
Abstract
BACKGROUND:
Pregnancy includes a series of changes to posture and gait.
PURPOSE:
The aim of this study is to investigate the short-term effect of proprioceptive training on the postural balance of pregnant women.
METHODS:
This is a randomized controlled trial with blinding of participants and examiners conducted in physician practices at the obstetric department of the hospital. Thirty-nine pregnant women with age between 25–30 years at 20 weeks gestation (WG) were randomized into blocks and allocated to either the intervention group with proprioceptive exercises (PEG; n = 20) or the control group (CG; n = 19). All outcomes (anteroposterior (AP), mediolateral (ML) and global postural sway (GPS) indices were measured by the Biodex Balance System®-BBS at 20, 24, and 32 WG.
RESULTS:
After 4 weeks’ intervention, the PEG showed decreased sway (AP, ML, and GPS indices) compared to the CG, indicating an improvement in postural balance due to the intervention. With pre- and post-intervention (between 20 and 24 WG), the PEG showed decreased AP and GPS sway. In the CG, without intervention, no sway was different between the pre and post period. After 8 weeks of follow-up (32 WG), the PEG demonstrated the maintenance and improvement of all the index of postural sway. In the CG, these index of postural sway has significantly increased.
CONCLUSION:
The proprioceptive training is effective in the reduction of postural sway during pregnancy. This improvement was maintained after 8 weeks of follow-up.
Introduction
Pregnancy involves a series of changes to the soft tissues and joints, as well as to posture and gait [1–3]. Generally, these modifications are caused by hormonal changes [4, 5] and musculoskeletal system changes [1], which can result in musculoskeletal pain [5, 6] and joint instability in the lower limb [4, 5] of the pregnant woman, affecting postural balance and entailing an increased risk of falling [8–14].
The fall risk has been found to be around 27% in pregnant women who reported a fall during one last their pregnancy [10] promoting changes in the postural sway [12]. Postural balance is best described as the ability to maintain the body’s center of gravity (COG) within the area of support provided by the feet [13].
Pregnant women perform postural adaptations to maintain corporal balance, promote appropriate joint force distributions, and achieve greater stability of the lower limb [14]. Substantial weight gain is about 50% of their body weight; it is concentrated in the abdominal area, and these alterations shift the COP, alter the postural balance and icrease the risk of falls [8, 12]. Butler et al. [8] reported increased postural sway throughout pregnancy, as evidenced by the increased length of the center of pressure (COP) path during quiet stance in pregnant women, when compared with non-pregnant women. McCrory et al. [11] observed that initial sway, total sway, and sway velocity of center of pressure (COP) were significantly less during the third trimester than during the second trimester and when compared to the non-pregnant controls. According to McCrory et al. [12], theses sway of the COP also showed to be decreased in pregnant fallers than in the no-fallers and control participants. Therefore, these changes generate compensatory postural adaptations that can overload somebody segments and cause pain (lumbar spine and lower limbs) [15]. This usually interferes with the quality of life of the pregnant woman [16].
In addition, there are other changes such as memory problems and difficulty in concentrating task and posture [16]. Besides, other important changes occur such as an anterior shift in the location of the center of mass [11, 12], increased ligamentous laxity [4, 5], decreased neuromuscular control and coordination [14, 16], swelling of the arms and legs [1], decreased abdominal muscle strength [7, 14], and increased lumbar lordosis [1, 3]; further changes in mechanical plantar loading [14] contribute to influencing or reducing control of motor tasks, promoting postural imbalances in the pregnant woman [17, 18]. The last trimester contributes to increase of the postural instability, with its increased fall risk [19].
Clinical findings show that 40% of all trauma-related visits to the emergency room or hospital admissions of pregnant women are attributed to accidental falls [20]. These falls may result in fractures, joint sprains, muscle strains, head injury, placental separation, uterine rupture, and occasionally maternal or fetal death [21]. Most of the falls (64%) occur during the second trimester of pregnancy [21]. According to Dunning, Lemasters and Bhattacharya [10] 27% of women fell while pregnant, and 10% experienced two or more falls. There is an urgent need for primary prevention in this high risk group [10].
