
Abstract
PURPOSE:
Advanced Practice Physiotherapy (APP) in paediatric orthopaedics is an effective adjunct to traditional consultant-led clinics, improving patient access to outpatient services, and reducing both waiting lists and times. However there has been no published economic evaluation of a paediatric orthopaedic APP service. This study performs a cost analysis, utilising a cost minimisation approach, comparing an APP Clinic in Paediatric Orthopaedics with usual care, from a health care perspective.
METHODS:
Data on all patients managed by the APP clinic for one calendar year were collected and outcomes and associated costs were calculated, including follow-up care. These costs were compared to the estimated costs of the usual care pathway, an Orthopaedic Consultant Elective Clinic (OCEC) and incremental savings per patient was calculated.
RESULTS:
A total of 534 patients attended the APP clinic for initial assessment during the calendar year 2017. The unit cost of a new appintment with the APP clinic is € 32.46 in comparison with € 56.98 for a new appointment in the OCEC. Our results demonstrate an incremental per patient saving of € 24.51 in favour of the APP clinic. Sensitivity analysis demonstrates that the cost savings obtained hold consistent in all cases, varying from € 23.13 to € 29.67 per patient in favour of the APP clinic pathway. This represents a cost saving of 43% for the APP Pathway over that of usual care.
CONCLUSION(S):
This is the first study to perform an economic analysis of the APP role in paediatric orthopaedics and demonstrates that an APP clinic for non-complex paediatric orthopaedic patients is substantially less costly than usual care.
Introduction
Musculoskeletal disorders are one of the most common reasons for a child or adolescent to attend their primary care physician or emergency units, accounting for between 4% and 18% of presentations annually [1–6]. Limited research exists that quantifies the cost of paediatric musculoskeletal disorders to health service providers and society, but available evidence implies the burden has been underestimated to date and is significant. A large proportion of these patients are referred by their general practitioners (GPs) for consultant opinion [3], however paediatric orthopedics as a specialty service is largely considered to be under-resourced and under-staffed worldwide [7–9]. This lack of investment has resulted in growing waiting lists for elective referrals, access issues and excessive wait-times for patients internationally [8, 10–12].
One effective solution to the outpatient waiting list problem has been the introduction of physiotherapists with extended scope and advanced practice duties, both within existing hospital services and as part of community interface teams [13–17]. These roles have developed internationally within public health systems over three decades, primarily in musculoskeletal medicine, and are now well-established service models in the UK, Australia, Ireland and Canada as well as Nordic countries, with proven reductions in patient wait-times [13–16, 18–21]. Advanced Practice Physiotherapists (APPs) are specialist physiotherapists who perform some tasks traditionally performed by doctors including patient assessment, referral for X-Ray/MRI, diagnosis and treatment, joint injection, removal of casts and K-wires and listing for surgery in some instances [20]. The APPs act as first-contact practitioners both in primary and tertiary care, with the goal of improving access for patients to specialist opinion, reducing waiting lists and providing intermediate care for patients who do not necessarily require a consultant review [21–25].
Recent evidence supports the APP role in paediatric orthopaedics as an effective adjunct to traditional consultant-led clinics, providing a means of improving patient access to outpatient services and reducing both waiting lists and waiting times for patients [26, 27]. A recent study demonstrated that over a 3 year period, 77% of patients presenting to a specialist APP clinic in paediatric orthopaedics were managed without consultant intervention. Mean wait-time for initial appointment was reduced from 101.92 weeks to 15.45 weeks for those patients managed autonomously by the APP clinic [26]. These outcomes are corroborated by similar findings in other studies [27, 28].
