
Abstract
BACKGROUND:
Median nerve neurodynamic testing is described in the literature with the scapula blocked and depressed and there are numerous descriptions of structural differentiation performed during testing. A better understanding of how these variables impact median nerve neurodynamic testing is warranted.
PURPOSE:
To compare the Upper Limb Tension Test A (ULTT A) with the scapula blocked and depressed to determine: the reliability of ULTT A with the scapula blocked and depressed; if there is a statistically significant difference between the left and right arms; and if there is a statistically significant difference for ULTT A with the scapula blocked or depressed.
METHODS:
This was a intertester and test-retest reliability and accuracy study. Elbow extension was measured with a standard goniometer. Sensory responses were captured with the Numeric Pain Rating Scale (NPRS). Subjects were randomly tested by Rater, side, and by test condition.
RESULTS:
The NPRS and end range elbow extension had moderate to good intertester reliability. There were poor to moderate findings for reliability of structural differentiation. There was no statistically significant difference (p > 0.05) between the left and right arms except for structural differentiation. There was a statistically significant difference between the scapula blocked vs scapula depressed test conditions except for the NPRS on the left arm (p = 0.08).
CONCLUSIONS:
ULTT A under the depressed scapula test condition is less reliable and more variable than the blocked scapula condition in the normal healthy population. Structural differentiation may not be a reliable or valid aspect of ULTT A.
Introduction
The Upper Limb Tension Test A (ULTT A) of the median nerve is used in clinical practice as part of a diagnostic test cluster for cervical radiculopathy (ULTT A, cervical rotation to the involved side less than 60°, distraction test, and Spurling A test) [2]. Wainner and colleagues also reported that ULTT A was the most useful test for ruling out cervical radiculopathy [2]. Although the study that established the diagnostic test cluster for cervical radiculopathy is considered to be of high methodological quality [8] and is included in the Neck Pain Revision 2017 Clinical Practice Guideline [9] as level 2 evidence [10], this work has yet to be validated prospectively.
Since the publication of the diagnostic cluster for cervical radiculopathy in 2003, there has been an evolution of understanding regarding neurodynamic testing of the median nerve. The diagnostic cluster for cervical radiculopathy described ULTT A as involving scapular depression consistent with a description by Elvey in 1994 (11). In addition, the diagnostic cluster for cervical radiculopathy described structural differentiation as part of ULTT A as involving contralateral cervical side bending that increased sensory responses or ipsilateral cervical side bending that decreased sensory responses [2]. In a clinical commentary in 2012, Nee and colleagues described the Upper Limb Neurodynamic Test 1 (ULNT 1) for the median nerve as including blocking of the scapula from elevation while performing the test [12]. This description was consistent with previous descriptions of this test by Elvey in 1997 [13], Hall and Elvey in 1999 [14], and Butler in 2000 [8]. For the ULNT 1, Nee et al. described structural differentiation as contralateral cervical side bending that increases sensory responses in the forearm and the release of wrist extension that decreases sensory responses [12].
Shacklock provides a third definition of median nerve neurodynamic testing called Median Neurodynamic Test 1 (MNT 1) [15]. In contrast to the ULTT A as described in the diagnostic cluster for cervical radiculopathy [2] and consistent with the description by Nee [12], the scapula is blocked from elevation during testing [15]. In contrast to the other procedures, Shacklock suggests that patients are unable to accurately perform contralateral cervical side bending for structural differentiation as the final component of the test secondary to the patient potentially not wanting to create a significant change in neural tension [15]. He therefore suggests that the MNT 1 procedure start by positioning the patient in contralateral side bending at the cervical spine [15]. He describes structural differentiation at the end of the test as the patient returning their neck to the neutral position to see if it relieves distal sensory responses if provoked or the release of wrist extension if proximal sensory responses are provoked [15].