Additionally, two-thirds of falls are associated with walking on slippery floors, rushing, or carrying an object. The root causes of these falls are not well-known. However, some factors that may contribute to the injuries sustained include deviations from normal posture, postural imbalance [17], and gait with plantar overload [22].
Another important observation is that the risk of falls may remain even after delivery, since, according to Butler et al. [13], postural stability declines gradually during pregnancy and remains diminished for 6 to 8 weeks after delivery. McCrory et al. [12] reported that pregnant women who have fallen exhibit altered dynamic postural stability compared to those who have not fallen, as well as compared to non-pregnant women.
This evidence from the literature suggests that physiotherapists, within their clinic practice, should observe and propose intervention programs that emphasize postural balance and the prevention of falls [23]. However, no study appears to have been conducted hitherto to verify the influence of proprioceptive exercises to increase postural stability in women during pregnancy. Exercise in pregnancy is encouraged, as long as the woman is generally healthy and the pregnancy is free of complications [24]. A wide range of moderate-intensity, non-contact activities are recommended to maintain posture and muscle strength [24], but neither of the two studies cited above mentions exercise specifically directed toward improving postural balance.
Thus, the purpose of the present study is to measure the effect of proprioceptive training, short-term, on dynamic postural balance during pregnancy and after 8 weeks of follow-up. The clinical relevance of this study is that the results obtained may improve physical therapy interventions to deal with musculoskeletal system changes and thereby enhancing stability and consequently postural balance during pregnancy. The hypotheses of the study are the following: (1) pregnant women who perform proprioceptive training, short-term, improve their postural balance, especially anterior-posterior sway (pre and post intervention) and compared to pregnant controls; (2) pregnant women who perform proprioceptive training (end intervention – 24 WG), short-term, maintain an improvement in body balance after 8 weeks of follow-up (32 weeks gestation), without training, compared to pregnant controls.
Materials and methods
Participants
Forty-two pregnant women (n = 42) aged between 25 and 30 years were recruited, based on the studies [11, 12], and randomized into blocks by physician practices in the obstetric department of the hospital. Three women did not attend the second visit, because they wished to withdraw from the study and also one who was relocating to another city. The evaluations were performed in the biomechanics laboratory of the university. The first evaluation was conducted at 20 WG, corresponding to the second trimester. All participants provided consent, based upon ethical approval by the Human Research Board of Local University with Clinical Trial Registry Number: 02694107.
Inclusion and exclusion criteria
The inclusion criteria were maternal age between 25 and 30 years, body mass index (BMI) not exceeding 30 kg/m2, low risk pregnancy, single fetus, and healthy sensory motor function in the lower limbs. Potential participants were excluded from the study if they would be one of the following: they were at less than 20 weeks gestation (WG); they were carrying more than one fetus; they had pre-eclampsia, toxemia, gestational hypertension, or previous abortion; or they were considered by their obstetrician to have a high-risk pregnancy.
Also excluded were women who had a history of Type I or Type II diabetes or any other condition that could affect sensation, a leg or foot fracture or ankle or knee sprain within the last year, current back or knee pain, history of cardiovascular, neurologic, neuromuscular, or pulmonary disease, vertigo, balance or any visual problems, or psychological illness. Similarly, pregnant women were excluded if they would be current smokers or if they would be currently taking any medication that may affect their ability to balance. Every woman who missed 3 sessions was excluded.
Design
This is a randomized controlled trial with blinding of participants and examiners. As participants were blinded to the knowledge of the group they would compose, since the participant chose a numbered envelope, which did not allow the participant to know the group that she would compose (control or intervention). Thus, the pregnant participants were randomized into blocks and allocated, using a simple, non-probability sampling method, to either the intervention group (PEG; n = 20), which performed proprioceptive exercise during one month, 3 sessions per week, or the control group (CG; n = 19); it was given an information pamphlet about usual care, information about how to adopt correct posture while sitting and standing, lifting, and carrying heavy objects, using support pillows and methods of turning over in bed or getting up from bed without exerting excessive strain on the lower back, but without education on proprioceptive exercise or physical therapy.
