
Abstract
BACKGROUND:
The prevalence of Achilles tendinopathy is greatest in activities including middle and long distance running, tennis, badminton, volleyball, and its incidence is increasing. However, currently no gold standard treatment for Achilles tendinopathy exists, although eccentric exercises are commonly recommended.
PURPOSE:
This study aimed to investigate the changes in clinical scores when administering a) acupuncture and b) sham acupuncture to the Achilles tendon in patients diagnosed with Achilles tendinopathy who did not respond to modified eccentric exercises.
METHODS:
Twenty-two patients were randomised and received either acupuncture or the control sham acupuncture treatment. VISA-A, NPRS, EQ-5D and GRC were recorded before treatment at week 0, then at week 2, week 4 with a final follow-up review at week 12.
MAIN RESULTS:
Acupuncture resulted in significant differences between groups and time points in VISA-A, NPRS, EQ-5D and GRC. The Acupuncture group reached the minimum clinically important difference (MCID) threshold for important difference, when compared to sham acupuncture. The difference between treatments would suggest a beneficial response following the use of acupuncture to the Achilles tendon in Achilles tendinopathy.
PRINCIPAL CONCLUSIONS:
The overall findings suggest the use of a standardised acupuncture protocol to the Achilles tendon is a viable treatment alternative, which could be used as a second line treatment in patients diagnosed with Achilles tendinopathy who did not respond to eccentric exercises. However, in view of the small sample size, the results of this feasibility study should be viewed with caution.
Introduction
The incidence of Achilles tendon injuries is increasing as more individuals regularly exercise both recreationally, and within sports [1, 2]. The prevalence of Achilles tendinopathy is greatest in activities involving endurance running [3–6]. Injuries are also seen in sedentary individuals, with 65% of patients diagnosed with Achilles tendinopathy having no link to sport or physical activity [7].
The mid-portion of the Achilles tendon is the most commonly injured site accounting for 55–65% of all Achilles tendon injuries [3]. Due to the quality and methodological shortcomings in studies [8], there is still no gold standard treatment for Achilles tendinopathy [9]. At present the greatest amount of evidence supports eccentric exercise as a first line treatment option [10–12], however, this is not always successful. Acupuncture is one of the best known complementary therapy treatments, and is widely used for musculoskeletal disorders and has been shown to offer pain relief [13]. Pain relief may be related to spinal acupuncture mechanisms through the effects of counter stimulation, or supraspinal acupuncture mechanisms through diffuse noxious inhibitory control (DNIC), and the stimulation of the descending antinocicepetive pathway and the limbic regions of the brain [14].
To date only one study by Zhang et al. [15] has explored the use of acupuncture in the treatment of Achilles tendinopathy. They reported an increase of 25.8 after 16 weeks and 28.4 after 24 weeks from baseline was found in the Victorian Institute of Sports Assessment — Achilles (VISA-A) for the acupuncture group, with a corresponding decrease of 3.2 at rest in the Visual Analogue Scale (VAS). These results suggested significant functional improvements and decreases in pain, which were greater following the use of acupuncture compared to eccentric exercise. However, when considering clinical outcome measures associated with Achilles tendinopathy treatments, the Numerical Pain Rating Scale (NPRS) [16], Global Rate of Change (GRC) and Euroqol-5D (EQ-5D) may also assist in identifying change in pain and health status. However, these outcome measures have yet to be validated for use on the Achilles tendon.
The aim of this randomised feasibility study was to investigate the changes in clinical scores when administering a) acupuncture and b) sham acupuncture to participants diagnosed with Achilles tendinopathy who were non-responders to a standardised eccentric loading programme.
Method
One hundred and fifty-two patients with Achilles tendon pain were referred to physiotherapy mainly through the GP service. Sixty-three patients were excluded due to; presence of insertional Achilles tendinopathy (24), naturally resolving symptoms (7), did not attend (7), medical co-morbidities (5), lumbar origin (5), other tendinopathies (3), declined intervention (3), ruptures (2), ankle OA (2), plantar fasciitis (2), unable to attend (1), referred for further investigation (1) and previous Achilles rupture (1). Of the eighty-nine eligible patients who consented, eighty-four patients (45 male, 39 female) were recruited, 80 patients (41 male, 39 female) completed the modified eccentric exercise phase (conservative treatment including the modified eccentric loading protocol).
