
Abstract
BACKGROUND:
Thoracic spine pain and dysfunction (TSPD) has received less attention in the literature compared to the lumbar and cervical spine, which has created challenges for differential diagnosis in the region.
AIMS:
The study purpose was to describe the clinical activity and outcomes of TSPD patients attending a clinical specialist physiotherapist (CSP)-led orthopaedic and rheumatology triage service, known as the ‘Musculoskeletal Assessment Clinic’ (MAC).
METHODS:
The Clinical Audit department of St Vincent’s University Hospital, Dublin, approved this study. A retrospective service evaluation was carried out of patients who attended the MAC with TSPD between August 2012 and October 2015. Data were analysed using descriptive statistics with SPSS version 20.
RESULTS:
Of the n = 5,143 new patients referred to the MAC over a period of 37 months, 88 of these (2%) (mean age 36.66, years sd = 16.61), were referred primarily for TSPD. Sixty nine percent (n = 61) of patients were categorized as non-specific thoracic spine pain (NSTSP) and 18% (n = 16) structural. Seventy-six investigations were requested for 59% (n = 52) of patients and plain radiograph was the most frequently requested (40.8%, n = 31). Eighty percent (n = 70) of patients were independently managed by CSPs, with 16% (n = 14) of patients being referred for a surgical or medical consultant opinion.
CONCLUSION:
The majority (80%) of the patients were independently managed by the CSPs. Presentations of TSPD to a physiotherapy-led triage service in a secondary care setting attributable to underlying serious pathologies appears to be rare. Replication of this study in other healthcare institutions would be useful for corroborating our findings.
Introduction
Spinal pain has been described as a significant clinical, social and economic problem worldwide [1], however it has been suggested that the thoracic region is an area that has not been afforded the same clinical and epidemiological focus as the lumbar and cervical spine [2, 3].
Epidemiological data suggests that thoracic spine pain is much less prevalent than lumbar spine pain. Briggs et al. [4] in a systematic review of 33 studies reported a one-month prevalence of 1.4–34.8% for thoracic pain across children, adolescents and adults [4]. A similar systematic review of low back pain (LBP) documented a one-month prevalence of 24.0–49.5% [5]. Data from service evaluations and audits of physiotherapist-led orthopaedic triage clinics also appear to reflect this. Low back pain has been reported to account for 35% of patients referred to a physiotherapist-led orthopaedic triage clinic over a 7 month period compared to 3% for thoracic spine pain [6].
Thoracic spine pain and/or dysfunction (TSPD) may result as a symptom of disorders of the musculoskeletal system of varying aetiologies including idiopathic, inflammatory, degenerative, and structural conditions [7–9]. Spinal pain and/or dysfunction may also occur as a result of specific conditions such as osteoporotic fractures, infection and malignancy [3, 10–12].
Thoracic spine pain and/or dysfunction may also occur due to the complex interaction between the innervations of visceral tissue and thoracic spinal structures as they converge on shared levels of the spinal cord. An increase in afferent activity from visceral tissue due to pathology can lead to referred pain in the thoracic region [13, 14]. Thoracic spine pain and/or dysfunction may also arise from other non-musculoskeletal sources such as the viscera i.e. the gastrointestinal, cardiopulmonary and renal systems [15], which may create difficulties with the differential diagnosis of a symptomatic thoracic spine [3]. Conditions such as acute pancreatitis, duodenal ulcers and visceral trauma can potentially refer pain to the thoracic region [16]. Thus the challenge for clinicians is to out rule sinister conditions when considering the thoracic region [17].
However in many cases of TSPD, there may be no single explicit and identifiable anatomical musculoskeletal source of pain and/or dysfunction [4, 18–20]. Similar to non-specific LBP (NSLBP), benign thoracic musculoskeletal spinal pain could be potentially afforded the title ‘non-specific thoracic spine pain’ (NSTSP).
Over a 42-year period a study found that in a total of 2,750 primary bone neoplasms, 4.6% of cases related to the spine, with the majority of these (37.8%) located in the thoracic spine [21]. A systematic review of evidence for malignant metastases reported approximately 70% of all bone metastases are located in the spine with 60–80% of those relating to the thoracic region [22]. The notion of TSPD as a symptom presenting in more sinister conditions has led it to become a clinical entity, along with others, known as ‘Red Flags’ [3, 23].