Despite many studies evaluating APP practice in adult and paediatric populations [16, 30], a number of literature reviews have highlighted the lack of high quality economic evaluations of APP practice. One within-trial cost analysis reported significantly lower direct costs to the hospital for the APP group, due mainly to lower salaries in this group compared to doctors, and significantly fewer requests for X-rays by the APP [31]. Some studies have shown small cost savings from APP clinics with fewer GP follow-up appointments and drug recommendations by APPs but increased numbers of physiotherapy appointments attended [32–34]. All of these studies have been conducted on adult populations. As yet the economic implications for this new model of service delivery remain unclear and there has been no published economic evaluation of an APP service specific to the paediatric population, from a health care perspective. This study seeks to perform a cost analysis, utilising a cost minimisation approach, comparing an APP Clinic in Paediatric Orthopaedics with usual care considered here as the Orthopaedic Consultant Elective Clinic (OCEC).
Methods
This economic evaluation was conducted following the guidelines by Drummond et al. [35] and Guidelines for the Economic Evaluation of Health Technologies [36]. The perspective adopted is that of the publicly-funded health and social care system [36]. Data were collected for the calendar year 2017, as part of a prospective longitudinal study evaluating an APP-led clinic. The analysis employed in this study utilises a cost-minimisation approach. When using this method to perform an economic analysis, care pathways are compared in terms of their costs only, if their outcomes have been proven or are expected to be similar [35, 36]. Our group has previously published research showing patient outcomes comparable with those from consultant -led clinics [26] and good to excellent (k = 0.46–1.0.) diagnostic agreement rates when compared with orthopaedic consultants’ diagnoses [37].
The APP clinic in paediatric orthopaedics
Two specialist physiotherapists lead the APP clinic, which runs concurrently and is co-located with the OCEC. All elective orthopaedic referrals to the hospital are reviewed by the consultant team, assigned a priority (routine/urgent) and allocated to the APP clinic by the consultants. Inclusion criteria for the APP clinic are routine/ non-complex patients with the following referral diagnoses: normal variants, curly toes, trigger thumbs, popliteal cysts, gait disorders, lower limb pain of mechanical origin, low back pain of mechanical origin and scoliosis screening. Exclusion criteria for assignment of referral to the APP clinic are lower limb conditions with specific diagnoses such as Perthes Disease, requests for specific surgical opinion and referrals suggestive of neuromuscular disorders, or infective, inflammatory or malignant disease. The OCEC sees all urgent patients and routine patients that do not meet the APP clinic inclusion criteria. As the APP service has been in operation since January 2011, this has resulted in two entirely separate streams of patients attending the different clinics, APP and OCEC, respectively.
The APP performs an assessment and diagnosis which allows formulation of an autonomous management plan. Any request for consultant opinion is at the APP’s discretion. All requests for investigation (X-Ray/ MRI/ Blood Tests) are initiated by the APP. Greater detail on the development and management of the service is available in a previous publication [26].
Patient clinical pathways
Within the APP service, once assessed by the physiotherapist, the patient folows one of four clinical care pathway outcomes as detailed in Fig. 1 and Table 2; discharge (D/C) back to GP+/–local therapy if necessary; review at APP clinic; review at orthopaedic clinic; refer to other specialist service e.g. paediatrics; neurology; rheumatology. Within this model, any patient booked for follow-on care in the OCEC is allocated a review appointment slot as per hospital policy. Patients who attended follow-on care with other specialities in the hospital are allocated new consultant appointments as they are new to that service. These clinical care pathways were devised from the outset of the APP service in conjunction with the relevant stakeholders i.e. hospital management; the hospital consultant group, allied health service managers and the APPs.