There are therefore many operational definitions of neurodynamic testing of the median nerve in the literature. Recent consensus suggest that the scapula should be blocked and not depressed during the testing procedure and that structural differentiation should involve a distal maneuver for proximal symptoms and a proximal maneuver for distal symptoms [12–16]. It has been repeatedly demonstrated that altered sensory responses occur with neurodynamic testing of the median nerve in the asymptomatic population [16–20]. It is therefore important to identify what a normal response is to this testing so that it can be differentiated from an abnormal response.
Utilizing a healthy, asymptomatic population, the purposes of this study was to determine: 1) the intertester and test-retest reliability of the onset of sensory responses during elbow extension during ULTT A with the scapula blocked and depressed; 2) the intertester and test-retest reliability of the magnitude of sensory responses during ULTT A with the scapula blocked and depressed; 3) the intertester and test-retest reliability of structural differentiation as part of ULTT A with the scapula blocked and depressed; 4) if there is a statistically significant difference between the left and right arms for the two testing conditions; and 5) if there is a statistically significant difference for ULTT A with the scapula blocked or depressed.
Methods
Design and raters
This was an intertester and test-retest reliability study. The protocol was approved by a University Institutional Review Board. The reporting of this study follows the Guidelines for Reporting Reliability and Agreement Studies (GRRAS) [5]. The Raters for this study were two licensed physical therapists, each with more than 14 years of experience. One of the Raters was board certified in Sports and the other was certified in Orthopaedics through the American Board of Physical Therapy Specialties.
Participants-sample size
We determined that 45 participants would be an appropriate sample size based on the methodology and rationale of Oliver and Rushton who performed a similar reliability study on ULTT A utilizing an asymptomatic population of physical therapy students [21]. Participants included students enrolled in the College of Health Professions and the College of Nursing that were able to participate in testing on two separate days at least 1 week apart. Participants were excluded if they: had the presence of any cervical or upper extremity symptoms [22]; had a history of cervical or upper extremity neurological symptoms [23]; had a muscular or joint mobility restriction that would hinder the proper execution of ULTT A [24]; had an inability to lay supine comfortably for the amount of time required to properly perform ULTT A [25]; were pregnant; or had a history of systemic illness such as rheumatoid arthritis.
Equipment
Elbow extension during the ULTT A was measured utilizing an 8-inch standard goniometer (Model 47; 8 ×0.2 ×2 inches; 0.64 ounces, Prestige Medical, Northridge, CA). The absolute maximal error (±2 standard deviations) has been reported to be 10.3° for measuring elbow extension [26].
Procedure
Individuals that met the inclusion and exclusion criteria and were willing to participate in the study were screened and provided informed consent. Screening was performed for subjects that had a history of cervical or shoulder dysfunction or were unsure if they had any symptoms related to their cervical spine or shoulders.
The participants were positioned supine on a treatment table with the cervical spine in a neutral position with their nose pointed towards the ceiling during testing on both days [21]. Pillows and towels were not used for head support. The height of the treatment table was set at the level of the greater trochanter for the Raters. The starting position for testing was 45° of shoulder abduction; 90° of elbow flexion; neutral forearm and fingers (mid-way between end-ranges); opposite arm resting at the side of the body; and both legs fully extended and not crossed over one another. Participants were randomly tested by Rater (1 or 2), side (Left or Right), and by test condition (Blocked or Depressed). For the blocked condition, a knuckled hand with the palm toward the participant’s shoulder was placed superior to the acromion to prevent shoulder elevation during the testing procedure. For the depressed condition, the same position was attained except the shoulder girdle was maximally depressed and then held in place during the testing procedure. The sequence for testing followed the sequencing described by the diagnostic test cluster for cervical radiculopathy [2] and Elvey [11]. The only variability was that step 1 of the procedure was under one of two conditions (scapula blocked or depressed). The sequence of the procedure was: 1. Scapula (Blocked or Depressed); 2. Shoulder abduction to 90° 3. Full forearm supination, with wrist and finger extension to include the thumb; 4. Full shoulder external rotation; 5. Elbow extension to the first onset of sensory response or discomfort (SR1) or when resistance prevented further elbow extension (R2); 6. Contralateral cervical side-bending; and 7. Ipsilateral side bending. Participants actively moved themselves into the ipsilateral and contralateral cervical side bending positions and held themselves there long enough to answer the question if their sensation or discomfort increased, decreased, or stayed the same. If the participant had discomfort at any point during the testing sequence, that trial was terminated at that point and the step number that the participant was able to complete was recorded. If participants had any change in sensation or discomfort that persisted following the testing at any stage of the protocol that did not resolve within 5 minutes, testing was terminated.