Red flags are symptoms found in a patient history that may relate to serious pathology, other examples being age (greater than 50 years), previous history of cancer and prolonged steroid use [10, 24]. However the diagnostic value of TSPD as a red flag has been challenged. Downie et al. (2013) reported the likelihood ratios for thoracic pain and scoliosis as indicators for malignancy and spinal fracture are close to zero, +1.0/–1.0 and +1.6/–0.9 respectively [11]. However, TSPD is still presented as a red flag among some international guidelines on spinal pain that influence investigation selection for sinister pathology [25].
The Western Australian Diagnostic Imaging Pathways Guideline advises if any red flag, including thoracic pain, is present in LBP then a plain radiograph is indicated [26]. However, it has been suggested that unnecessary spinal imaging is a societal and clinical concern with adverse consequences for both policy makers and patients alike [27].
Physiotherapy-led triage services have been in existence for many years within hospital based orthopaedic and rheumatologic clinics in order to help reduce costs by triaging patients who do not necessarily need consultant intervention [6, 29]. The prevalence, diagnoses and outcomes of patients with TSPD seen in physiotherapy-led musculoskeletal triage services are not known.
The purpose of the study was to carry out a retrospective service evaluation of TSPD patients assessed in a physiotherapy-led orthopaedic and rheumatology triage service, known as the Musculoskeletal Assessment Clinic (MAC), based in a university-affiliated secondary care hospital setting between August 2012 and October 2015. The primary aims of this service evaluation were to: Estimate the prevalence of TSPD in patients attending the service Describe the diagnostic categories of patients presenting with TSPD with the specific aim of identifying the number of patients diagnosed TSPD attributable to a medically ‘serious’ pathology.
Secondary aims were to: Describe the demographics of patients presenting with TSPD Describe the number and types of investigations requested by CSPs, and report on reasons for their selection. Describe the care pathways along which patients with TSPD were managed.
Methods
Study design
A retrospective service evaluation was carried out of all TSPD patients attending the MAC over a 39 month period from August 2012 to October 2015.
The MAC is a musculoskeletal assessment triage clinic lead by two CSPs, operating in the Bone and Joint Unit of St Vincent’s University Hospital (SVUH), a University-affiliated secondary care hospital. This unit includes six orthopaedic and six rheumatology consultants and accepts referrals from General Practitioners (GPs) and other hospital consultants. Consultants screen all referrals and select which patients are to be assessed in their consultant-led clinics or the MAC.
The primary functions of the MAC are to provide a diagnosis and determine an appropriate care pathway for the management of patients with musculoskeletal disorders. Patients are managed along one or a combination of the following pathways: referral for physiotherapy, referral onto the orthopaedic or rheumatology team, referral onto another medical or surgical specialty (e.g. pain medicine), request for further investigations and/or MAC review or discharge back to GP care.
The two CSPs in the current study had 22 and 18 years of clinical experience each, of which 5 and 8 years were in the role of CSP respectively. Both clinicians had completed a relevant postgraduate master’s degree prior to the beginning of the evaluation and one of the CSPs had completed a PhD.
Between August 2012 and October 2015, a total of 5,143 new patients were assessed by the CSPs. For the purposes of this study, TSPD was defined as pain or dysfunction (musculoskeletal or non-musculoskeletal in origin) confined to the “region of the thoracic spine, between the boundaries of T1-12 and across the posterior aspect of the trunk” [7]. Patients whose primary referral was not for TSPD were excluded from the service evaluation.
Procedure
The study was approved by the Clinical Audit department of SVUH. Data were extracted from the electronic clinical databases, maintained daily by the two CSPs as part of routine clinical practice, by one researcher (CS) not affiliated with SVUH. Any patient identified from the database with a clinical diagnosis of TSPD was included in the service evaluation. If there was uncertainty regarding a patients’ diagnosis or management, the patients’ healthcare record was accessed in order to obtain further relevant information. Demographic (gender, age) and clinical (diagnosis, investigations requested, MAC outcome) data were extracted for each patient. Patients’ medical records were searched to establish the outcomes of patients referred on for medical or surgical consultations. All data were subsequently amalgamated into a single dataset using SPSS (version 20). Descriptive statistics were calculated for all variables.
Results
Demographics
Of the 5,143 new patients assessed, 88 patients were identified as presenting with TSPD, representing 1.7% of the total. Of the 88 patients, 65.9% (n = 58) were female. The mean age of the patients was 36.7 years (range = 16–80 years).