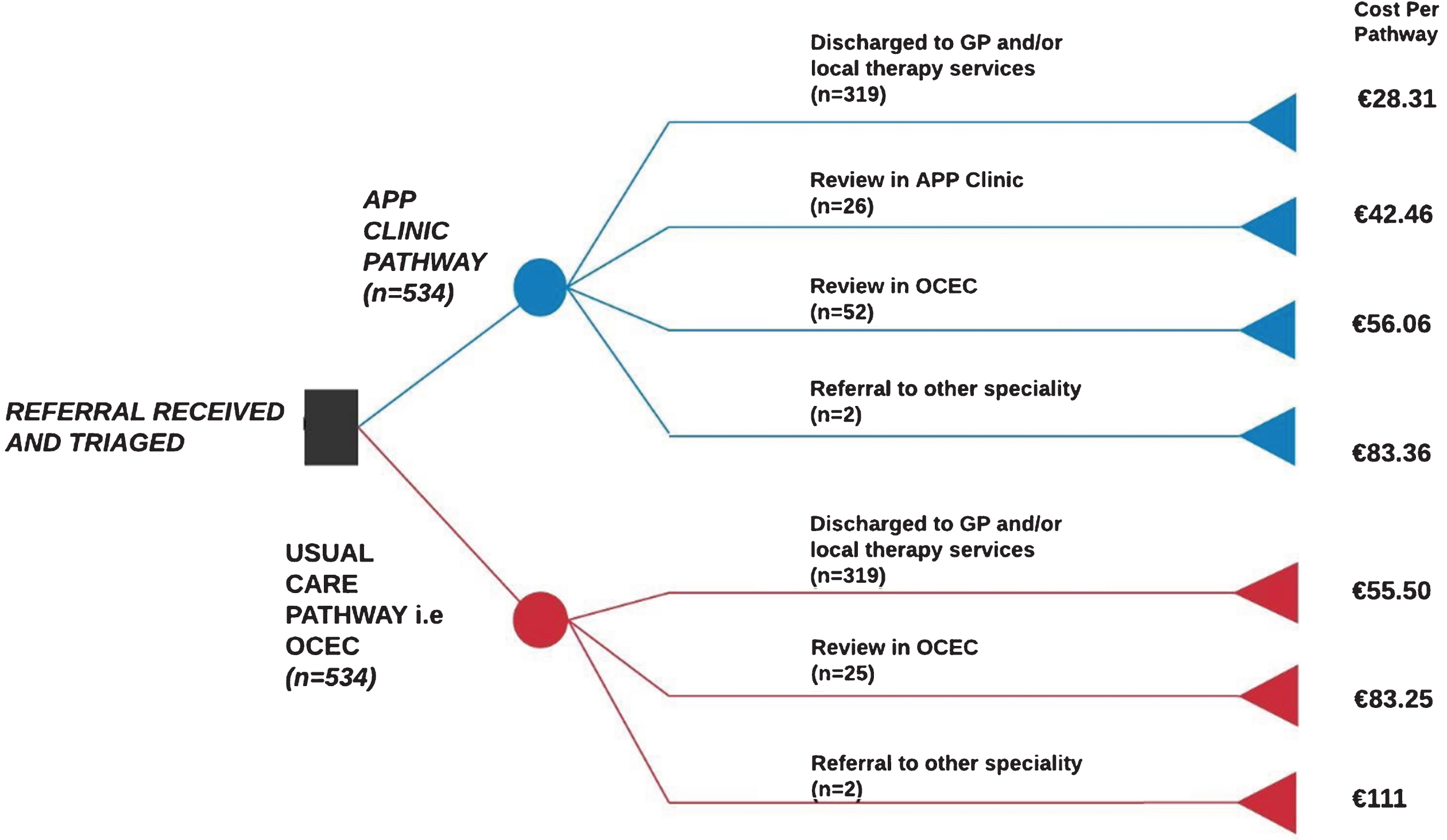
Decision Tree representing Clinical Care Pathways: APP Clinic Vs Usual Care including costings for each arm. APP Clinic pathway represents actual pathway and treatment of patient in 2017. Usual Care pathway represents hypothesis of pathway for same patient cohort in absence of APP service. The final column respresents the individual cost of each pathway arm.
All new and review appointments for the APP clinic are given 30 and 15 minute slots respectively, as per hospital policy. New and review appointments with an OCEC are given similar time frames [38], with time allocated for review by the non-consultant hospital doctor (NCHD) and nursing support. While there is some variation in actual time spent at appointments, this was not recorded for each individual patient and analysis was conducted based on recommended safe outpatient appointment time-frames [39].