The landmarks that were utilized to measure elbow extension at 90° of shoulder abduction to ensure the goniometer was appropriately aligned were the ulnar styloid process, medial epicondyle of the humerus, and anterior aspect of the acromion process [20]. Sensory response was recorded utilizing a 0 to 10 Numeric Pain Rating Scale (NPRS) as the elbow was extended from a flexed position at SR1 . The angle of elbow extension was also recorded at SR1. If sensory responses were not provoked the angle of elbow extension at R2 was recorded [20, 28]. If the participant could not tolerate the test position of 90° of shoulder abduction and at least 90° of shoulder external rotation secondary to the onset of sensory responses, the trial was terminated and the last completed maneuver was recorded.
A researcher not performing the testing procedure recorded the elbow extension measurement for SR1 or R2 for the participants’ left and right sides to maintain blinding of the Raters. In order to control for order effects, the selection of the Rater that tested the participant first was randomized by flipping a coin. In addition, the order sequence of where the Rater started for the 4 test conditions was also randomized by flipping a coin for the side (left or right) and condition (blocked or depressed). The average of three tests was used for the final determination of the NPRS at the end range of elbow extension and for elbow extension range of motion. The prevailing two out of three responses were utilized to determine if contralateral or ipsilateral cervical side bending increased sensory responses, decreased sensory responses, or if there was no change in sensory responses for ULTT A with the scapula blocked and depressed. If the participant did not have a sensory response at the end of the neurodynamic test, it was recorded as a 0 on the NPRS, no change for the structural differentiation, and the degrees of elbow extension was recorded at R2.
Data analysis
Descriptive and inferential statistics were used to answer the research questions. We did not anticipate the amount of missing data secondary to the number of normal healthy participants that were unable to tolerate the protocol under the depressed scapular condition.
We were concerned that commonly utilized techniques for imputing missing data such as carrying the last observation forward or utilizing the average of responses would artificially inflate the reliability statistics. We also could not utilize the automatic multiple imputations feature in SPSS version 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. IBM Corp., Armonk, NY) secondary to its inability to calculate the reliability statistics of interest (Quadratic Weighted kappa, ICC2,3, and kappa). We therefore first sought to determine if there were any statistically significant differences between Raters 1 and 2, Left and Right arms, blocked and depressed test conditions, and between Visits 1 and 2 for the testing parameters of interest utilizing the multiple imputation feature in SPSS. We then performed the same analysis utilizing only complete data in MedCalc for Windows, version 18.5 (MedCalc Software, Ostend, Belgium). We then compared to see if there were any differences in the results between the two different statistical analyses. Since there was no difference in the statistical findings between the analyses performed utilizing the multiple imputation feature in SPSS and the original data utilizing MedCalc, we performed the data analysis using MedCalc and the original complete data in order to answer the research questions. This was also done in order to retain the medians and confidence intervals that are lost with calculations utilizing pooled data from multiple imputations. The data did not meet the parametric assumptions. The Quadratic Weighted kappa with a 95% confidence interval was used to assess reliability for the NPRS secondary to the interpretation that this data was ordinal and non-linear [29]. The ICC2,3 was used secondary to the ratio level goniometric data that was collected for elbow extension. The ICC2,3 values were interpreted as less than 0.4 = poor, 0.4 to 0.59 = fair, 0.60 to 0.74 = good and 0.75 or greater as excellent reliability [6]. Kappa values were interpreted as: 0.0–0.20 = slight, 0.21–0.40 = fair, 0.41–0.60 = moderate, 0.61–0.80 = substantial, and 0.81–1.00 = almost perfect [7].
