and from ward lists. Medical records were screened to ascertain eligibility, and confirmed by nursing staff before patients were approached. At the bedside, details of study were fully explained and written consent was gained for participation. A standardized data extraction form was used to record demographic data (age, gender, presenting complaint/ diagnosis, past medical, social and falls history, and discharge plans), which was obtained from participants directly, and from medical notes (Fig. 1).
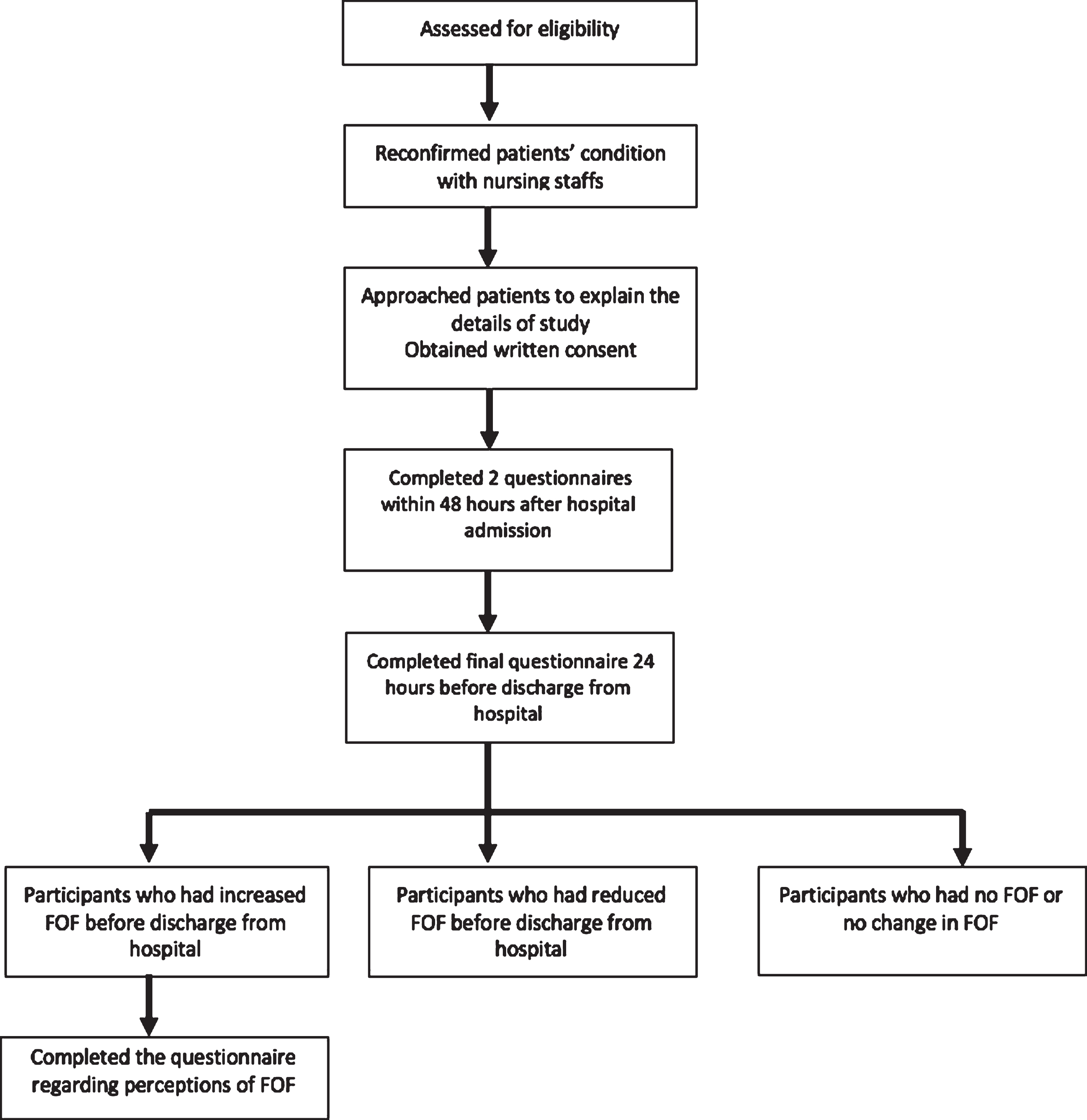
Flowchart of study procedure.