Diagnosis
The clinical hypotheses of the CSPs were organised into the eight main categories with associated sub-categories taken from an amended version of an algorithm used in a previous study for thoracic pain [3]. (Table 1). The majority of TSPD patients were categorized as having NSTSP (69%, n = 61). For NSTSP, the subcategory of ‘mechanical thoracic pain’ was the most frequently diagnosed by CSPs at 51% (n = 46). At the time of the audit, 4 of the patients with a clinical hypothesis of NSTSP were currently awaiting confirmation of diagnosis post-investigation.
Diagnoses of TSPD patients according to Categories and sub-categories of TSPD referred to the MAC between August 2012 and July 2015. (N = 88)
Diagnoses of TSPD patients according to Categories and sub-categories of TSPD referred to the MAC between August 2012 and July 2015. (N = 88)
*4 patients with a clinical hypothesis of mechanical thoracic pain awaiting investigation to confirm initial CSP diagnosis. **n = 6 complained of pain ***n = 4 complained of pain.
The second most common category was structural (18%, n = 16), comprising the subcategories of scoliosis at 14% (n = 12) and Scheuermann’s Disease (5%, n = 4). Of note, half of the patients diagnosed with scoliosis did not present with any pain (n = 6). 4% patients (n = 3) were given a diagnosis of axial spine spondyloarthropathy with the remainder of the cohort’s diagnoses including fractures (5%) and discogenic pain (3%) categories.
The majority of TSPD patients (59%, n = 52) who attended the MAC had one or more investigations(s) ordered by CSPs. In total 76 investigations were ordered, with plain radiograph being the most frequently requested (31%, n = 31) followed by MRI (25%, n = 19) (Table 2).
The investigations ordered by CSPs for patients with TSPD? (N = 76 investigations)
The investigations ordered by CSPs for patients with TSPD? (N = 76 investigations)
Sixty percent of patients (n = 31) had 1 investigation while 19% (n = 19) had two and one patient had 4 investigations (see Fig. 1). Of the 52 patients who had an investigation, plain radiograph in isolation was the most common test (31%, n = 16), followed by MRI in isolation at 23.1% (n = 12) and radiograph in combination with blood tests at 15.4% (n = 8) (Table 3).
