
Abstract
BACKGROUND AND PURPOSE:
Shoulder injury is common in cricketers, with disorders of the upper-limb accounting for up to one fifth of the total number of injuries in modern-day cricket. Pain and cross-season loss of range of motion of the dominant side have been demonstrated in over-head throwing athletes, but only limited data exists concerning cricketers. We aimed to inform injury prevention and management strategies by determining whether elite cricketers demonstrated altered shoulder range or strength, and whether this related to pain presentation, across a competitive period.
METHODS:
Eighteen male professional county cricket players (mean±SD) aged 24.0±4.3 years, 1.8±0.1m height, and 83.6±7.7kg body mass underwent shoulder range-of-movement (ROM), strength, and pain assessment using the Kerlan-Jobe Orthopaedic Clinic (KJOC) Shoulder and Elbow score on two separate occasions at least 12 weeks apart (13.2±1.0), over the course of a competitive season.
RESULTS:
One third of all players tested reported playing with shoulder pain at some stage during season. Both dominant (20°±11.8°) and non-dominant (14°±14.7°) throwing arm Total Arc ROM increased between testing intervals (p≤0.01), with significant concomitant increases in player external rotation (ER) ROM of both dominant (11.6°±8.4°) and non-dominant (8.8°±6.4°) throwing arms (p≤0.01). The dominant shoulders of prospectively injured players demonstrated a reduction in ROM (mean Total Arc ROM difference of -17.3°±6.2° vs -0.6°±11.8°), and lower dominant ER:IR strength ratios mean ER 0.71±0.13 vs IR 0.93±0.21) at baseline testing compared to non-injured players. ER strength decreased in both arms (p≤0.01), while ER:IR DOM strength ratios were significantly lower than at pre-season (mean loss of 16–18±21N/0.2±0.25 ER MVIC NBW per side, p≤0.05).
CONCLUSION:
Professional county cricket players exhibit increases in shoulder ROM and decreases in dominant throwing arm strength ratios across a competitive Cricket season. Pre-season differences in dominant vs non-dominant shoulder ROM and dominant throwing arm shoulder strength ratios appear to be associated with prospective onset of in-season shoulder trouble in the professional cricketers studied.
Introduction
Recent studies have identified that shoulder injury amongst elite and professional cricketers is common, with previous data suggesting that up to 23% had a throwing related shoulder injury and/or pain in the dominant throwing arm which routinely affected players performance and choice of fielding position at any one time [1–4]. Whilst disorders of the upper-limb account for one fifth of the total number of injuries in modern-day cricket, it has been estimated that a diagnosis of primary or secondary glenohumeral joint impingement accounts for 75% of all shoulder related throwing injuries in cricketers [1–4].
Given the magnitudes of inferior force and adduction torque produced during the cocking, acceleration and deceleration phases of overhead throwing technique [3, 7], it is well established that the execution of optimal throwing biomechanics and optimising of individual player bowling and throwing volumes and workloads is essential to the overall maintenance of stability, mobility, and structural integrity of the glenohumeral joint during these actions [4–11]. Authors have postulated that the maintenance of appropriate range of movement (ROM), strength ratios, and rotator cuff activation patterns at the glenohumeral joint may be instrumental in the prevention of a plethora of acute shoulder injuries and chronic pathologies [8–16]. Previous studies have attempted to use static measurements of athletes’ glenohumeral ROM and dynamometry strength measurements of internal and external rotator musculature ratios, in the attempt to identify causal relationships between specific clinical and physiological indices and prospective incidence of injury in overhead throwing athletes [3, 16–29].
To date there is limited cricket-specific data available on player glenohumeral joint anthropometric and physiologic parameters, and how they may relate prospectively to the onset of shoulder pain and injury in professional Cricket. Further studies are required to establish in-season variations in glenohumeral joint ROM and strength, and their resultant impact upon player participation and performance in this group [2, 31]. Therefore, the aim of this study was to establish data on shoulder ROM, rotator and hand grip strength in a cohort of professional first class county cricket players to examine whether these variables were associated with the onset of shoulder pain/injury during the 2011 season.