An electronic database of the APP pathway was established to prospectively record the following: demographic information, date of referral, date of first appointment offered, referring diagnosis, diagnosis after assessment in the APP clinic and clinical care pathway outcomes. Data cleaning was performed and patient health care records were reviewed to obtain missing data. All data recorded were cross-referenced with the hospital Patient Administration System (PAS) to ensure accuracy.
As the APP clinic and OCEC clinic manage two entirely different patient cohorts, it was not possible to obtain actual costs and outcomes of the OCEC for a matched patient population. Therefore usual care was calculated as the predicted costs and outcomes of patients if the APP clinic did not exist; i.e. attendance only at an OCEC. Data for the usual care pathway were predicted from the APP data. Initial predictions for all usual care patient pathways were matched to those of the APP clinic and revised following a review of all cases by a member of the consultant team to ensure agreement. The possible predicted pathway outcomes were: Discharge (D/C) back to GP with or without local therapy; review at orthopaedic clinic; or refer to other specialist service. Descriptive analysis of patient characteristics was performed using SPSS 24.0.
Costs
Costs were calculated for care of all new patients seen in the APP clinic and their follow-up care for one calendar year. Costs were calculated to reflect the health service perspective when providing a new service [36]. From the patient perspective, there is no difference between the 2 clinic pathways proposed in terms of indirect and out-of pocket costs incurred. Costs were not discounted as the study was conducted over a 12-month period. All costings are provided in local currency (Euro) for the cost year 2017.
Capital and overhead costs
The APP clinic is co-located and runs strictly in conjunction with the Consultant clinic. Capital outlay for provision of equipment including an examination plinth, desk, 3 chairs and a desktop computer were annuitized to calculate the equivalent annual value (Appendix A) [40]. The APP clinic receives the same administrative support as all orthopaedic clinics, such as appointment management and digital dictation. Overhead costs to the hospital such as heating, lighting, IT services, provision of waiting area space are included as per guidelines [36] as 25% of annual salary.
Direct costs
The APP clinic is managed with a single specialist physiotherapist and no auxiliary nursing staff in attendance. In comparison, a patient receiving usual care via the OCEC will interact with a minimum of one staff nurse, one NCHD and one consultant as per safe outpatient appointment guidelines [39]. Personnel wages were calculated based on the midpoint of the relevant staffs’ published, consolidated pay scales [41, 42]. As there are currently different salary scales for consultants, an unweighted average of the midpoint of each of the scales was used to estimate consultant wages.
Sensitivity analysis
This base-case analysis calculated costs for patients that attended for either a new or review appointment within one calendar year. It is common practice in paediatric orthopaedics to review patients at a more distant point in the future e.g. 1-2 years, to evaluate the effect of growth on a patient’s symptoms. The base-case analysis included only patients who were advised to return for review during the same calendar year. A sensitivity analysis was conducted to test the robustness of the original analysis and included costs for all patients advised to return for a review APP appointment or OCEC appointment at any future date, and varying patient attendance rates from 10% to 100%. A further sensitivity analysis was performed costing the pathways assuming that all staff were on the lowest relevant pay scale rating and similarly on the highest relevant pay scale rating.
Results
A total of 534 patients attended the APP clinic for initial assessment during the calendar year 2017. Of those who presented, 52% were female and the mean age was 7.75 years (Table 1).
Characteristics of patients attending physiotherapy orthopaedic triage clinic
Characteristics of patients attending physiotherapy orthopaedic triage clinic
GP = General Practitioner.
All patients in this study entered the APP care pathway which resulted in one of 4 outcomes which are reported in Table 2 and delineated in Fig. 1 with the cost per appointment for each outcome. Following initial assessment, 76.9% of patients attending the APP clinic were managed independently without a consultant intervention deemed necessary. The cost of a new appointment with the APP was € 28.31. There were no additional appointment costs for all patients who were discharged to the care of their GP.