The modified eccentric exercise protocol used in this study was adapted from Alfredson et al. [17]. Participants performed two types of eccentric exercises, with knees straight and with knees flexed, with a pain threshold of no greater than 4/10 on a VAS. Both exercises were performed bilaterally or unilaterally, depending on the level of discomfort not exceeding the pain threshold, using minimal concentric movement. Each exercise included up to 15 repetitions performed in 3 sets once per day.
Ethical approval was gained from NRES Committee North West — Greater Manchester South - REC 12/NW/0035, the University of Central Lancashire — BuSH 067 with Research and Development approval obtained from Southport and Ormskirk NHS Trust — 2011/059/LTC. All procedures followed during the study were in accordance with the Helsinki Declaration.
All patients were provided with modified eccentric exercises (within a pain framework — pain no greater than VAS 4/10) that allowed minimal pain free concentric movement. Standard static stretching was also provided coupled with appropriate footwear advice, orthotics, and management advice. During this 6-week phase patients were seen four times, two weeks apart over a 6-week period. The non-responders to modified eccentric exercises and standard treatment were invited to be randomised into two treatment groups, a) acupuncture or b) sham acupuncture. The randomisation was performed using a computer generated random number list. Once consent had been provided for the acupuncture phase, digital weighing scales were used to measure body weight, and stature was measured using a standard tape measure against a wall, whilst bioelectric impedance analysis was used to measure percentage body fat. The non-responders then attended three acupuncture/sham acupuncture treatments which were performed at weekly intervals, week 0, week 1 and week 2. Figure 1 shows the Achilles tendinopathy patient treatment and assessment flowchart.
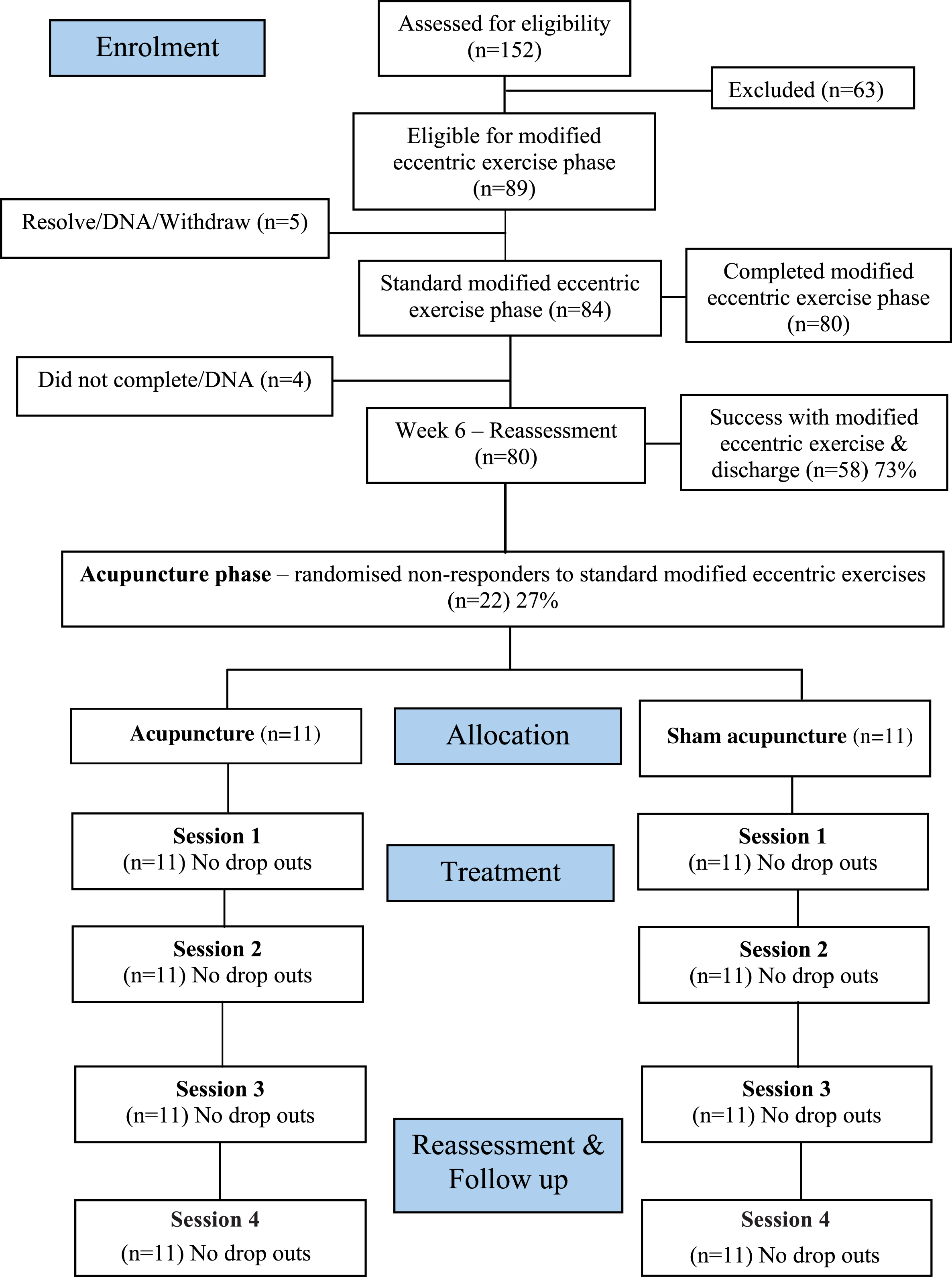
Achilles tendinopathy patient treatment and assessment flowchart.
The Acupuncture treatment was provided by a member of the Acupuncture Association of Chartered Physiotherapists (AACP) and followed AACP guidelines. The Acupuncture technique used was standardised 9-needle Achilles tendon acupuncture protocol [18], (Fig. 2). The Achilles tendon was cleaned using alcohol wipe sterets, with participants positioned in prone lying. Nine small plastic