Methods
Participants and data collection
In this observational cohort study, 18 male professional cricket players were recruited from three county cricket clubs, and underwent upper-limb musculoskeletal profiling on site at squad training bases on two separate occasions. After training in all outcome measures one experienced sports physiotherapist (JP), conducted all data collection.
Baseline pre-season data collection took place prior to the start of competitive fixtures (‘0 weeks’), and then opportunistically at least 12 weeks post baseline measures (mean 13.2 weeks) following > 24 hour break from throwing activities to allow sufficient recovery time from competition/acute effects of throwing [23]. All consenting participants were tested, including those who reported shoulder pain, as long as they continued to participate in training and games, and were cleared to do so by club medical staff. Participants who had previous shoulder or neck surgery within the year before testing and bowled with one arm but preferentially threw with the other were excluded from analysis as per previous methods. Ethical approval was approved by Queen Mary Research Ethics Committee.
Study outcome measures/variables
Shoulder ROM
Shoulder ROM and thoracic combined elevation was measured using a Solatronic digital inclinometer (model EN17) and tape measure, as per previous methods by Giles et al. [3] and Dennis et al. [31]
Shoulder strength
Internal and external Glenohumeral joint rotator maximal voluntary isometric contraction (MVIC) measured using a Lafayette Manual Muscle Testing hand-held dynamometer [25].
Hand grip strength
JAMAR® Plus digital HHD hand grip strength (Kg) scores were used as per previous methods [34].
In-season player upper-limb function/injury status
The Kerlan-Jobe Orthopaedic Clinic (KJOC) Shoulder and Elbow score was used in order to evaluate players’ current function and injury status at time of testing [35].
Data analysis
Descriptive statistics were used to present recorded data, which were reported as the arithmetic mean (M)+standard deviation (SD). Pre-season and in-season repeated measures were analysed using paired sample t-tests, with a level of significance set at p≤0.05), using Statistical Package for the Social Sciences (SPSS) Statistical software (IBM, Version 20). Cohen’sdwas used to determine the effect size between the mean difference of pre-season and in season measurements. Graphs were formulated using Microsoft Excel software.
Results
Player characteristics are summarized in Table 1, whilst the variables of the study are summarized in Tables 2 and 3. 18 first-class county cricket players completed repeated measures data sets, eleven of which were Fast-Bowlers, three Slow-Bowlers, and four ‘Specialist Batsmen’.
Player characteristics
Player characteristics
Player Shoulder ROM & Kerlan-Jobe Orthopaedic Clinic (KJOC) score results
*Difference between pre-season and in-season scores (p≤0.01).
Player Shoulder Strength, calculated ER:IR Ratios, & JAMAR Handgrip results
**Difference between pre-season and in-season scores (p≤0.01), *(p≤0.05).
At baseline pre-season testing, players tended to exhibit a reduced ROM in their dominant throwing arm compared to their non-dominant throwing arm, precipitated by a loss of corresponding dominant IR ROM (Table 2, Figs. 2 & 3). Nonetheless, despite this typical dominant GIRD pattern, most cricketers in the initial sample (n = 34) exhibited Total Arc ROM in the region of 180° bilaterally [38], with the exception of the wicketkeepers who tended to have reduced Total Arc ROM compared with the overhead bowlers and specialist batters. Specialist Batsmen generally exhibited greater non-dominant ER ROM and dominant to non-dominant Total Arc ROM differences than Fast-Bowlers, whilst they also displayed greater dominant to non-dominant GIRD than Slow-Bowlers, at baseline testing.
Flow diagram of study data collection process.