Since the data was not normally distributed, the Mann-Whitney U was used to determine if there were any statistically significant between-group differences for the NPRS and elbow extension goniometric measurements. Since the data for structural differentiation was nominal, a chi square analysis was used to determine if there were any statistically significant between group differences.
Results
Descriptive statistics
Figure 1 outlines how the participants moved through the study. Fifty participants arrived for testing. Forty-seven met the inclusion/exclusion criteria, agreed to participate, and signed informed consent. Four participants were lost to follow-up. Three participants were still symptomatic at their second visit and 1 of the participants did not show up for their follow-up appointment. This left 43 participants that were available for data collection for Visits 1 and 2. The characteristics of the sample for the study are included in Table 1. The numbers and percentages of participants that had missing data secondary to not being able to attain the test position by arm, Rater, and test condition are shown in Table 2. The numbers of participants that had complete data for the analyses performed are also shown in the tables.
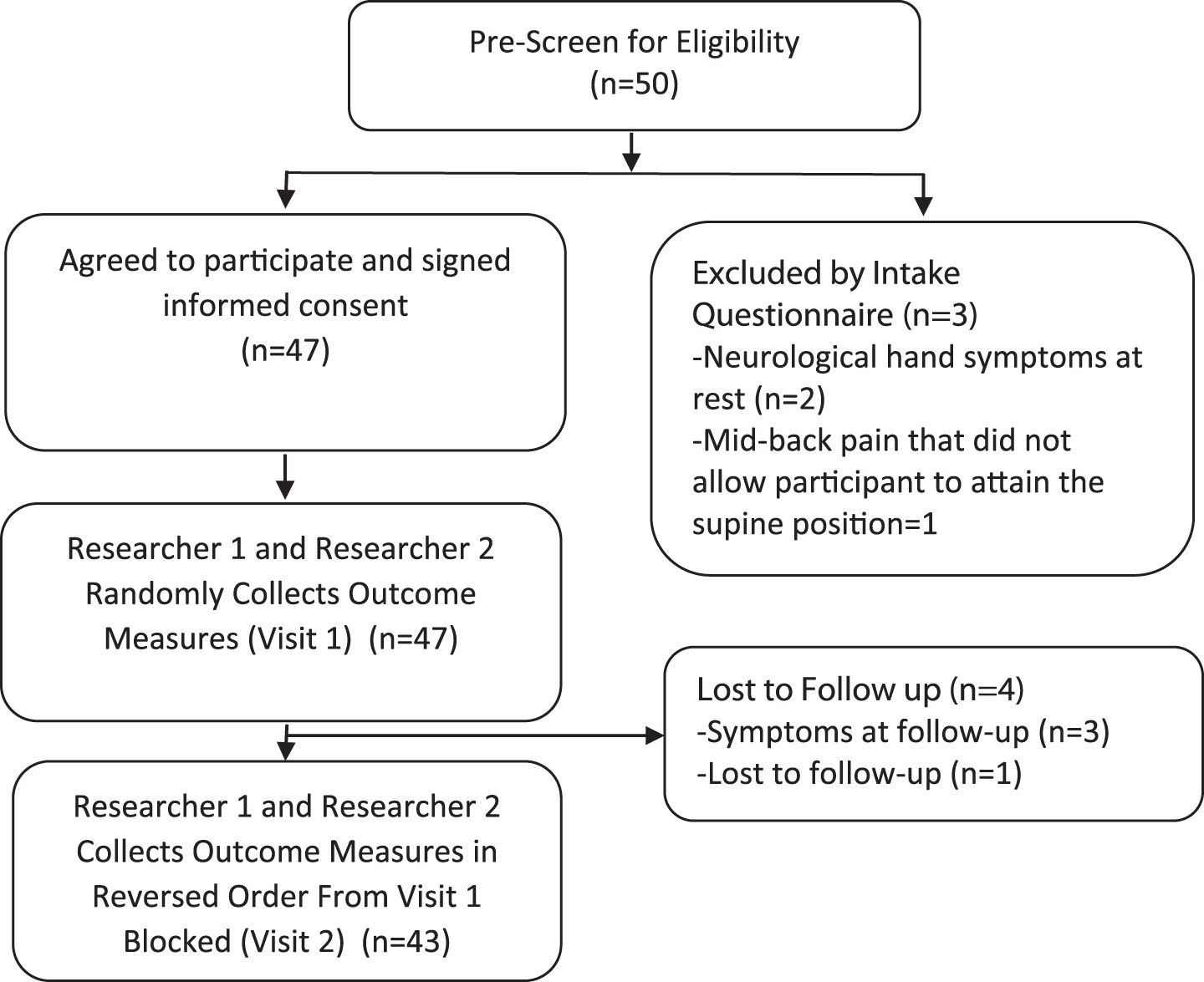
Flow of the study.
Sample Characteristics
*Data are medians & (minimum to maximum).
Participants that could not attain the test position by shoulder, tester, and test condition*
*Data are frequency counts and percentages
Table 3 provides the result for intertester reliability and Tables 4 & 5 provide the results of test-retest reliability for Raters 1 and 2. Intertester reliability and test-retest reliability for Rater 1 was moderate to substantial for the NPRS at the end range of elbow extension; excellent for the blocked and depressed condition for degrees of end range elbow extension; fair to moderate for contralateral side bending; and substantial for ipsilateral side bending.
Intertester Reliability of Rater 1 & 2 for Right and Left Arms Visit 1
