
Abstract
INTRODUCTION:
The rate of force development (RFD) is increased by high-load isometric resistance training (RT), whereas not by low-load isometric RT. However, it is unknown whether low-load isometric RT with neuromuscular electrical stimulation (NMES) can increase the RFD.
PURPOSE:
The aim of this study was to clarify the short-term effects of low-load isometric RT with NMES on the RFD.
METHOD:
Twenty-four healthy subjects randomly received both low-load RT of the hip abductor muscles with NMES and sham NMES condition. The RFD of the homonymous muscles was assessed at pre- and post-intervention. Time intervals of the RFD were set to 0–50 ms (50RFD), 0–100 ms (100RFD), 0–200 ms (200RFD), and 0–300 ms (300RFD). Two-way repeated measures analysis of variance was used to analyze the effects of time and intervention.
RESULT:
Low-load RT with NMES significantly increased 50 and 100RFD compared to sham NMES condition. On the other hand, 200 and 300RFD were not changed by either condition.
CONCLUSIONS:
The significantly increased RFD might be related to the factors affecting each RFD interval. This finding might have an important clinical implication for developing a mechanism-based effective training.
Keywords
Introduction
The rate of force development (RFD) has been studied as a useful indicator of muscle strength. The RFD is calculated by the change in force over a certain time period (Δforce/Δtime) during an isometric contraction [1–5]. Previous studies reported a positive correlation between the RFD and gait speed and the activities of daily living score [6, 7]. In addition, the RFD has been assessed at different time intervals from the onset of contraction (e.g., 0–50 ms, 0–100 ms, 0–200 ms, etc.) because these intervals reflect different factors [1, 8]. In particular, previous studies reported that the RFD at shorter time intervals reflects factors pertinent to neural drive (e.g., spinal excitability) [1, 8], whereas the RFD at longer time intervals reflects more diverse factors (e.g., muscle cross-sectional area) [2].
Many studies have reported methods to increase the RFD. Some studies have shown that the RFD was significantly increased by high-load isometric resistance training [1, 10]. Conversely, other studies showed that the RFD was not significantly increased by low-load isometric resistance training [6, 12]. In addition, previous mechanism-related studies suggested that the enhancement of neural drive by resistance training contributes to an increase of the RFD [1, 13].
Spinal excitability is enhanced by neuromuscular electrical stimulation (NMES) [14, 15]. Although NMES alone does not have a significant effect to increase the RFD [6], we hypothesized that the RFD, especially shorter-interval RFD, representing the state of neural drive, would be increased by low-load isometric resistance training with NMES. In the present study, hip abductor muscles, which stabilize the pelvis in the frontal plane during walking, were chosen as test muscles because they have an important role in both elderly individuals and patients with functional impairment of the hip (e.g., femoral neck fracture and total hip arthroplasty) [16–20]. In addition, a higher RFD in hip abductor muscles increases duration of one leg standing balance, whereas reduces time to walk using tandem gait. [21].
The aim of this study was to clarify the short-term effects of low-load isometric resistance training with NMES on the RFD of hip abductor muscles in healthy adults. If the hypothesis stated above that the RFD, especially shorter-interval RFD, would be increased by low-load isometric resistance training with NMES was valid, this study could have important clinical implications for individuals with difficulty performing high-load resistance training such as patients with pain after fracture surgery and knee osteoarthritis [22, 23].
Methods
Subjects
Twenty-four healthy adults (8 females; 26.2 [1.7] years old; mean [SD]) participated in this study. No subject had a history of either neurological or orthopedic disease. They provided informed consent to the experimental procedure, which was approved by the human ethics committee of our hospital. This study was performed in accordance with the Declaration of Helsinki.