Clinical outcome following initial assessment at APP clinic
*Some patients attended for more than 1 review appointment in the year 2017 ie. 40 patients attended for a total of 52 consultant review appointments. ¶ APP clinic can refer directly to other specialities within the hospital such as paediatrics, neurology, rheumatology, plastic surgery and endocrine.
Those who attended a follow-on appointment generated additional costs which are reflected in Fig. 1. Those who attended for a review appointment at the APP clinic generated a further cost of € 14.15 per patient. A total of 17.6% of patients seen were booked for review appointment in the OCEC (€ 27.75 per additional appointment) and 5.6% were referred to another speciality (€ 55.50 per appointment). Not all patients booked for review attended their follow-up appointment, and a small number of patients in the orthopaedic review category attended for more than one review appointment within 2017.
To calculate the cost of the usual care pathway, we predicted costs based on actual data collected from the APP pathway. All patients were costed for a new appointment in usual care (€ 55.50 per appointment). The APP pathway data identified 40 patients who attended the OCEC for a total of 52 review appointments. In the predicted usual care pathway, these 40 patients would have had their initial assessment in the OCEC and only 12 would have required review. In addition, of the 26 patient seen for review at the APP clinic, only 13 were designated as requiring review at the OCEC, as identified by a member of the consultant orthopaedic team. Therefore the total number of appointments is 25. The orthopaedic team similarly agreed that those patients referred to another speciality were appropriate, therefore those that attended another speciality in 2017 were costed as for the APP pathway (€ 55.50 per appointment). These are all imputed costs for the usual care pathway, based on actual data collected from the APP pathway.
Table 3 demonstrates the cost per appointment in each pathway, including both new and review appointments, taking into account salary, overhead and time allocated per appointment. The average cost for a new and review elective patient to be seen in the APP clinic is just under half of the cost for the same patient to be seen in a consultant clinic: € 28.31 compared to € 55.50. A similar differential can be seen for review appointments.
Cost per appointment based on salary, overhead and time allocated to patient whether new/ review
PRSI = Pay Related Social Insurance; APP = Advanced Practice Physiotherapist (APP); NCHD = Non-Consultant Hospital Doctor (NCHD) (Source: (42); Overhead costs defined as per local guidelines(36).
Table 4 shows the results of the cost analysis, which takes into account both new and review appointments that took place over one calendar year, and also Capital outlay costs for the APP clinic. This gives a figure of total unit cost of a new appointment with the APP clinic is € 32.46 in comparison with € 56.98 for a new appointment in the OCEC. When total costs for each pathway were considered by number of contacts, we found an incremental cost saving to the service provider of € 13093.38 in favour of the APP clinic care pathway, or € 24.51 per patient
Total cost of appointments for one calendar year: APP clinic vs Usual Care
*APP appointments do not exist in Usual Care Pathway i.e. N/A. ¶ Only 25 patients identified as needing “Review” appointment with orthopaedic consultant in Usual Care pathway due to receiving initial appointment with consultant in this pathway Capital Outlay Cost as previously described in methods and delineated in Appendix A.
Table 5 shows the results of the sensitivity analyses, which were conducted in the first instance to include all those patients advised to return at any future date for a review appointment, with varying patient attendance rates, and in the second instance, evaluating the cost when all staff were costed for their lowest and the highest pay scale rating. The results demonstrate that the cost savings obtained hold consistent in all cases, varying from € 23.13 to € 29.67 per patient in favour of the APP clinic pathway.
Sensitivity analysis
The objective of this study was to perform a cost analysis of an APP clinic in paediatric orthopaedics compared to usual care, utilising a cost-minimisation approach. This is the first study to perform such an analysis in paediatric orthopaedics and it reports an incremental saving of € 13,093.38 for one calendar year in favour of the APP clinic. This represents a cost saving of 43% for the APP Pathway over that of usual care. Our results demonstrate that an APP clinic for non-complex paediatric orthopaedic patients is less costly than usual care.