Sample-size calculation
The sample size was determined based on a pilot study by El-Shamy et al. [25]. The mean and standard deviation (SD) for the main outcome were measured by percentage of changes from the baseline during this previous study. Based on a sample with the power size estimation of the study beta of 80%, and in order to detect the effect size of difference 5%, with a significance level of p < 0.05, 15 participants were needed.
Intervention
The pregnant women randomized to the group that received proprioceptive exercises for one month was assessed at baseline and after 4 weeks (the end of the intervention), and during that time they undertook 3 sessions per week. The intervention group did not perform any other type of physiotherapy treatment during the intervention period, only the proprioceptive exercise program. The intervention group received training with the Cox® Proprioception Exercise Program [26] (Table 1), which consisted of exercises to improve static posture, including those involving one foot, walking, and ball exercises.
Exercises in the 4-week Cox® Proprioception training program
Exercises in the 4-week Cox® Proprioception training program
The training program was divided into 5 min. of slow walking, 10 min. of general warming up and proprioceptive exercises, ending with 5 min. cooling down exercises (Table 1). The intensity of the exercise was controlled by maternal pulse frequency (Pulse Meter POD-3, Japan). If the pulse frequency exceeded 140 beats per minute, the exercise would be stopped and the participant would be sent for the attention of a cardiologist from the local hospital, and would be excluded thereafter from the study. The physiotherapist responsible for proprioceptive training in the intervention group had experience in women’s health and prenatal care. Each training group consisted of 5 to 10 participants. Women in the intervention group received a handout illustrating and explaining the proprioceptive exercise program prior to the intervention.
Women in the control group did not receive specific instructions regarding proprioceptive exercise and were instructed not to perform any proprioceptive exercise during treatment period. This group were given only an information pamphlet, which included advice on normal care in addition to information about how to adopt correct posture while sitting and standing, lifting, and carrying heavy objects, using support pillows and methods of turning over in bed or getting up from bed without exerting excessive strain on the lower back, but without education on proprioceptive exercise or physical therapy.
It is important to emphasize that the pregnant groups evaluated (intervention and control) practiced some type of physical activity, such as walking or bodybuilding, but this was not measured. The groups of pregnant women were not prevented from performing physical activity, but the control group was oriented not to perform proprioceptive exercises training and physical therapy during the study period.
Dynamic balance assessments were performed using a Biodex Balance System®-BBS (Biodex, Inc., Shirley, NY, USA), which consists of a multiaxial standing platform that can be adjusted to provide varying degrees of platform tilt. A maximum of 20° of platform surface tilt can be selected. The Biodex proprioceptive protocol was used in the standing position (double-limb stance) on a platform without shoes or stockings. The participants were instructed to cross their arms over their chest to minimize the use of their arms in attaining balance, or to focus on a visual feedback screen directly in front of them and attempt to maintain the cursor in the center of the screen while standing on the unstable platform.
Three indices were electronically generated: (1) anterior/posterior index (AP), (2) medial/lateral index (ML), and (3) balance index. The balance index is believed to be the best indicator of the global postural stability (GPS) of a patient balancing on a platform. A higher score in all these outcomes indicates poorer balance. The BBS device has 8 levels of stability, ranging from level 8 (more stable) to level 1 (least stable). In theory, this “instability” should correlate with proprioception and neuromuscular response [26].