Experimental procedure
All subjects took part in two testing sessions on two different days. The experimental procedure is shown in Fig. 1. The subjects randomly received an intervention of low-load isometric resistance training combined with NMES (training with NMES) in one trial and the same training combined with sham NMES (training with sham NMES) in the second trial. To avoid carry-over effects of the interventions, the interval between the trials was set to a minimum of 1 week (maximum of 2 weeks) according to a previous study [24]. All subjects were placed in a side-lying position with their non-dominant side upward on a treatment table. The hip and knee of the non-dominant limb were at 10° flexion with neutral rotation and at full extension, respectively. The hip and knee of the dominant limb were in slight flexion for comfort and stability [5]. First, the optimal stimulus points of the non-dominant gluteus medius for NMES were explored while observing muscle contraction according to a previous study [25]. And, the point was defined as the point of stimulation at which a barely perceivable muscle contraction was present at the lowest stimulus intensity [26]. Then, two electrodes were placed in the positions over the non-dominant gluteus medius (Fig. 2). Before the intervention, the RFD of the hip abductor muscles was measured (shown in detail below) as the pre-intervention assessment. After the intervention ended and confirming each subject does not have muscle fatigue, the RFD of the hip abductor muscles was measured again as the post-intervention assessment.

Flowchart of experimental procedure in this study.

Typical electrode positions to stimulate gluteus medius.
The subjects were placed in the same position while fitting the band attached a pull sensor type handheld dynamometer (HHD) (Mobie; SAKAI Medicine, Tokyo, Japan) used in the pre-intervention assessment. To conduct the isometric resistance training of hip abductor muscles, the non-elastic band made of 100% polyester was used. The subjects were instructed to perform isometric resistance training for a total of 10 times with NMES or sham NMES. The isometric resistance training was consisted of muscle contractions of 3-4 s duration at a rate of 4 times/min, which is based on a previous study [8]. The load of resistance training was set to approximately 30% of their maximal voluntary contraction (MVC) measured at pre-intervention assessment in each experiment day, which was used as low-load training in a previous study [12, 27–30]. In addition, during intervention, visual feedback of force was provided to the subjects on a computer screen placed at eye level.
A portable surface neuromuscular stimulator was used for NMES (Delta Zero; Nihon MEDIX, Tokyo, Japan). The proximal and distal electrodes (5×5 cm, SR5050) were placed on the motor point of the non-dominant gluteus medius at the muscle belly. An asymmetrical biphasic square pulse was used for the stimulus waveform. The pulse width and stimulus frequency were set to 1 ms and 100 Hz, respectively [14, 15]. In the training with NMES condition, stimulus intensity was set to a sub-motor threshold in the non-dominant gluteus medius. Motor threshold was defined as the minimum stimulation intensity needed to evoke a visible twitch. In the training with sham NMES condition, stimulus intensity was set to zero. To ensure that the subjects were unaware they were receiving NMES or sham NMES, they were informed that the stimulus intensity in both conditions was set to a low level that would be imperceptible [31]. In addition, visible twitch was induced in both the NMES and sham NMES condition. Then, the stimulus intensity was gradually decreased to the predetermined value.
Measurement of the RFD
The RFD of the hip abductor muscles was measured using the HHD according to a previous study that indicated high intra- and inter-rater reliability [5]. Briefly, the setup for measurement is shown in Fig. 3. The RFD was measured by using a pull sensor type HHD with the band which was used to remove the assessor bias [32, 33]. The subjects were instructed to contract their hip abductor muscles isometrically as fast and forcefully as possible. In practice sessions, the subjects performed 3 submaximal voluntary contractions for familiarization purposes. After practice, they were asked to maximally contract 3 times for 5 s [28, 29]. Rest time between the trials was set to 60 s. Visual feedback of force was provided to the subjects on a computer screen placed at eye level. The HHD signals were sampled at 1,000 Hz using an analog-to-digital converter (USB-6229; National Instruments, Austin, TX, USA). LabVIEW software (National Instruments, Austin, TX, USA) was used to provide the start signal, log forces, and give visual feedback of force.