The base-case analysis calculated costs for all new and review patient attendances that occurred in one calendar year (2017) reporting an incremental per patient cost of € 24.51. The results of the sensitivity analysis were similar to the base-case with savings between € 23.13 and € 26.41 per patient. A further sensitivity analysis demonstrated that the base-case results held true, despite varying salary scale, with savings of between € 24.15 and € 29.67 reported. We are cognizant that not all clinics will have similar staffing requirements to our own and may not have an NCHD in attendance. However, we elected not to perform a sensitivity analysis based on the consultant alone seeing the patient in the OCEC, as these results would have overwhelmingly reported in favour of the APP pathway, given the marked differential in salaries.
Proposed as a cost-effective means of delivering high quality services to patients who do not necessarily need surgery, APP clinics have been introduced and widely adopted internationally [13, 43]. A variety of approaches have been used in the literature to evaluate their economic value, both in APP adult orthopaedic triage and other disciplines. Comans et al. [44] utilised a cost-utility approach to demonstrate an incremental cost effectiveness ratio (ICER) of AUD $1691 per QALY for their adult APP Triage program. This was considered to be highly cost-effective when compared to the Australian implicit threshold of AUD $50,000 [45] per additional QALY gained. Cost-analysis studies performed alongside RCTs evaluating APP services have been reported in Accident and Emergency [46] and adult orthopaedic outpatient services [31], with inconsistent results reported. The former showed no savings in direct costs to the health provider and the latter reported the APP clinic as significantly cheaper. Neither study utilised a full cost-effectiveness methodology in terms of demonstrating an Incremental Cost Effectiveness Ratio (ICER).
Our analysis was based on appointment costs within the local healthcare system, taking into consideration appointment time, administration costs, overhead, and capital costs. A previous British study reported an APP paediatric orthopaedic clinic to be cost-effective based on staff wages [28], with no discussion of appointment time, numbers of patients seen, or overheads/ initial outlay capital costs.. Our results of a 43% cost saving compare favourably to a similar study in adults in the UK where savings of 27.3% [47] were reported relative to usual care pathways.
It is a limitation of this study that a Cost-Effectiveness Analysis or a Cost Utility Analysis could not be performed. However, given that the majority of the patients are discharged without the need for intervention, we were unable to identify an appropriate paediatric validated outcome measure to demonstrate an improvement in health outcomes or quality of life [48, 49]. For this reason, our group chose to perform a cost minimisation analysis. This approach assumes the outcomes of patients attending the APP clinic pathway are identical to outcomes for these same patients if they had attended usual care pathway. This method has been used in recently published literature to evaluate the costs of implementing new methods of care within physiotherapy and occupational therapy services [50–54]. This assumption is supported in three ways. Firstly, the majority of the patients screened as suitable to attend the APP clinic pathway are a patient group known as normal variants; conditions that resolve spontaneously with the normal growth and development of the child, and do not require treatment to alter the outcome [55–57]. This patient group constitutes between 25% –50% of the elective referrals to paediatric orthopaedic surgeons, and they are usually discharged after the initial assessment [58–61]. These conditions make up greater than 50% of the patients seen in the APP clinic in this study [26] and previous work by this research group demonstrates that the APP management of these conditions concurs with expert opinion and similar international studies [26–28].
Secondly, it is also reasonable to assume that the APPs made accurate and similar diagnoses to those the patients would have received if they were seen in the usual care pathway. A previous study by the current authors evaluated diagnostic agreement between the APPs and the orthopaedic consultant team at our facility across a broad spectrum of disorders, and found diagnostic agreement rates to be good to excellent based on kappa co-efficient (0.46–1.0.), with a raw percent agreement of 87% [62]. Similarly, previous literature identifies that specialist physiotherapists have near perfect agreement with paediatric orthopaedic consultants in terms of assessing and diagnosing paediatric gait concerns [63]. Finally, in terms of safety, the APP clinic has been in operation for more than 7 years and has managed in excess of 6,000 patients. The service is located in the same tertiary facility as the national centre for paediatic specialities, including oncology, haematology, rheumatology, and genetics, and no adverse outcomes have been identified or reported for any patients who initially presented through an APP paediatric orthopaedic clinic.