rings covered with sterile tape were then attached to the Achilles tendon to enable the Streitberger sham acupuncture needles to remain in place [19]. Acupuncture or sham acupuncture needles were then inserted into the Achilles tendon, with the needles stimulated for 60 seconds every 5 minutes in a thrusting/twisting motion. The acupuncture session ended 30 minutes after the last acupuncture or sham acupuncture needle was inserted, then needles were removed.

The standardised 9-needle Achilles tendon acupuncture protocol inserted into the Achilles tendon (Kishmishian et al., 2012).
All patients were assessed using the VISA-A, NPRS, GRC and EQ-5D forms. The GRC has been used as an 11 point Likert scale in numerous studies [20, 21] with [22] recommending the use of an 11-point scale for GRC over other scales. The EQ-5D is a standardised measure of health status, and is a quality of life questionnaire which comprises of 5 questions relating to health, mobility, ability to self-care, ability to undertake usual activities, and anxiety and depression, which have been shown to be valid and reliable [23–25]. Although, no data has linked these measures with Achilles tendinopathy. When used as a secondary outcome measure, these provided a more holistic assessment of Achilles tendinopathy. From the 5 health dimensions measured, scores are then inserted into the EQ5D index value calculator which provide an index of health. Clinical scores were measured before acupuncture and sham acupuncture treatment and assessment at week 0 (session 1), before treatment on week 2 (session 2), before review and reassessment at week 4 (session 3) and before the final follow-up review at week 12 (session 4).
Differences between the two groups and time points in the VISA-A, NPRS, GRC. VISA-A and NPRS scores were tested for normality of distribution using the Kolmogorov-Smirnov test and were found to be normally distributed and suitable for parametric statistical testing, whereas the EQ-5D scores were found to be non-normatively distributed. A Repeated Measures ANOVAs was used for the VISA-A and NPRS scores and a Mann-Whitney U test was used for the EQ-5D scores. In addition to the Repeated Measures ANOVAs the effect sizes were also calculated, and p values < 0.05 were regarded as significant. The differences between groups and time points were further explored using mixed methods ANOVAs. All data analysis was performed using SPSS version 21 (Chicago, IL, USA).