Intertester Reliability of Rater 1 & 2 for Right and Left Arms Visit 1
*Quadratic Weighted kappa. †ICC2,3. ‡kappa.
Test-Retest Reliability for Right and Left Arms Rater 1
*Quadratic Weighted kappa. †ICC2,3. ‡kappa.
Test-Retest Reliability for Right and Left Arms Rater 2
*Quadratic Weighted kappa. †ICC2,3. ‡kappa.
Test-retest reliability for Rater 2 was substantial for the NPRS at end range elbow extension for the left and right arms. Reliability was excellent for the degrees of end range elbow extension for the blocked and depressed condition for the left and right arms, slight to moderate for contralateral side bending, and moderate to substantial for ipsilateral side bending.
There were no statistically significant differences between the left and right arms or between Rater 1 and Rater 2 for the NPRS or for degrees of elbow extension under the blocked or depressed condition (p = 0.25–0.97) (Table 6). A Chi-square analysis determined that there were statistically significant differences between the left and right arms and between Raters 1 & 2 for a 3×3 comparison of the reporting of increase, decrease, or no change in sensory responses for contralateral side-bending and for ipsilateral side-bending (p < 0.01).
Differences Between Left and Right Shoulders for Tester 1 and 2 for All Test Conditions Visit 1
Differences Between Left and Right Shoulders for Tester 1 and 2 for All Test Conditions Visit 1
*Data are medians & (95% Confidence Intervals). †Mann Whitney U Test.
There were statistically significant differences between the scapula blocked and scapula depressed conditions for Raters 1 & 2 for the NPRS and degrees of elbow extension for the left and right arm (p≤0.02) except for the NPRS for Raters 1 and 2 on the left arm (p = 0.08) (Table 7). A Chi-square test determined that there were also statistically significant differences between the scapula blocked and scapula depressed conditions for a 3×3 comparison of the reporting of increase, decrease, or no change in sensory responses for contralateral side-bending and for ipsilateral side-bending for Raters 1 & 2 (p < 0.01).