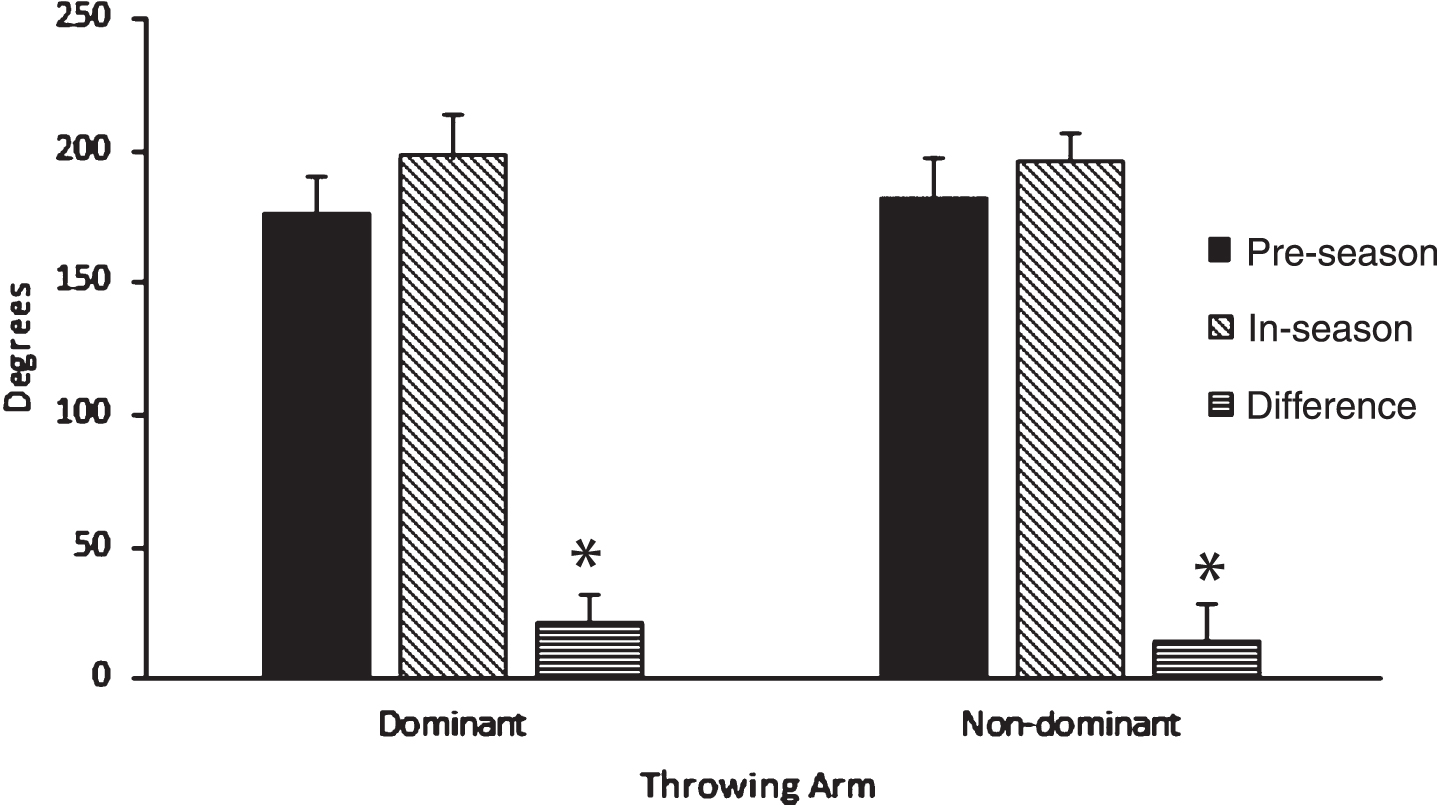
Pre and In-season Player Glenohumeral Joint Total ROM Measures (degrees). Mean±standard deviation displayed. *Difference between pre-season and in-season scores (p≤0.01).