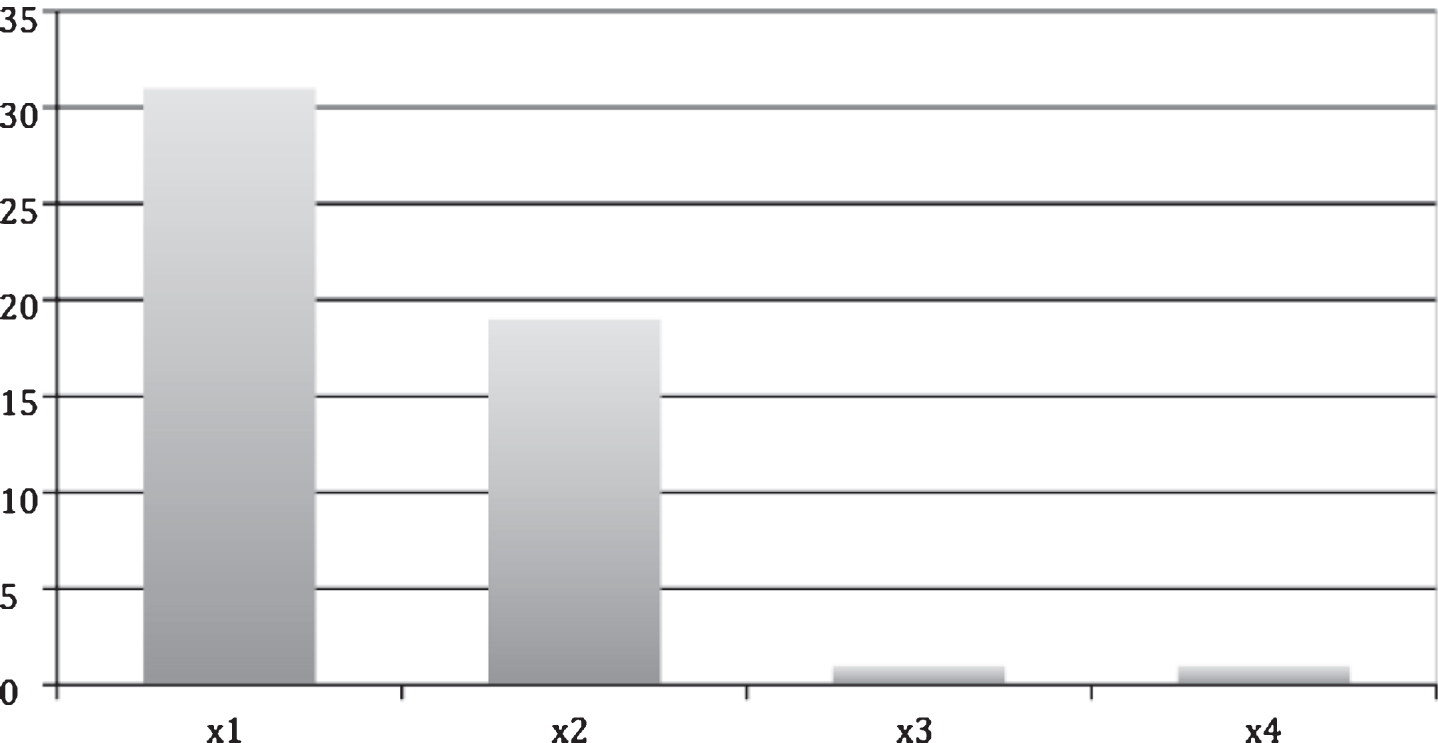
Number of investigations per patient within the MAC (no of patients who had investigations, n = 52; total no of investigations ordered, n = 76). x1 = one investigation, x2 = two investigations etc.
Number and types of investigations ordered per patient with TSPD. (N = 52 patients had an investigation)
XR = plain radiograph, MRI = Magnetic resonance imaging, CT = Computerized tomography, DEXA = Dual energy X-ray absorptiometry.
Fifty-one percent of patients (n = 31) categorized as having NSTSP had an investigation, whereas the proportion was much higher in the structural category with 75% of patients (n = 12) having an investigation.
A total of 10 different indicators were identified for a CSP ordering an investigation (Table 4). The most common reason was to ‘characterise or quantify structural deformity’ for 26.9% (n = 14/52) of patients. The second most frequent reason was a ‘routine’ check by CSPs, (25%, n = 3/52) for either assessing degenerative change or inflammatory markers.
Reasons identified for investigations ordered by CSPs (52 patients had an investigation*)
Reasons identified for investigations ordered by CSPs (52 patients had an investigation*)
*33 patients had one reason identified for their investigation with 19 having more than one reason.
The presence of ‘red flags’ was the reason for investigation in 9.6% patients (n = 5/52). Four different ‘red flags’ were described with ‘night pain’ and ‘age’ reported in each of 3 patients. Four ‘inflammatory signs’ were documented in 8/52 patients (13.5%), with ‘morning stiffness lasting more than an hour’ and ‘secondary multi-site symptoms’ both present in 3 patients each (Table 4). 12% of patients (n = 6/52) had a change in clinical diagnosis following a requested investigation.
The vast majority of patients (79.5%, n = 70) with TSPD were independently managed by the CSPs and did not require onward referral to consultant-led care, with 53% (n = 47) of the patients discharged following advice and 26% (n = 23) patients discharged to physiotherapy (Fig. 2). 88.5% of patients (n = 54) categorized with NSTSP were discharged with no further management from the MAC. All patients diagnosed with a spondyloarthropathy (n = 3) were referred to consultant-led rheumatology clinics.