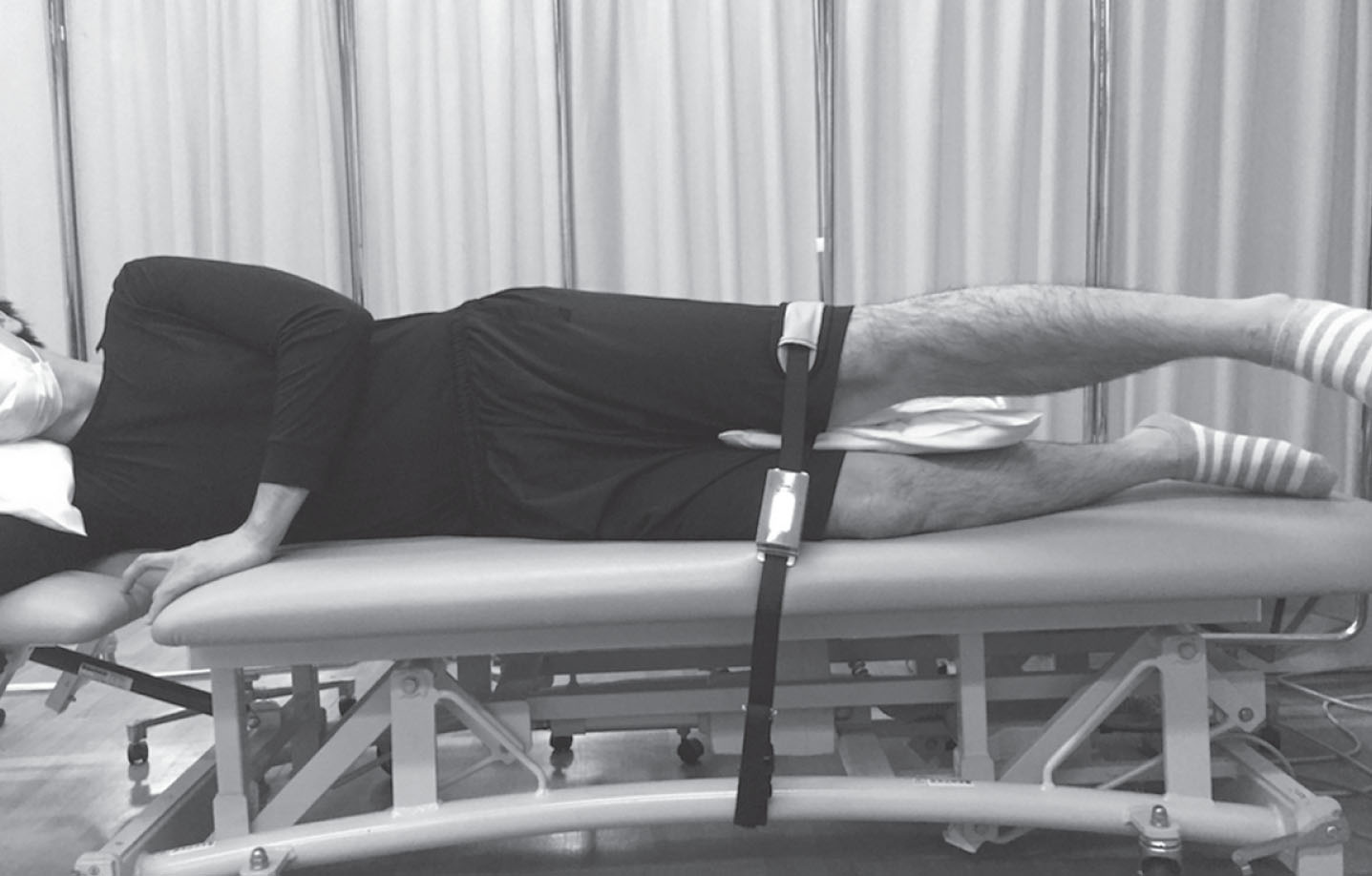
The setup for RFD assessment and low-load resistance training of the hip abductor muscles.
The RFD was derived as the slope of the force-time curve (Δforce/Δtime). Time intervals relative to the onset of contraction were set to 0–50 (50RFD), 0–100 (100RFD), 0–200 (200RFD), and 0–300 (300RFD) ms according to previous studies [1, 34]. Torque onset was calculated as the point above 2% of the MVC for each trial, which is a widely-used criterion for determination [4, 5]. All RFD values were divided by the body weight of each subject. The highest value of the 3 repetitions was used for statistical analysis. To examine the differences of the pre-intervention RFD values between the intervention conditions, a paired t-test was used in each interval. Two-way repeated measure analysis of variance (ANOVA) was used to analyze the effects of time (pre- and post-intervention) and intervention condition (training with NMES and sham NMES). Statistical significance was set at P < 0.05. And, effect sizes were calculated using partial eta squared. Based on a previous study [35], values of 0.01, 0.06 and above 0.14 were considered as small, medium and large, respectively. Moreover, the minimal detectable change at the 90% confidence level (MDC90) was calculated from standard error of measurement×1.65×the square root of 2.