To determine clinical importance two factors were considered; the minimum clinically important change (MCIC) from baseline of pre-treatment to a certain time point in a primary endpoint of a treatment, and the minimum clinically important difference (MCID) between treatment groups [26]. The clinically important thresholds for the outcome measures were based on previous research with 16 points for the VISA-A [27], 2 points for the average pain for the NPRS [28] and an index value of 0.074 for the EQ-5D [29]. The GRC was dichotomised [30, 31] into responders and non-responders, the rate of success was expressed as patients who achieved +3, +4 and +5 points, from an 11 point GRC scale (ranging from –5 much worse to +5 much better).
Results
Twenty-two patients who were non-responders consented to enter the study. These consistent of 8 male and 14 female patients aged between 35 and 72 with a mean age of 51.8 years, height 1.70 meters (0.1), weight 89.3 kg (14.1), percentage body fat 34.5% (7.0%) and had a BMI of 30.2 (3.1).
Differences between the two groups confirmed a significant difference (p < 0.001) between acupuncture and sham acupuncture groups. The total change in acupuncture and sham acupuncture EQ-5D from baseline to the final follow-up session in week 12 was 0.16 and 0.01 respectively. Overall acupuncture showed a greater increase in EQ-5D score in comparison to sham acupuncture by 0.15. The Repeated Measures ANOVA show a significant mean increase in VISA-A score following both acupuncture and sham acupuncture. Additionally, a significant decrease in NPRS score was seen in the acupuncture group, whilst no significant difference was seen in the sham acupuncture group, (Table 1).
Mean change from baseline and standard deviation (sd) for VISA-A and NPRS and Repeated Measures ANOVA main effects with effect size
Mean change from baseline and standard deviation (sd) for VISA-A and NPRS and Repeated Measures ANOVA main effects with effect size
Further pairwise comparisons were conducted for the significant main effects, (Table 2). The acupuncture group showed a significant difference between all weeks/sessions (p < 0.001 to p < 0.002), with the exception of week 4 to week 12, where treatment effects stabilised. For sham acupuncture, a significant increase between the baseline in week 0 to week 4 (p = 0.002), and to the final follow-up session in week 12 (p = 0.016). For the NPRS scores the acupuncture group showed significant differences between the baseline at week 0 and week 2 (p < 0.001), and between weeks 4 and 12 (p < 0.003), (Table 2). The largest change occurred between baseline in week 0 and week 4, with a decrease of 2.91 points, although this then increased slightly by 0.36 points at the final follow up session in week 12.
Repeated Measures ANOVA Pairwise comparisons for significant main effects for NPRS and VISA-A for Acupuncture and Sham groups
The mixed methods ANOVA showed no significant difference in NPRS and VISA-A scores over the time points for grouped data (p = 0.152, p = 0.163). However, significant differences were seen between treatment groups (p < 0.001), with the acupuncture group demonstrating a significant difference of 12.42 points (p = 0.001) in the VISA-A and 1.55 points (p = 0.001) in the NPRS when compared to sham acupuncture, Table 3.
Mixed methods ANOVA Pairwise comparisons between the Sham and Acupuncture treatment groups
The GRC was dichotomised [30, 31] into responders and non-responders. The acupuncture group demonstrated 73% of patients were responders, whereas the sham acupuncture group demonstrated 36% responders. Dichotomisation showed that there were 73% of responders in the VISA-A score in the acupuncture group, more than double that of the 27% of responders in the sham acupuncture group, when the cut point for clinical significance is a change of 16 points. The percentage of responders for VISA-A score is equal to the number of responders for the GRC. For NPRS, 64% of responders in the NPRS score in the acupuncture group, more than triple that of the 18% of responders in the sham acupuncture group, when the cut point for clinical significance is based on a change of 2 points.
Acupuncture resulted in a statistically and clinically significant increase in VISA-A scores from baseline to session 4 by 27 points. When compared from baseline, the use of acupuncture to the Achilles tendon in Achilles tendinopathy exceeded the 16 point threshold for VISA-A MCIC and MCID at 12 weeks. The greatest increase in VISA-A was noted in session 3 and 4, at week 4 and week 12 respectively, following the acupuncture treatment. This suggests that improvement seen following the final acupuncture treatment in week 2 was maintained for the follow-up periods.