Differences Between Scapula Blocked and Depressed for Tester 1 and 2, Visit 1, for the Left and Right Shoulder
Differences Between Scapula Blocked and Depressed for Tester 1 and 2, Visit 1, for the Left and Right Shoulder
*Data are medians & (95% Confidence Intervals). †Mann Whitney U Test.
Our findings suggest that the sensory response (NPRS) at the end range of elbow extension and the degree of end range elbow extension during the test have moderate to good intertester reliability independent of test condition (Blocked vs. Depressed). The poor to moderate findings with large confidence intervals for ULTT A structural differentiation tests (Contralateral and Ipsilateral side bending) suggest that these maneuvers may not be reliable. This is similar to what was observed for Raters 1 and 2 for test-retest reliability with moderate to good reliability observed for the NPRS at the end range of elbow extension and degree of end range elbow extension during the test and poor to good reliability observed with structural differentiation. The statistically significant differences between the left and right arms and between Raters 1 & 2 for structural differentiation in asymptomatic participants suggests that ULTT A as part of the diagnostic test cluster for cervical radiculopathy may not be valid. The statistically significant differences between the scapula blocked and scapula depressed conditions suggests that depressing the scapula significantly changes the test.
Legakis and Boyd performed a study comparing neurodynamic test responses with ULTT of the median nerve with the scapula blocked from elevation and with the scapula depressed in the dominant limb for elbow extension range of motion at the end of the neurodynamic test [16]. In their study, they reported excellent reliability of the ULTT with the scapula blocked and scapula depressed with ICC2,1 values of 0.93 (95% CI: 0.60–0.99) and 0.92 (95% CI: 0.56–0.99), respectively [16]. The average for elbow extension at the end of the test sequence was 144.7° (19.1° SD) with the scapula blocked and 139.5° (20.6° SD) with the scapula depressed [16]. Based on the average increase of 5° of elbow extension with the scapula blocked, the authors recommended utilizing this test sequence to allow further excursion of the nerve during testing [16]. The authors did not compare the left side to the right side in order to determine if this difference of 5° is a normal variant when testing the normal healthy population [16]. They also did not include structural differentiation that is considered a key component of neurodynamic testing [12, 20]. Consistent with other studies [21, 27] this study used an electrogoniometer [16]. Besides our study, the only study that compared left and right sides using a goniometer in a healthy population reported that an inter-limb difference of more than 15° for the median nerve was a meaningful difference [27]. This suggests that the 5° difference between testing the median nerve with the scapula blocked vs depressed may not be a clinically meaningful difference [16]. In addition, the use of an electrogoniometer may not be generalizable with the goniometric measurements that are typically utilized in the clinical setting.
In our study, we utilized structural differentiation as defined by the diagnostic test cluster for cervical radiculopathy as contralateral and ipsilateral side bending in a normal asymptomatic population. This is in contrast to the work of Nee et al. [12] and Shacklock [15] that suggest using the cervical spine for structural differentiation of distal sensory responses and the wrist for structural differentiation of proximal sensory responses. Additionally, Schmid et al., suggested that the clinician could use the wrist, shoulder girdle, or any combination of these structural differentiation maneuvers at their discretion if the patient’s response was “unclear” in a symptomatic population [30]. Based on the impact of the movement sequencing of the sciatic and tibial nerve during a straight leg raise (SLR) in an embalmed cadaver model, Boyd et al. suggest that the movement sequence of neurodynamic testing does not matter [31]. This is inconsistent with the findings of Gilbert et al. that reported prepositioning the ankle into dorsiflexion prior to performing the SLR produced a significantly larger displacement of the nerve in unembalmed cadavers [32]. The conclusion that the movement sequence does not matter may be premature. Boyd reported that releasing the scapula from a blocked position decreased or eliminated sensory responses 90% of the time and did not change sensory responses 10% of the time for the dominant and nondominant limbs in an asymptomatic population as the final component of structural differentiation when performing ULNT 1 [17]. This interlimb symmetry occurred as significant asymmetries were present between the dominant and nondominant limbs for structural differentiation involving ipsilateral and contralateral cervical side bending [17]. This suggests that adding or releasing scapular depression in a normal heathy asymptomatic population has the ability to change the neurodynamic findings 90% of the time. This is consistent with the findings of Davis et al. that used scapular depression during ULNT 1 and observed altered sensory responses in 86.9% of asymptomatic healthy individuals [19]. Given our findings in conjunction with the findings of Boyd [17] and Davis et al. [19] in an asymptomatic healthy population, introducing scapular depression may have a significant impact on upper extremity neurodynamic excursion and sensory responses in the asymptomatic population that may create a large percentage of positive sensory responses when somebody becomes symptomatic.