The BBS provides valid, reliable, and repeatable objective measures of a patient’s ability to balance on stable and unstable surfaces [26]. All measurements were performed at stability level 8. In order to assess balance, patients were asked to stand (double-limb stance) without shoes or stockings, with their eyes open, on the BBS device for 1 min. During the assessment period, the platform began to move freely and simultaneously to tilt about both axes (AP and ML). All postural balance measurements were repeated for 3 trials×20 seconds, with 30 seconds’ rest in between for both groups (PEG and CG) at 20, 24, and 32 WG, and the outcome of the 3 trials was collected, averaged by the software, and displayed to the right of the age-related predictive value for the analysis.
Data analysis
Means and standard deviations were calculated for each variable using descriptive statistics. The paired t-test was used to analyze and compare balance variables within each group (PEG or CG) and before and after intervention. The independent t-test was carried out to assess differences in the balance parameters between both groups (PEG and CG) before and after intervention (p-value < 0.05).
Results
A total of 39 pregnant women completed the 4-week intervention and were included in the analysis. No subjects dropped out from either group (PEG and CG) from 20 to 24 weeks gestation, but during the third trimester follow-up, 5 women in the PEG and 3 women in the CG dropped out for personal reasons. Hence, data were available for 39 women during the study and for 31 women during the third trimester follow-up (Fig. 1).
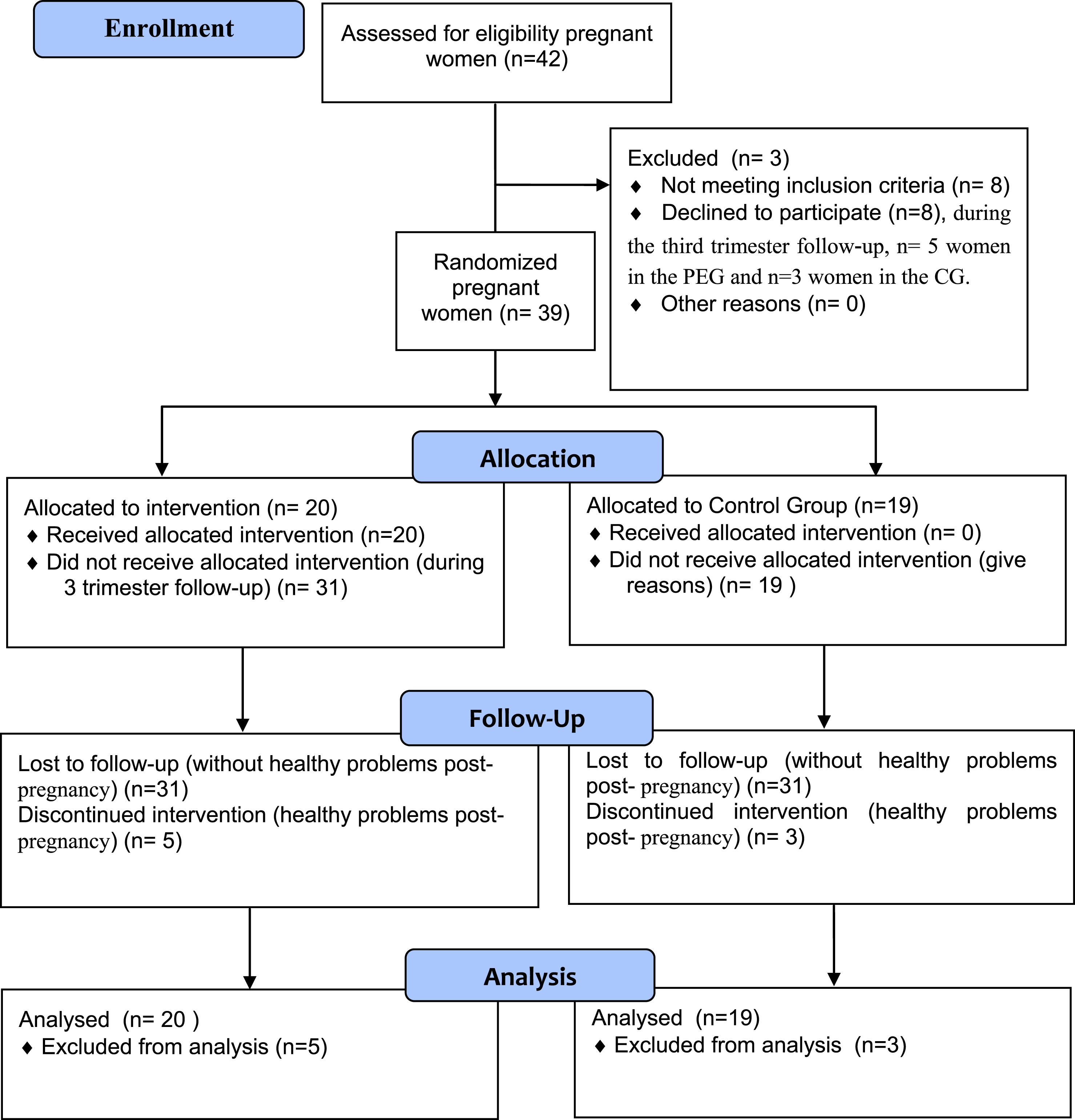
Flow chart of the study populations.