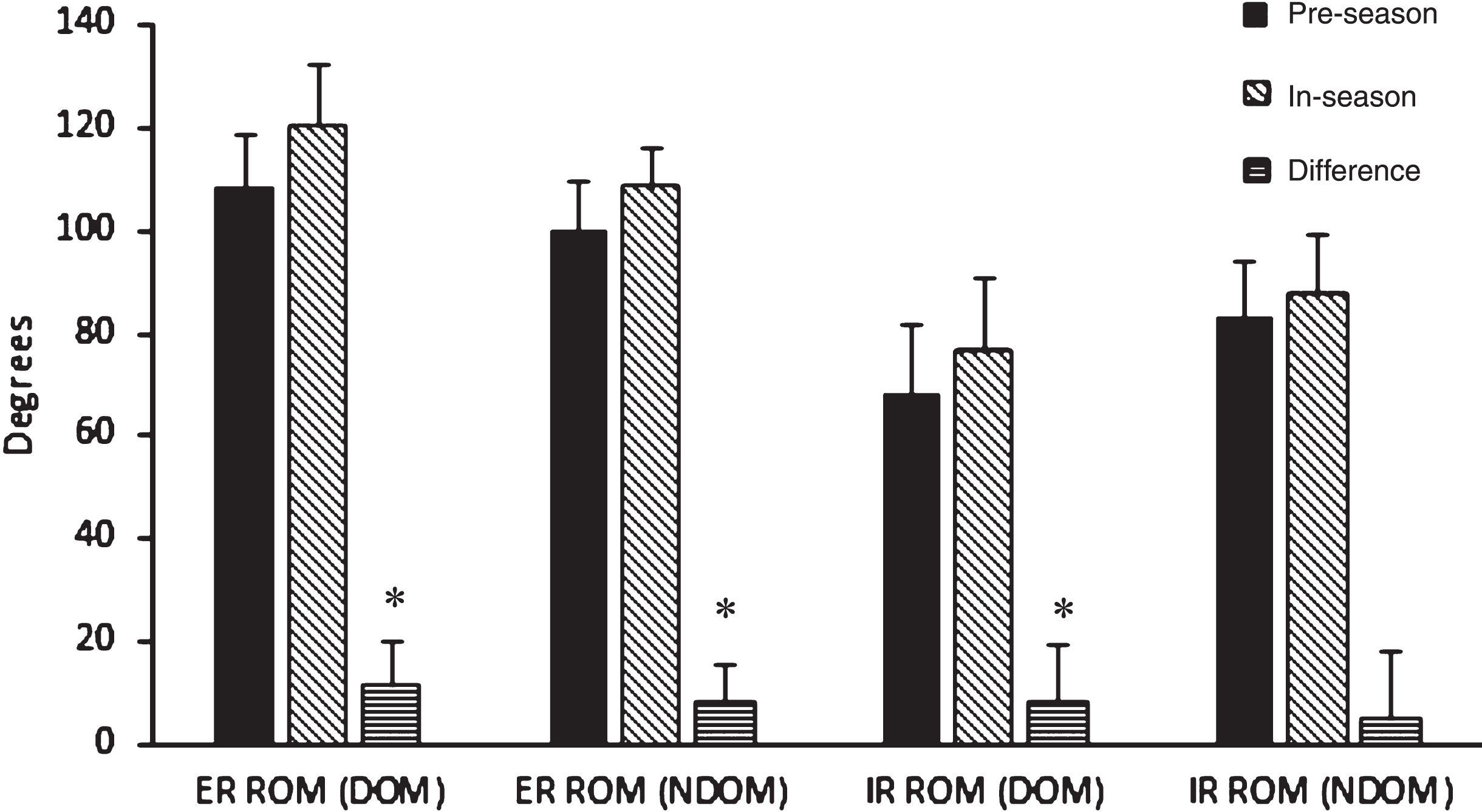
Pre and In-season Player Glenohumeral Joint IR and ER ROM Measures (degrees). Mean±standard deviation displayed. * Difference between pre-season and in-season scores (p≤0.01).
Over the course of the study, there was a significant (p≤0.01) increase across the group for both dominant and non-dominant Total Arc ROM between pre and in-season measures (Fig. 2), largely as a result of significant (p≤0.01) increases in player ER ROM (Fig. 3)
In-season measures for Total Arc ROM across the sample were comparable with a mean of 198°±16.9° in the dominant shoulder and 197°±10.3° in the non-dominant shoulder. On average, this represented an overall increase of 20°±11.8° of dominant Total Arc ROM, and 14°±14.7° of non- dominant Total Arc ROM, in the repeated measures cohort of eighteen first-class county cricketers during the study period.