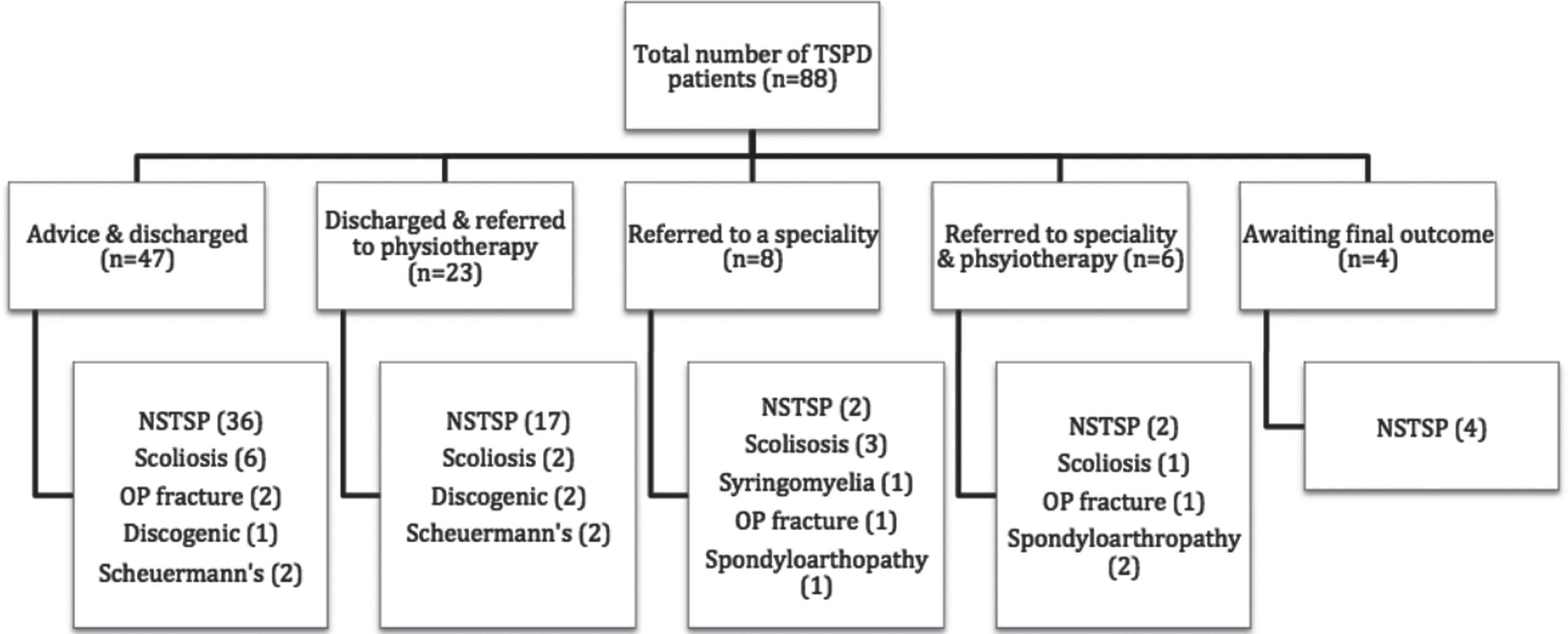
Care pathways for patients with TSPD referred to the MAC and type of clinical diagnosis (N = 88). NSTSP (non-specific thoracic spine pain); OP (osteoporotic).
Sixteen percent (n = 14) of the initial TSPD cohort were referred to specialist consultant care, with 43% also receiving a simultaneous referral to physiotherapy. In relation to the patients referred to specialist consultant care, 43% (n = 6) were referred to orthopaedics. In five of these six cases this was for a surgical opinion (n = 4 scoliosis, n = 1 syringomyelia). Subsequently, these five patients were referred outside SVUH to another hospital for a further specialist surgical opinion, thus their final outcome could not be determined. One of these patients, diagnosed with syringomyelia, was also referred to a neurosurgery department of another hospital for a surgical opinion (Fig. 3).