In order to determine if FOF could be screened for quickly, a Single-item question (SIQ) was compared to the validated Falls Efficacy Scale-International (FES-I). Using a Likert scale (“a lot, a little, perhaps, not at all”), the SIQ has been used widely to assess prevalence and degree of FOF among older adults [7, 13–16]. It is highly correlated with FES-I in elderly care in-patient settings [17], with good test-retest reliability [14, 18]. The FES-I is a validated tool developed by the Prevention of Falls Network Europe (ProFaNE) to measure the level of concern about falling when performing 16 different activities [19]. Participants rate their level of concern using an ordinal scale (1–4 from not at all to very concerned) [19]. Total score ranges from 16 to 64, with a cut-off score of ≤19 indicating low concern about falling, between 20–27 indicating moderate concern and ≥28 indicating high concern [20]. This questionnaire has shown excellent reliability, minimal floor effect, no ceiling effect, and sensitivity to change in older adult populations [17, 20].
The first and second SIQ and FES-I scores were completed within 48 hours of hospital admission, with the researcher’s assistance as required. The first score was based on their self-reported premorbid functional status and FOF (“About 2 weeks before hospital admission, when you were well... ”), and included falls history over the previous year. The second score was based on their current status (on admission). Each questionnaire took less than 10 minutes to complete.
Upon completion, nursing and therapy staffs were approached to determine the participants’ functional status and planned discharge date. Healthcare records were examined daily to monitor progress. Participants were approached for a final time within 24 hours of planned discharge date to complete the final SIQ and FES-I. Patients with increased FOF (either a greater pre-discharge SIQ report or FES-I score, than premorbid or admission scores), were asked to complete a questionnaire exploring their perception of FOF.
The research team developed a simple questionnaire to evaluate participants’ perceptions about FOF with minimal burden on patients [21]. The questionnaire’s themes were based on published literature [10, 22–26], aiming to explore contributing factors to FOF, coping strategies after discharge home, suggested intervention to reduce FOF and determinants of FOF during hospitalization (if applicable).
Data was analysed by using IBM SPSS Statistics 24. A p-value of <0.05 was denoted as statistically significant in all tests. Analyses was done based on complete data. Baseline characteristics are presented using descriptive statistics. Categorical data is presented using count and percentage, normally distributed data using means (standard deviation (SD)) and non-normally distributed data using medians (interquartile range (IQR)). Qualitative data, including contributing factors, possible interventions and coping strategies, are presented as frequencies.
With the small sample size, the Fisher’s Exact Test was used to measure the association between changes in FES-I score and participants’ baseline characteristics.
Results