Only one previous study by Zhang et al. [15] has explored the use of acupuncture measured pain and function using the VISA-A. This reported a significant increase in at 8 weeks by 22.1 points, at 16 weeks by 25.8 points and at 24 weeks by 28.4 points which supports the findings of this study. However, Zhang et al. [15] used 4 acupuncture needles into a painful area in the Achilles tendon, which could not be kept consistent between treatments or participants; as the painful area can increase or decrease in size between treatment and participants.
The increase in VISA-A score following acupuncture is similar to that reported by Tumilty et al. [27] and Rompe et al. [32]. They reported significant increases from baseline to 18.5 points at the week 4, increasing to 32.4 points at 12 weeks and an increased VISA-A scores in Achilles tendinopathy following eccentric loading and Extra Corporeal Shock Wave Therapy (ESWT) respectively. Eccentric loading increased by 25 points at the 4 month follow-up compared to the ESWT group increase by 20.1 points. Rompe et al. [33] also reported increased VISA-A scores in Achilles tendinopathy following both eccentric loading only and eccentric loading coupled with ESWT. The eccentric loading group increased by 22.7 points at 4 months; whereas the combined eccentric with the ESWT group increased by 36.3 points.
Acupuncture resulted in a 2.5 point NPRS decrease in pain compared to a 0.27 point decrease following sham acupuncture. Therefore, the standardised acupuncture protocol to the Achilles tendon in the Achilles tendinopathy RCT met the MCIC and MCID 2 point threshold for the decrease in pain using the NPRS outcome measure. The greatest decrease in pain occurred at week 4. Similar to the results of the VISA-A, if a greater number of treatments had been administered, this may have resulted in greater reductions in pain. Similarly, Rompe et al. [33] reported a significant decrease in NPRS in Achilles tendinopathy following both eccentric loading only and eccentric loading coupled with ESWT. The eccentric loading group decreased by 3.1 points at 4 months, whereas the combined eccentric with ESWT group decreased by 4.4 points. Conversely, Tumilty et al. [27] reported a non-significant decrease in NPRS at 4 weeks when using low-level laser therapy (LLLT) to the Achilles tendon, which suggests acupuncture to the Achilles tendon may be more useful than LLLT in Achilles tendinopathy.
The overall difference in average Achilles tendon pain over a one week period using NPRS between acupuncture and sham acupuncture, resulted in a significant difference of –1.55 points (–2 points). No significant difference were seen in the NPRS following sham acupuncture, despite an initial decrease from baseline to session 2 by 1 point. Interestingly by session 4 at week 12, pain returned to baseline values, suggesting sham acupuncture is ineffective in reducing pain. The initial reduction in pain is likely to be related to mixed mechanisms of a placebo response, and the limbic touch response [34, 35], and suggests any reduction in pain occurring from sham acupuncture may be short lived.
In addition, the standardised acupuncture protocol to the Achilles tendon in the Achilles tendinopathy randomised feasibility study exceeded the MCIC and MCID 0.074 point threshold for the improvement in health [29]. This was supported by the positive and statistically significant VISA-A and NPRS data that show all values change in the same direction, suggesting improvement and an effective treatment. Furthermore, GRC data demonstrated that 73% of patients in the acupuncture group responded to treatment. Therefore, if a patient has less pain, this could result in an increase in function and activities of daily living.
Potential mechanisms
The potential physiological mechanisms behind the effects found in this study could be related to the local and segmental effects of acupuncture reported by Tian et al. [36]. The clinical improvements noted in the acupuncture group, may be related to the local increase in blood flow and oxygenation, through pro-inflammatory effects and the mechanism of axon reflexes and the inhibition of the sympathetic nervous system [37, 38]. The stimulation of A-Delta and C-afferent fibres would release vasoactive and pro-inflammatory neuropeptides such as calcitonin gene-related peptide (CGRP), substance P, neurokinin and opioids. This would result in peripheral vasodilation in to the Achilles tendon, which is mainly mediated by CGRP [39]. The release of growth factors such as vascular endothelial growth factor following acupuncture could promote an increased vascular response following acupuncture and assist in Achilles tendon healing, by the local increase in fibroblasts and tenocytes which result in cellular proliferation and collagen synthesis [40]. The functional improvement seen in the VISA-A could suggest tissue healing may have occurred, which could enable the structure and function of the Achilles tendon to return to its pre-injury status [41].