The PEG group (n = 20; age: 27.1±1.5 and BMI: 28.1±1.1 kg/m2). The CG group (n = 19; age: 27.6±1.1 and BMI: 27.9±1.8 kg/m2), without statistical differences between the groups (p > 0.05).
The pre-intervention showed no significant differences between groups (PEG and CG) for all dynamic stability indices (AP, ML, and GPS), as shown in (Table 2). Another important result was that after 4 weeks of post intervention, the PEG showed a decreased dynamic stability index (AP, ML, and GPS) compared to the CG, indicating an improvement in postural balance due to the intervention (PEG) (Table 2).
The comparative proprioceptive balance of participants in the PEG versus CG at pre and post-training program (between-group analyses)
Test t-student between groups*.
Table 3 shows a decrease and significant differences pre and post intervention, but only for dynamic stability (AP and GPS), in the PEG. In the CG, without intervention, variable none differed between 20 and 24 WG.
The comparative proprioceptive balance of females pre versus post training program for both groups (within-group analyses)
Test t-student between groups*.
All the dynamic stability indices remained the same between 24 WG (post training program) and 32 WG (follow-up) for the PEG, demonstrating the maintenance of improved stability after 8 weeks without intervention (32 WG) (Table 4). In the CG, the mean of the dynamic stability index increased, yielding significant differences between 24 and 32 WG.
The comparative proprioceptive balance of females at 24 versus 32 weeks gestation for both groups (within-group analyses)
Test t-student between groups*.
Table 5 shows that at 32 weeks gestation the mean of dynamic stability indices decreased in the PEG compared to the CG.
The comparative proprioceptive balance of females at 32 weeks gestation for both groups (between-group analyses)
Test t-student between groups*.
The purpose of the present study is to measure the effect of proprioceptive training, short-term, on dynamic postural balance during pregnancy and after 8 weeks of follow-up. The main findings of this study confirmed the first and the second hypotheses, and with the pre- and post-intervention the PEG showed decreased AP and GPS sway. After 4 weeks’ intervention, compared to the CG, the PEG showed decreased sway (AP, ML, and GPS indices), indicating an improvement in postural balance due to the intervention. In addition, after 8 weeks of follow-up (32 WG) the PEG demonstrated the maintenance and improvement of all the index of postural sway.
In the literature, the maintenance of postural balance requires the integration of the visual, vestibular, and somatosensory systems [26]. Joint afferents contribute to the central nervous system’s (CNS) function at three distinct levels of motor control [25]. At the spinal level, first level of motor control, nervous reflex movement patterns are received from higher levels of the nervous system. This provides for reflex splinting during conditions of abnormal stress about the joint and has significant implications for rehabilitation [27]. In the present study, a rehabilitation program was developed that incorporated proprioceptive control of the joints, which is necessarily related to an appreciation of the central nervous system’s (CNS) influence on motor activities. Thus, one possible explanation for the positive effect of intervention in the PEG compared with the control group (CG) may be attributed to the improvement of the action of the ankle-foot articular receptors, which may have improved the communication of the receptors with the nervous system peripheral nervous system to the postural balance control circuits.