Of the 258 patients screened, 46 were eligible for this study. Reasons for exclusion (n = 212) are presented in (Fig. 2). Three eligible patients declined to participate and one patient’s cognition prevented data collection. Ten patients’ follow-up assessments were missed due to unexpected early discharges. The remaining 32 participants’ data was complete, and used in the analysis. There were no significant differences in the age, mobility or premorbid-FOF between the final included participants and those who declined or had missing data.
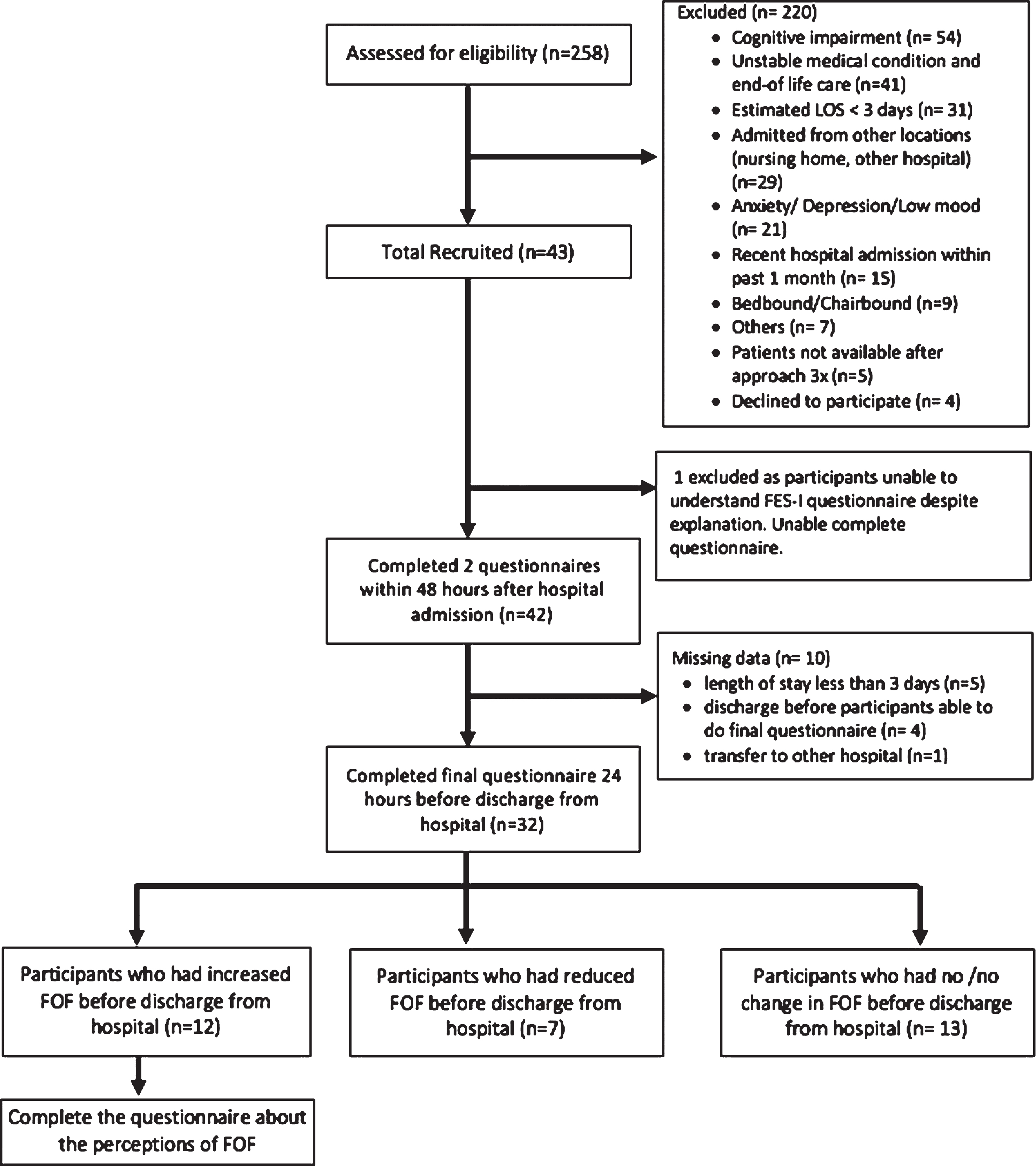
Participant flow.
Baseline characteristics are presented in (Table 1). Most participants were male (n = 22, 68.8%), aged between 65–86 years (75±5) with a length of stay (LOS) between 3 and 14 days (median 6 [4–10]). The main reasons for admission were cardiopulmonary conditions, which included acute decompensated heart failure and exertional chest pain. All were independently ambulant premorbidly, with most being community ambulant (n = 25, 78.1%). Fifteen participants (34.4%) had fallen at least once in the previous year; three (9.4%) of whom had fallen in the week prior to admission.
Baseline characteristics of participants
Baseline characteristics of participants
Abbreviation: FOF = fear of falling based on single item question “Are you afraid of falling?
In answering the SIQ (Are you afraid of falling?), most reported no premorbid-FOF (n = 25, 78.1%), or admission-FOF (n = 24, 75%) or discharge-FOF (n = 26, 81.3%). However, the FES-I results indicated somewhat different findings. While none had high levels of concern about falling, 15 (46.9%) had moderate levels of concern about falling premorbidly, 16 (50%) on admission and 15 (43.8%) at discharge. This suggested that patients were somewhat concerned about falling, however, hospitalization had little effect on FOF in this cohort.
Only four participants (12.5%) experienced more FOF at early onset of the acute illness; i.e. their admission-FES-I score was greater than their premorbid-FES-I. The remaining twenty-eight (87.5%) had similar FES-I scores premorbidly (21 [18–24]), and on admission (21 [18–25]), p = 0.125.
While ten participants reported increased FOF during their illness (from premorbid report to discharge report), another ten reported decreased FOF (discharge-FES-I, 20 [17–24] vs premorbid-FES-I, 21 [18–24]), p = 1.0. Nine participants (28%) reported increased FOF during hospitalization (admission to discharge), while 12 (37.5%) reported less FOF (admission-FES-I, 21.00 [18–25] vs discharge-FES-I, 20.00 [17–24]) p = 0.7.
Associations between change of FES-I score and baseline categorical variables
The cohort was divided into three groups: those who reported a greater, less or no change in FOF during hospitalization, comparing admission and discharge SIQ and FES-I scores. A fall in the previous year was the only variable statistically significantly associated with a change in FOF. Of the nine participants with greater FOF during hospitalization, seven had fallen in the previous year (p = 0.018).
Associations between change of FES-I score and categorical variables
Associations between change of FES-I score and categorical variables
The twelve participants who reported greater FOF (by FES-I or SIQ) during hospitalization completed a questionnaire exploring their experience of FOF. Common contributing factors included balance problems (n = 10, 90.9%), breathlessness, all with history of COPD, (n = 5, 45.5%); lower limb muscle weakness (n = 5, 45.5%), and history of fall (n = 4, 33.3%).