The local reduction in pain may also be related to the spinal acupuncture mechanisms through the effects of counter stimulation [14]. The supraspinal acupuncture mechanisms of pain relief through the DNIC, could account for a short-term pain relief following treatment in the few patients that experienced this. The reduction in pain may be related to the stimulation of the descending antinocicepetive pathway and the limbic regions of the brain. This would result in the release of betaendorphins, adrenocorticotropic hormone and cortisone. Studies using fMRI [36, 42] have reported that a strong DeQi stimulation resulted in significant deactiviations in the brain, indicating a mechanism for pain relief.
The standardised Achilles tendon acupuncture protocol [18] on patients with Achilles tendinopathy, is suggested to primarily stimulate the Achilles tendon locally, causing local pro-inflammatory healing and pain relieving effects. The use of acupuncture could also activate all three mechanisms of acupuncture analgesia, locally, segmentally/spinally and supraspinally [39].
Strengths and limitations
No dropouts were recorded in the 22 patients randomised into the acupuncture or sham acupuncture treatment groups which increases the confidence in the results by reducing the bias that can be introduced through dropouts. The non-specific effects of acupuncture and sham acupuncture [43] were controlled as the same protocol, practitioner, patient-therapist interaction resulted in equal empathy and communication to all patients between groups. However, this was a single blinded randomised feasibility study where only the participant was blinded, and where the principle investigator in this study was also the acupuncturist and physiotherapist, which could introduce bias.
Although both needling techniques were uncomfortable, the intensity during a 60 second stimulation of an acupuncture is stronger than the stimulation of a sham needle. However, as no patient had experienced penetrative acupuncture to the Achilles tendon, this was not felt to affect blinding. Improvements in pain may be, in part related to the 4 day relative rest phase between treatment and by following a pain framework of not exceeding VAS 4/10 for general activities. However, as the majority of patients had rested and offloaded unsuccessfully prior to attending the study and followed the pain framework in the modified eccentric exercise phase of the study design, therefore it is unlikely that this could account for the magnitude of the differences between groups.
Due to sample population group not performing hopping actions in daily activity, this was considered to introduce an unnecessary risk. Therefore, in this study the Hop element comprising of 10 points was omitted from the VISA-A questionnaire. Although this would reduce the risk of Achilles tendon rupture, the VISA-A was developed for sporting athletes rather than for sedentary patients who do not take part in regular vigorous exercise. This possibly distorted the baseline and final outcome measure values, which should be considered when making future comparisons. Furthermore, as patients in the acupuncture group returned to their previous levels functional activities, and were able to self-manage their symptoms on discharge, this may suggest that acupuncture is a beneficial treatment alternative and why the relatively low final score of 60 on the VISA-A was achieved following acupuncture treatment.
Recommendation for clinical practice
The positive effect of the 6 week modified eccentric loading phase in this study, coupled with standard physiotherapy management advice (within a pain framework — pain no greater than VAS 4/10) on Achilles tendinopathy, is an imperative first line treatment, which is supported by previous studies [10–12]. The results of this randomised feasibility study suggest a minimum of 3 weekly acupuncture sessions may be required to achieve of positive outcome in non-responders to the recommended first line treatment for Achilles tendinopathy. During acupuncture treatments, the recommended 4 days of relative rest between acupuncture sessions is advocated, before gradually progressing loading, exercise and function, within a pain framework.
Conclusion
This randomised feasibility study has shown statistically and clinically significant improvement in VISA-A, NPRS, EQ-5D and GRC following acupuncture to the Achilles tendon in patients with Achilles tendinopathy. Acupuncture reached the MCIC and MCID threshold for important change for all clinical scores. Whereas sham acupuncture failed to meet any MCIC or MCID threshold for important change in clinical scores. This study shows that acupuncture can have a positive effect in 73% of non-responders to the first line treatment of Achilles tendinopathy. This suggests that the use of a standardised acupuncture protocol to the Achilles tendon is a viable treatment alternative and an effective second line treatment in patients diagnosed with Achilles tendinopathy who are non-responsive to eccentric exercise.
Conflict of interest
None to report.