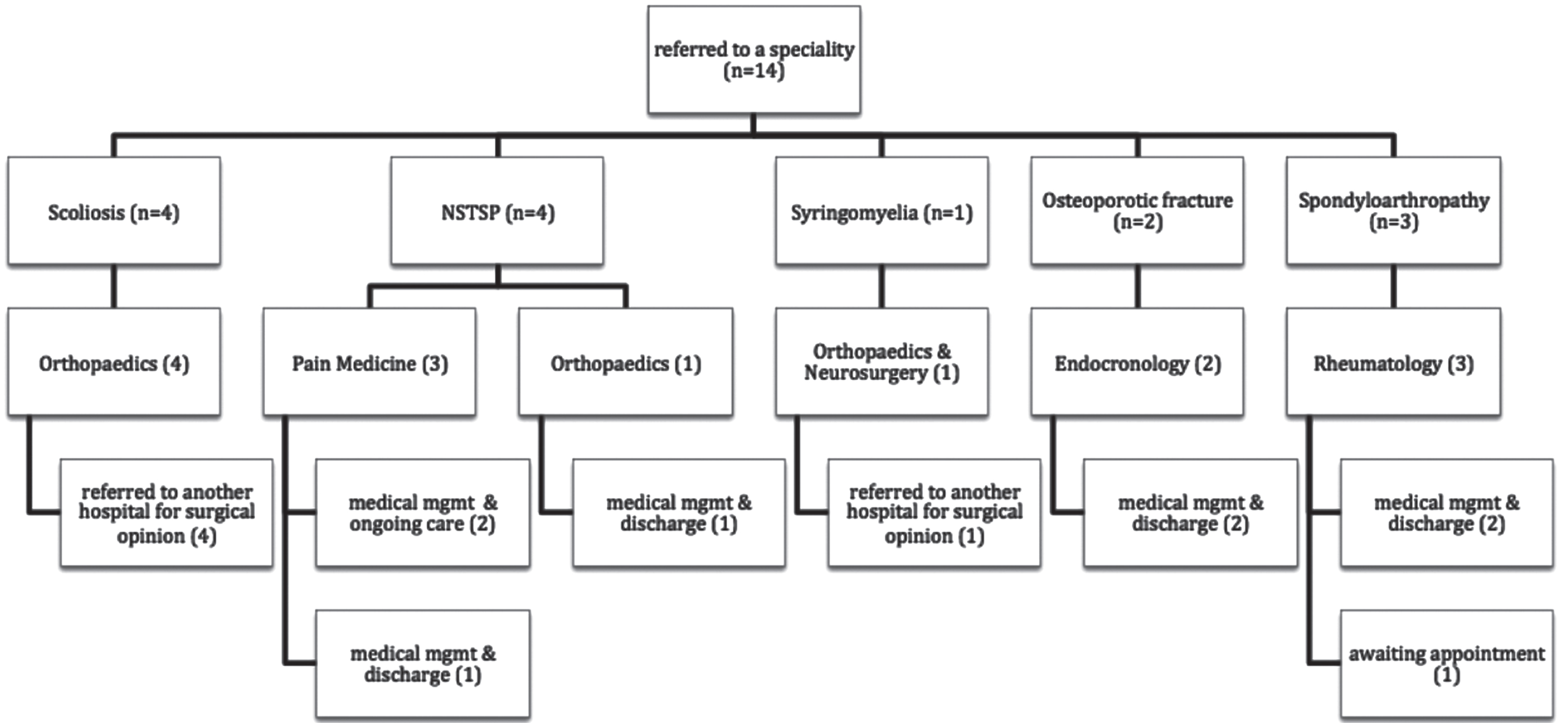
Care pathways for patients with TSPD referred to specialist consultant care according to diagnostic category. (N = 14) NSTSP = non-specific thoracic spine pain, mgmt = management.
Six patients referred to consultant care received medical management and were subsequently discharged from specialist care. One patient at the time of the audit was awaiting an appointment for a rheumatology consultation and the rest of the outcomes are detailed on the care pathway flow chart (Fig. 3).
At the time this study was completed, four out of the total 88 patients were awaiting an investigation requested by a CSP (Fig. 2) therefore their final outcome was unknown.
This service evaluation is the first to focus specifically on patients referred with TSPD to a musculoskeletal triage clinic. Our evaluation found that TSPD accounted for 1.7% of patients seen in a physiotherapy-led musculoskeletal triage clinic. O’Farrell et al. (2014) [6], in a similar study reported that ‘thoracic pain’ accounted for 3% of patients over a 7 month period suggesting that primary presentations of TSPD in physiotherapy-led triage clinics may be extremely low compared to other regional musculoskeletal disorders.
The majority (69.3%) of TSPD patients in the current study were categorized as presenting with NSTSP. Another Irish study investigating LBP in an orthopaedic triage clinic found that over a 27-month period, NSLBP accounted for 72% of 2,146 patients presenting with LBP [30]. In 90–95% of LBP cases, a single anatomical cause of pain cannot be specially determined thus a non-specific label is applied [31]. Therefore, it is possible that benign musculoskeletal spine symptoms classified as ‘non-specific pain’ may be as prevalent in thoracic spine as in lumbar spine.
Osteoporotic fractures described as a ‘sinister pathology’ in relation to LBP [10, 11], is the only ‘sinister’ condition reported in this study accounting for 4.5% of TSPD patients, with no cases of neoplastic, infective or visceral conditions reported. Curley et al. (2004) in a service evaluation in a similar triage clinic reported that 3% of LBP patients presented with a ‘serious pathology’, including myeloma and tumours [30].