A major limitation of this study is the lack of a direct and concurrent comparator service in the facility where the research was conducted. Our centre is a major tertiary paediatric orthopaedic hospital and all elective appointments are for specialist opinion. The APP clinic manages patients deemed routine and consultants manage urgent and surgical patients. In comparing costs between clinics, this is an evaluation of actual costs to attend the APP clinic, versus the predicted costs to the hospital if the patients had been seen in a consultant clinic. It is assumed that the investigative costs, such as x-rays and bloods, would have been similar or lower than in consultant clinics, as APP clinics in other contexts have previously demonstrated [31, 64]. However it is acknowledged that investigative costs may have been different between care pathways and we have not addressed these differences in cost. There is minimal provision of equipment and no provision of medication to patients from the APP clinic, primarily due to the fact that the majority of these patients are diagnosed as normal variants and discharged. Therefore these items were not costed, as the costs were negligible. It is assumed that predicted costs from the usual care pathway would also be negligible for the same patient cohort, but this is an assumption and therefore a limitation. Again while we delineated the patient pathways presented in this study with the consultants and reviewed each patient’s data in tandem with them as a quality assurance mechanism, we cannot be sure that predicted patient pathways in the consultant clinic are accurate.
The activity costed in this study does not take into account or cost those who failed to attend the assessment or review appointments made in the APP clinic in 2017. No published data exist to allow an estimation of attrition rates at consultant clinics in comparison to APP clinics for patients screened as suitable for APP assessment, therefore it is possible that these rates may have differed between the care pathways in terms of overall number of assessments actually provided. The authors assume that the attrition rate would have been the same for the consultant clinic; however this is acknowledged as a limitation of the study.
This study is a single centre study and as such could be viewed as reflecting cost savings for one centre, based on local work practices. However, as the role of APPs is relatively new internationally, and the studied centre is the first to provide it nationally in paediatrics, it was not possible to conduct a multi-centre study. It should be acknowledged that the costs in this study are estimated using data from a public hospital and may not be directly generalizable to other health systems with differing funding models. Dierick et al (65) highlight the difficulty in establishing cost-effectiveness for an intervention as complex as role substitution as “outcomes are related not only to clinical health status, process of care and costs, but also to non-health care outcomes, like accessibility or continuation of care.” Nevertheless, this analysis provides evidence in demonstrating the potential savings that can be achieved in a given setting.
Conclusion
This study demonstrates that significant savings can be made to the health service by national adoption of APP roles in paediatric orthopaedic centres. As compared to a consultant clinic, the APP clinic generates a per patient cost saving of € 24.51, and a pathway saving of 43% inclusive of initial asset costs to set up the service. Further economic evaluation to include a Cost Benefit Analysis of the service is planned.
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
Ethical approval for this study has been granted by the institution Hospital Ethics (Medical Research) Committee. This article does not contain any studies with human participants performed by any of the authors.
Funding
This study forms part of a PhD undertaken at University College Dublin which was partly funded by the National Children’s Research Centre, Dublin.
Footnotes
Appendix A
Asset costs
| Item | Source | Quantity | Total cost | Equivalent annual value | ||
| Plinth | Medstore.ie | 1 | € 1250 | € 146.54 | ||
| Desktop computer with microsoft office | HarveyNorman.ie | 1 | € 828 | € 97.10 | ||
| Desk chair | Medstore.ie | 1 | € 199 | € 23.33 | ||
| Patient chair | Medstore.ie | 2 | € 318 | € 37.28 | ||
| Desk with computer workstation | Bryansryan.ie | 1 | € 155.41 | € 81.22 | ||
| Total | € 322.43 |
Equivalent annual rate calculated as per ACT Consortium Guidance on Economic Evaluation (40) Assuming 10 year warranty/ lifetime on all assets, discount rate 0.03(35).