Seven participants used activity-avoidance as a coping strategy, nine slowed movement down, and eight sought help to move around. Only two patients reported receiving FOF education, one of whom received falls prevention education also. Participants believed that home exercises prescription (all), education about coping strategies for FOF (n = 11) and fall risk preventions (n = 12) could help to manage their FOF.
Discussion
The results of this study showed that (1) acute hospitalization did not in general increase FOF in older adults; (2) patients who did have a heightened FOF pre-discharge had previous falls; and (3) older adults’ perception of risk factors, interventions and coping strategies are consistent with existing literature.
Acute hospitalization does not increase FOF in older adults
No significant change in FES-I score was detected over time, suggesting that hospitalization had no effect on FOF. Previous studies have shown that older adults had FOF on admission and post-hospitalization [5–7]. However, the studies only measured FOF at a single time point (after hospital admission), or compared FOF on admission to FOF at home after discharge [5–7]. This is the first study measuring FOF during hospitalization.
However, the patient cohort may explain the null findings. Most were male, independently-ambulant both premorbidly and in hospital. Denkinger et al. identified the female gender, functional decline and walking-aid use as risk factors for FOF in older community-dwellers [22]. Hence, it is reasonable that our cohort did not develop FOF in hospital. Future studies should focus on a frailer in-patient population.
Association between history of falls in past year and the change of the level of FOF
Falls in previous year and worsening FES-I score were significantly associated, suggesting that fallers are more likely to develop further FOF during hospitalization. A fall history is strongly linked to FOF, development of FOF post-hospitalization and is a predictor for persistent FOF [5, 27–29]. Potentially, the symptoms of acute illness can lead to insecurity and confidence walking in the hospital. As walking in hospital is associated with a shorter hospital stay [30], this group need assessment and targeted interventions to address the negative effects of their inactivity in hospital and should be included in future studies.
Perceptions about fear of falling
No study has been found exploring patients’ perceptions of contributing factors and interventions for FOF. The participants’ self-perceived risk factors for FOF were balance problems, breathlessness, reduced lower limb muscle strength and history of falls. Most of these factors have been previously detected [22, 32], however breathlessness has not previously been found. In this study, all participants with COPD (n = 5) stated breathlessness was a contributor, potentially reducing their exercise capacity, leading to their FOF [33, 34]. Functional capacity has been previously associated with FOF in older adults with stable COPD [35], or the discomfort associated with low oxygen intake may also cause the FOF. This novel finding warrants further investigation.
Patients perceived potentially effective interventions to be exercise prescription, education on FOF management and fall risk reduction, suggesting they intuitively believe in the evidence-based interventions, increasing their interest and adherence [8, 25]. Education regarding FOF managements and fall risk reduction are part of the components of cognitive-behavioral therapy, which is known as effective intervention for FOF [36, 37].
Patients’ planned coping strategies post-hospitalization are also consistent with previous evidence [10, 23]. Activity-avoidance and slowing down during movement are commonly-used strategies [23], and may be a practical solution for those who live alone. However, it may lead to further functional decline and reduction in quality of life [23]. Interventions to promote exercise and activity in hospital [38], and at home [26] may reduce the negative consequences of inactivity after discharge.
Limitations of the study
The results from this study need to be interpreted carefully. Firstly, this is a small study and needs to be repeated with a larger sample size. As this study used a convenience sample, most participants were robust, fairly independent and cognitively intact, limiting the findings’ generalizability. Future studies should focus on frailer in-patients, those with a falls history, or with a higher risk of developing FOF, especially those with cognitive impairment [39, 40].
Using self-reported premorbid FOF was a practical solution given that patients were first recruited after admission to hospital. However, it may have led to some bias. Premorbid status was defined as status two weeks prior to admission, however, some participants reported an illness period of greater than two weeks. Defining their own premorbid status timeline (before the acute illness onset) may lead to better accuracy. The Falls Efficacy Scale detected more fear of falling than the SIQ.
Conclusions and implications to future research
In-patients without functional impairments/decline did not develop FOF during hospitalization. Non-independently ambulant, or frailer patients with a falls history or FOF should be examined specifically. Patients with poor cognition, as a high risk group, should be included if they are able to follow commands. The FES-I appeared more sensitive to FOF than the SIQ in older medical inpatients. Patients with COPD should be explored specifically in future studies. The in-hospital management of potentially maladaptive patient-identified coping strategies, namely exercise avoidance/slowing down (which can lead to negative consequences post hospitalization), should be examined. Older adults are aware of their FOF and their personal risk factors for FOF and they believe in evidence-based interventions. Hence, evidence-based interventions in hospital should be examined further.
Conflict of interest
None to report.