It has been suggested in relation to LBP that when the presence of thoracic spine pain is clustered with other red flags it may provide a more robust indication of malignancy [11, 17]. This service evaluation identified that five patients presented with TSPD in addition to other coexisting red flag(s), however none subsequently presented with a sinister pathology following investigation. To the authors knowledge, there are currently no identified systematic reviews or international consensus on the screening of the thoracic spine specifically.
Overall 76 investigations were requested over 37 months for TSPD in the current study corresponding to 0.86 investigations per patient, which is higher than the rate (0.6) previously documented for the MAC in a previous study (n = 714) which reported on all musculoskeletal patients referrals over a 7-month period [6]. The higher rate reported in the current study may indicate that TSPD is more readily investigated however this requires further investigation. Future research may investigate the clinical reasoning processes of CSPs regarding screening for red flags in relation to the thoracic spine and decision pathways for further investigation.
If thoracic and lumbar ‘non-specific’ musculoskeletal spine pain is regarded as benign [18, 31], then it could be argued that the requesting of investigations could be more selective, as it may not alter treatment and unnecessary investigations may hinder patient recovery [32]. Furthermore, what is considered as a ‘routine’ investigation for example in relation to x-ray (accounting for 25% of patients in this study) may need to be challenged in relation to current evidence i.e. if plain radiographs are not advised for NSLBP [25], it is possible this should be mirrored for NSTSP and requires further consideration.
The findings of this service evaluation of a physiotherapist-led triage clinic in an Irish hospital have shown that the majority (80 %) of TSPD patients were independently managed by two CSPs. Wood et al. (2015) in a retrospective study, over a 2-year period, reported that 92% of 2,651 spinal patients were managed by physiotherapists in a triage clinic in the United Kingdom [33] and Blackburn et al. (2009) reported that 71% were of back pain patients were independently managed by physiotherapists in an Australian triage clinic [34]. Evidence has shown that experienced physiotherapists leading orthopaedic and/or rheumatology triage services can independently manage the majority of patients thereby helping to downstream costs, waiting times, and patient outcomes [36, 37].
Limitations and future recommendations
The current findings should be considered alongside certain limitations. The diagnosis, investigations and outcomes of patients in one physiotherapy-led MAC may not be representative of others either nationally or internationally. Although the current study was performed over a period longer than most comparable triage studies, the sample size may be considered low. As some patients were referred beyond SVUH, the study was not able to fully investigate the outcome of some patients.
Further research could investigate the incidence screening procedures and management of of TSPD patients within a variety of different clinic settings such as a primary care centre e.g. when assessed by a first contact practitioner physiotherapist or GP.
Future research and empirical evidence may help to develop a consensus on the most appropriate screening tests and procedures for patients with TSPD.
Conclusion
The findings of this service evaluation indicate that non-specific TSPD may be as common within the thoracic region and has been described for NSLBP in the lumbar area, and integration of treatment models, such as the biopsychosocial model [18], employed for LBP could be considered for NSTSP. Although TSPD has been historically aligned to sinister conditions, this assumption requires further investigation.
Contribution of the paper
The majority (69%) of patients in this service evaluation were categorized with non-specific thoracic spine pain. This is comparable to previously reported rates for non-specific low back pain (72%) and challenges the view that thoracic spine pain may be indicative of sinister patholoty. Future research could focus on thoracic spine pain and dysfunction in a primary care setting. There appears to be an innate caution amongst clinicians regarding thoracic pain and its history as being indicative of a ‘Red Flag’ symptom. This study found that 0.86 investigations were requested per patient, which is higher than that reported in other comparable studies (0.6). This study reported the second most frequent reason for requesting an investigation was as a ‘routine check’. Imaging and testing help clinicians rule in or out certain pathologies but investigation usage may need to be tempered in line with current evidence. This study demonstrated that the majority of patients (79.5%) were independently managed by two clinical specialist physiotherapists which is in line with other evaluations/audits of physiotherapist-led triage services for spinal and musculoskeletal pain.
Conflict of interest
There are no conflicts of interest.
Ethical approval
St Vincent’s University Hospital, Dublin has provided ethical approval for this study (Audit No 1414).