When we designed this study, we did not anticipate the number of normal healthy participants that would not be able to complete the protocol as described by the diagnostic test cluster for cervical radiculopathy, predominantly under the depressed scapular condition. We discovered 1 (2.1%) participant that could not complete the protocol with the scapula blocked. There were 9 (19.9%) participants that could not complete the test sequence with the scapula depressed and as many as 5 (10.6%) participants that could not complete the test on either upper extremity with the scapula depressed. Given that 3 participants still had a sensory response at their second visit and as many as 9 normal healthy participants could not tolerate shoulder external rotation under the depressed scapula condition, the depressed version of this test should be reconsidered and possibly eliminated.
This study has several limitations. This study was performed on a young healthy population. Our findings therefore are not generalizable to the general asymptomatic or symptomatic population. Our testing procedure involved taking the average of three measurements under four test conditions (Rater 1 blocked, Rater 1 depressed, Rater 2 blocked, and Rater 2 depressed) bilaterally. Although all conditions were randomized to ensure that there were no ordering effects, there may have been differences between the first and last tests from which the averages were determined that may have increased variability. We also did not specifically record the location, distribution, or type of sensory changes experienced. This information descriptively could provide valuable information regarding what a normal response to this test is.
For neurodynamic testing of the median nerve to be valid, sensory responses have to be reliably reproduced in the asymptomatic and symptomatic population and the sensory responses should be significantly different between these two populations. If there are statistically significant differences in sensory responses between these two groups, the sensory responses should change in response to treatment and the sensory responses of the symptomatic population should approach the sensory responses of the asymptomatic population. Failure to meet these criteria in logical framework that connects the neurodynamic assessment to the diagnosis, the diagnosis to the treatment, and the treatment to the outcome significantly hinders the assessment of the clinical utility of this treatment paradigm [33].
Conclusion
In our study, we found that elbow extension and the magnitude of sensory changes can be reliably assessed in a healthy asymptomatic sample and that there were no statistically significant differences between the left and right sides for these measures. Consistent with the findings of Boyd [17], we found that structural differentiation involving ipsilateral and contralateral side bending was statistically different between the left and right sides in the normal asymptomatic population. Clinically, neurodynamic testing is used to compare a symptomatic side to an asymptomatic side to determine if the test is positive. Given that asymmetry is a normal finding in the asymptomatic population, this testing procedure may not be valid in the symptomatic population. Our findings suggest that elbow extension, the magnitude of sensory changes, and structural differentiation assessed during the performance of ULTT A may be different with the scapula blocked as compared to depressed. This finding suggests that ULTT A may be a different test if it is performed with the scapula blocked or depressed and that a clinician’s choice to use the shoulder girdle for structural differentiation may significantly change the test.
Further research of ULTT A is necessary to establish what a normal response is in the normal healthy population. In order to do this, the test should be refined to ensure that all normal healthy participants can complete the testing procedure. The testing parameters should also be refined to ensure that the test is reliable and not statistically different between the left and right upper extremities in the normal healthy population.
Conflict of interest
None to report.
Funding
Funding was not provided for this study.