In regards to shoulder strength scores (Table 3), at the time of in-season strength measurement, overall group ER MVIC dominant and non-dominant values and PER:IR DOM strength ratios were significantly lower that at pre-season (mean loss of 16–18±21N / 0.2±0.25 ER MVIC NBW per arm, p≤0.05). In the studied sample, Slow-Bowlers were the only group that tended to maintain a balanced 1 : 1 ER:IR MVIC DOM strength ratio across the shoulder between pre and in-season measures. Changes across the group for CET and JAMAR® measures were non-significant.
In regard to prospective development of shoulder pain within the studied group, at in-season follow-up, 27.8% of the sample (n = 5, 2 FB’s, 3 BAT), presented with self-reported ‘Arm Trouble’ during OHT activities that was not preventing them from playing on the KJOC questionnaires. Those with in-season upper-limb pain (n = 5) tended to exhibit differences in mean pre-season side-to-side Total Arc ROM scores (17.3°±6.2°), whilst side-to-side Total Arc ROM scores were comparable in the unaffected group (n = 13). Similarly, those in the in-season ‘playing, but with arm trouble’ group had greater ER non-dominant ROM compared to the ‘no arm trouble group’, whilst players who developed in-season ‘arm trouble’ had a tendency towards lower Pre-season ER:IR DOM strength ratios (≤0.71±0.13 v 0.93±0.21), than those who did not.
The current cohort of professional cricket players exhibited side-to-side shoulder ROM profiles consistent with other overhead throwing athletes of similar ages who had been assessed with similar methodologies in previous studies [3, 43]. For example, all players studied (regardless of playing position) exhibited a mean Total Arc ROM of approximately 180° bilaterally, comprising of decreased internal and increased external glenohumeral joint rotation of the dominant shoulder in comparison to the non-dominant shoulder. Similar findings have been previously reported in repeated measures observational studies in college baseball [24], whilst the studied cohort of professional cricketers also evidenced significant in-season increases in dominant and non-dominant Total Arc ROM and ER ROM during the course of an athletic season.
It has been postulated that these overhead throwing-specific ROM patterns develop as a consequence of short-term and chronically induced sport-specific soft-tissue/capsuloligamentous and osseous humeral retroversion adaptations [9, 39–44]. Previous studies investigating the pathomechanics of overhead throwing athletes have implicated glenohumeral joint posterior-inferior capsular contracture caused by recurrent microtrauma induced by high volume and intensity repetitive eccentric throwing loads, as the primary mechanism in development of the ‘disabled throwing shoulder’, whilst comparison of side-to-side GIRD measurements has been accepted as an appropriate clinical marker of this phenomenon [7–9, 51]. In the current study, between one-quarter of the original sample (n = 34), and a third of the repeated measures sample (n = 18) had a clinically defined GIRD of≥20 degree side-to-side IR difference [40, 51], at baseline testing. In contrast, once ROM deficits were classified in line with Wilk’s original “total motion concept”, 50% of the repeated measures sample (n = 9/18), and 56% of the initial sample (n = 19/34) exhibited clinical Total Arc ROM deficits between their dominant and non-dominant throwing arms [8]. Nevertheless, the efficacy of traditional GIRD and TAM measurements as pre-season prognostic clinical markers in relation to the onset of shoulder pain/injury in the studied cohort may be questionable on account that only 5 out of 18 professional Cricket players studied (27.7%) identified themselves as prospectively developing in-season ‘Arm Trouble’ by the time of the second study measurement, whilst mean GIRD Dominant-non-dominant ROM differences in this group were below previously suggested GIRD clinical thresholds (-18.1°±8.7°). On this evidence, it may more prudent for clinician’s to consider using combinations of upper-limb musculoskeletal profiling screening measures in tandem (i.e. ROM & Strength), whilst making allowances for typical individual and sport-specific variations that may occur in healthy throwers when setting GIRD and TAM cut-off definitions [24, 51].