Results
The differences in the pre-intervention RFD value between training with NMES and with sham NMES condition are shown in Table 1. There were no significant differences in the RFD at baseline.
The difference in the pre-intervention rate of force development between training with neuromuscular electrical stimulation (NMES) and with sham NMES condition
The difference in the pre-intervention rate of force development between training with neuromuscular electrical stimulation (NMES) and with sham NMES condition
The mean 50, 100, 200, and 300RFD values at pre- and post-intervention are shown in Fig. 4. And, the summary of two-way repeated measure ANOVA on time and condition is shown in Table 2. The results revealed no significant main effect of time or condition in all intervals. But, there was significant interaction between time and condition in 50 and 100RFD, whereas no significant interaction in 200 and 300RFD. These results represent that 50 and 100RFD values were significantly increased by training with NMES compared to training with sham NMES, whereas 200 and 300RFD values were not changed by either intervention.
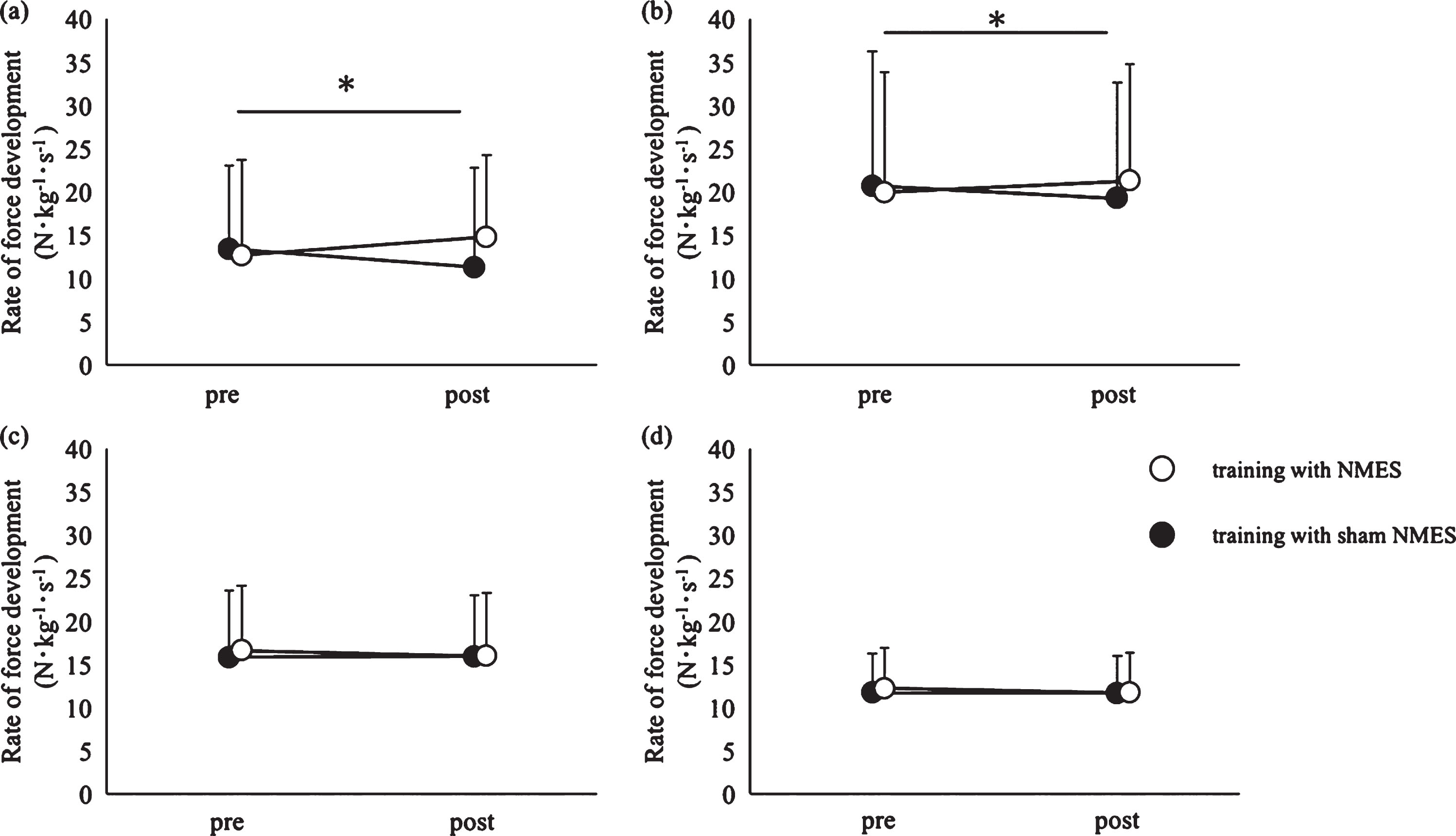
Comparison of the pre- vs. post-intervention on the rate of force development (RFD) across the intervention groups: low-load resistance training with neuromuscular electrical stimulation (training with NMES) (open circles), low-load resistance training with sham NMES (training with sham NMES) (filled circles). Time interval from contraction onset divided into (a) 0–50 ms (50RFD), (b) 0–100 ms (100RFD), (c) 0–200 ms (200RFD), (d) 0–300 ms (300RFD). The bars indicate standard deviation. An asterisk indicates a significant difference (p < 0.05).