Another possible explanation is that partial differentiation of joint afferent receptors has also been shown to alter the musculature’s ability to provide co-contraction joint stabilization by antagonistic and synergistic muscles [28]. Although the present study did not perform electromyographic evaluations of the muscles of the lower kinetic chain of the pregnant woman, to verify this possible muscular activation, these reports in the literature help to understand the maintenance of a better postural stability of the pregnant woman after 8 weeks of completion of the intervention with proprioceptive training program (PEG) compared to the CG.
The proprioceptive training program conducted in the present study improved the joint mechanoreceptor activation, which results in improved balance adjustment in pregnant women. This fact was also observed with regard to postural control, and explained by the proprioceptive training delivered in the study by An et al. [29], despite the presence of participants with knee injury. In addition, movements that are repeated can be stored as central commands and can keep the information for the joint proprioceptors [25], which may explain the maintenance of the postural balance of the pregnant woman after 8 weeks of follow-up of the intervention group (PEG).
Numerous investigators have examined different aspects connected with postural stability during pregnancy. Jang et al. [9] found greater anterior-posterior and radial sway and a wider preferred stance breadth in pregnant women during a quiet stance. Jang et al. [9] and Ribas and Guirro [19] found significant decreases in postural balance during the last trimester, associated with increased anterior-posterior displacement. Butler et al. [13] concluded that postural stability gradually decreases during pregnancy and remains reduced up to 6–8 weeks after childbirth. These studies emphasize the importance of the anterior-posterior sway for improved postural stability during and after pregnancy. In this line of reasoning, an important clinical finding of the study is the improvement of the anterior-posterior sway of the pregnant women after the intervention and after 8 weekly follow-up of PEG.
The clinical relevance of this study was not verified in intervention studies in the literature for improving balance in pregnant women, although much evidence exists for the disturbance of balance during pregnancy, and a review of studies [10, 30] identifies this as an important clinical problem, which must be encompassed within the rehabilitation process during pregnancy [30]. El-Shamy et al. [25], consistent with the findings of this study, demonstrated that pregnant women’s stability indices significantly increased from the second to the third trimester, and that they had decreased postural stability during pregnancy. The relaxin and estrogen hormones have been identified, in some studies, as contributors to these postural and ligamentous laxity changes [4, 5].
Despite all these changes, it was observed in this study that the proprioceptive training allowed better joint stability and balance control (AP and ML sway) in the second (24 WG) and third trimester (32 WG) of pregnancy. Another important result was that no significantly different ML was found at stability level 8 during the second trimester in either group (PEG and CG), but it significantly increased during the third trimester in the CG compared to the PEG; this can be explained by the fact that, when the feet are kept together, the support base is analogously configured as a square, with the center of gravity (COG) representing the midpoint between the two directions. Likewise, it is believed that, by separating the feet, the support base expands, which decreases the ML displacement in relation to AP [30].
One limitation of our study is that it took no account of changes in the psycho-physiological, social, physical activity and cultural level of the participants, which may or may not have had an influence on the results, although no studies in the literature suggest that such an influence exists.
Conclusion
Proprioceptive training, short-term, was effective in promoting reduction of postural sway during pregnancy, especially anteroposterior oscillation and postural balance. This improvement was maintained for all the oscillations, anteroposterior, mediolateral, and global postural, at 8 weeks follow-up (32 WG).
Authors’ contributions
Both authors have made substantial contributions to the conception and design, collection of data, or analysis of data in this study; they have also contributed to drafting the manuscript or revising it critically for important intellectual content. All the authors have read and approved the final manuscript.
Conflict of interest
Authors have declared that no competing interests exist.
Footnotes
Acknowledgments
The authors gratefully acknowledge all the participants, physicians, physiotherapists, and nurses for the effort they devoted to this study.