In analysis of the strength data of the studied sample, whilst players did not produce absolute MVIC scores of the magnitude of top flight Major league professional baseballers [25], they did exhibit mean IR Dominant unilateral ER:IR muscle ratio patterns comparable to age-matched asymptomatic non-athletic controls [45], and minor league baseballers [19]. In fact, even though playing position specific numbers were limited in the current study, it appears that professional first-class county cricket players may exhibit their own unique position-specific strength profiles, with fast bowlers generally maintaining balanced mean ER:IR ratio patterns (0.85±0.17), whilst specialist batsmen (0.74±0.14), and slow bowlers (1.12±0.25) tended to be either largely IR or ER strength dominant respectively. It is conceivable that this may occur as a direct consequence of specific musculoskeletal adaptations in response to variations in the specific technical demands and intentions of front-on fast bowling and side-on slow-bowling techniques [20, 52], a-kin to documented specific positional variations in glenohumeral joint ROM and strength between position players and pitchers in baseball [8, 43]. Nonetheless, knowledge of these potential variations in professional first-class county cricket player position-specific upper-limb musculoskeletal profiles may serve to provide a basis upon which to base future individualised conditioning and clinical/therapeutic decision making and programing for particular players [48].
Finally, in regard to the analysis of players perceptions of their athletic upper-limb KJOC function and pain during the study, 29% of players classified themselves as ‘Playing, but with arm trouble’ at some stage during season, whilst pre-season Dominant vs non-dominant Total Arc ROM differences of≥-17.3±6.2, and ER:IR DOM strength ratios≤0.71±0.13 were evident in the small group of players (n = 5) that prospectively developed in-season shoulder issues. Overall, less than one-fifth of players surveyed (n = 6/34) rated their upper-limb function as ‘100% ’ on the KJOC score at any stage during season. These findings are consistent with previous work that has also identified a similar prevalence of shoulder issues amongst professional first-class county cricket players (23%) during the course of a previous competitive season [2], highlighting the fact that professional cricketers tend to continue to participate regardless of shoulder pain without missing matches, meaning the impact of such overuse shoulder problems may be overlooked when employing ‘time-loss’ injury surveillance classifications [1, 49].
Potential limitations of the current study are that the dependent variable used to establish a temporal link between clinical GIRD, Total Arc ROM, and strength measures with incidence of injury was based solely on player self-reported injury/pain KJOC questionnaire scores. Future studies may seek to triangulate this data with official club medical records to more accurately verify the incidence and impact of player shoulder injury/pain during the competitive season. Similarly, measures of shoulder rotator strength were gained using MVIC HHD measures, even though shoulder external rotators have been found to function primarily in an eccentric manner during the deceleration phase of the throwing motion [6–9, 40]. On this basis, it may have been more clinically relevant to measure the strength of these muscles in an eccentric manner as per previous methods [20]. However, considering its ease of use, practicality, portability, cost, size, and moderate-to-good reliability and validity when compared with isokinetic devices, HHD strength testing remains a justifiable and practical field-based muscle strength assessment method in this context [53].
In summary, the current cohort of professional cricket players exhibited significant increases in Total Arc ROM and decreases in dominant ER:IR strength ratios across a competitive Cricket season. It appears that professional cricket players may exhibit their own unique strength and ROM profiles, dependent upon playing position, that are inherently different to other overhead throwing athletes, given the subtle sports-specific differences and demands of professional Cricket. This is the first study to have attempted to monitor serial changes in seasonal upper-limb ROM and strength, whilst providing temporal classifications of player’s current upper-limb functional/injury status at time of ROM and strength testing in professional cricket players. It is hoped that these findings may be useful in informing future injury prevention, screening, load monitoring, and player ‘In-season’ conditioning strategies, in a bid to help reduce the impact and prevalence of shoulder injury/pain in future cohorts of professional cricket players.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The authors would like to thank the ECB and the first class county cricket clubs of Leicestershire, Derbyshire, and Middlesex, as well as former ECB physiotherapist Mark Young, county physiotherapists Rob Leather, James Pipe, Pete Waxman, and Dylan Morrissey at QMUL for their assistance with the study.