Summary of two-way repeated measure ANOVA on time and condition
SS, sum of square; df, degree of freedom; MS, mean of square.
The aim of this study was to investigate the short-term effects of low-load isometric resistance training with NMES on the RFD of hip abductor muscles in healthy adults. The results showed that 50 and 100RFD were increased by training with NMES compared to training with sham NMES. The RFD values in the later time intervals were not changed by either intervention. According to the criterion of a previous study [35], effect size of interaction between time and condition in 50 and 100RFD was large (0.22 and 0.17, respectively), whereas that in 200 and 300RFD was small (0.03 and 0.04, respectively).
The effects of low-load resistance training with NMES on the shorter-interval RFD might be comparable to the high-load resistance training used in previous studies. In this study, 50 and 100RFD were increased by low-load resistance training with NMES (25 and 16%, respectively). Aagaard et al. (2002) reported that RFDs were increased 17–26% by high-load resistance training for young healthy adults [1]. In addition, Suetta et al. (2004) also showed that RFDs were increased 26–45% by high-load resistance training for patients after unilateral hip-replacement who did not feel pain [6]. Although it is not fully clear why only 50 and 100RFD were significantly increased by this combined therapy, one of the factors might be the characteristics of the RFD. Regarding RFD in the shorter time interval, a previous study using surface electromyography suggested that an increase in neural drive contributes to an increase in the RFD [1]. A previous study on spinal excitability, which is a key factor in neural drive, supports this suggestion. Collins (2007) demonstrated that the H-reflex, which is used as an indicator of spinal excitability, is greater when NMES depolarizing sensory axons is delivered [14]. These results suggest that NMES increases spinal excitability and enhances the effect of low-load resistance training on the RFD in the shorter time interval. Moreover, the NMES parameters (e.g., wider pulse width) used in the present study might also have increased effectiveness. A previous study showed that evoked H-reflex became larger with increasing pulse width of the NMES [15].
This study verified the hypothesis that the RFD of hip abductor muscles may be increased by low-load resistance training with NMES. This finding will help the patients with difficulty performing high-load resistance training because of pain. For example, previous studies reported that there are many patients with pain after fracture surgery and knee osteoarthritis and they can not sufficiently cause the strong muscle contraction [22, 23]. In those patients, it is difficult to implement the high-load resistance training to increase the RFD (e.g., 70–90% of 1 repetition maximum) [1,9,10, 1,9,10], which is positively correlated with gait speed and the activities of daily living score [6, 7].
However, the present study had some limitations. The main limitation of the present study was the small sample size, which decreases the generalizability of the results. In addition, the amount of change by the intervention did not exceed the MDC90 value. The results suggest that the amount of change might not exceed the MDC90 values because there was a certain amount of inter-subject variance of difference in the baseline RFDs. A further study will be needed using a larger sample size. In addition, although the present study clarified the short-term effects of combination therapy, the long-term effects or after effects of combination therapy on the RFD in hip abductor muscles was not tested. For clinical application, a further study will be needed using a larger sample size and to test the long-term effects or after effects of combination therapy.
Conflict of interest
None of the authors has any conflict of interest to disclose.
Footnotes
Acknowledgments
We appreciate Ikuo Motoya and the staff of the Department of Rehabilitation at Kawamura Hospital for their helpful technical assistance.