
Abstract
BACKGROUND:
Recent smartphones are equipped with gyroscopic functions enabling measurement of joint range of motion (ROM). Previous studies have demonstrated that the use of the iPod™ to measure shoulder ROM shows good reliability. However, evidence of concurrent validity of shoulder ROM taken with an iPod™ remains scarce. Thus, the aim of this study was to investigate the concurrent criterion validity of the gyroscopic functions of the iPod™, for the measurement of shoulder joint ROM.
METHODS:
A trained examiner measured shoulder ROM for the movements of flexion, abduction, extension and external rotation. For each movement, four to six trials (repetitions) were performed at different angles, in order to obtain values for the entire available ROM. Measures were simultaneously taken with the iPod™ (5th generation) and a digital inclinometer (gold standard). Validity was estimated using the Intraclass Correlation Coefficient (ICC) and mean differences (MD), as well as 95% limits of agreement (LOA) with Bland-Altman plots.
RESULTS:
ROM data was collected from 28 healthy participants. We found excellent criterion validity for all four movements studied (ICCs = 0.907–0.996). In terms of accuracy, the MD between both instruments for all movements was between –1.9° and 2.0°, except for extension (MD = 3.80°–4.70°).
CONCLUSIONS:
This study provides evidence of validity of the gyroscopic functions of the iPod™ for the measurement of the shoulder ROM in a wide range of amplitudes. The use of an armband to position the instrument can minimize potential measurement errors compared to conventional goniometry. However, future studies should investigate ways to improve accuracy of extension measurements.
Introduction
With an annual prevalence of up to 47% in developed countries worldwide [1, 2], shoulder pain is one of the foremost musculoskeletal problems encountered by rehabilitation professionals [3]. Apart from pain, shoulder pathologies are often accompanied by deficits in joint range of motion (ROM), and ultimately, limitations of activities and disabilities [4].
The measurement of joint ROM is one of the predominant elements of a musculoskeletal assessment - these measurements make it possible to objectively identify deficits, document their evolution over time as well as to evaluate the effectiveness of interventions addressing these deficits [5–8].
Recent technological advances have enabled smartphones, such as iPhone™ and iPod™, with gyroscopic functions, allowing angular measurements. As such, gyroscopic functions are available on all iPod™ (generation 4 and above). These functions combine an accelerometer, a gyrometer and a magnetometer to provide measurements in degrees, expressed in three axes, called “Roll” for left-to-right rotation, “Pitch” for front-to-back rotation and “Yaw “ for rotation on itself. Hence, mobile devices equipped with sophisticated sensors (gyroscope equipped smartphone or iPod™) are becoming widely available and are challenging traditional ROM assessment tools. They are relatively affordable ($200US) and potentially a more accurate tool to measure ROM than an universal goniometer [9]. In fact, an increasing number of professionals use their smartphones in everyday clinical situations such as documenting progress related to patient’s performance and providing home exercise programs [10]. Another advantage of the iPod™ is that it is more convenient to use than the universal goniometer or inclinometer, as it can be directly attached to the patient’s arm, therefore reducing potential positioning errors [11]. This aspect can also help the therapist to note and correct any movement compensations, thus reducing measurement errors originating from the patient. Finally, some applications (ie: GetMyROM) offer the possibility to save and send by email the results of the examination, therefore reducing potential recall bias and potentially save time for clinicians.
It has been shown that smartphone static ROM measurements are to comparable to a robotic arm and an inertial measurement unit (IMU) [12]; their sensors are sufficiently precise to measure biomechanical real-time movements [13]. On the human body, smartphones were already shown to be reliable and/or valid for the measurement of movements of the spine [14, 15], ankle [16, 17], knee [18–24], hip [25], wrist [26] and elbow [27–29]. In regards to shoulder ROM measurements, the reliability of smartphone measurements (obtained via different applications) has also been studied and documented as good to excellent [30, 31] (See appendix 1). Also, some studies evaluated combined movements of the shoulder and found an inter-rater reliability ranging from 0,79 [32] to 0,92 [33] and an intra-rater reliability of 0,92 [33].
Although the reliability of smartphone measurements for the shoulder joint seems to be well established, the concurrent validity of smartphone measurements of shoulder ROM remains scarce because previous studies had some limitations in their methods, related to they fact that not all movements were studied, but most importantly, the gold standard they used was for most studies a universal goniometer –the goniometer has a very high measurement error [11] (See appendix 1). Thus, considering the multiple advantages of the iPod™ mentioned above and the limitations found in the literature, our main objective was to study the concurrent criterion validity of the gyroscopic functions of the iPod™ for the ROM measurement of shoulder flexion (FLEX), abduction (ABD), extension (EXT) and external rotation (ER). The underlying scientific hypothesis was that the concurrent validity of the iPod™ would be confirmed for all shoulder movements, with Intraclass Correlation Coefficients≥0.80 (with the digital inclinometer as the gold standard). Moreover, since the shoulder is the multiaxial articulation of the human body with the highest amplitudes [1, 5], we also aimed to explore the validity of this instrument within multiple articular amplitudes for each movement, as all previous studies only examined its validity at end-range. Yet, ROM limitations may occur at any particular angular movement.
Methods
Design
This is a descriptive, cross-sectional, correlational study comparing shoulder ROM measurements obtained by the iPod™ to those acquired concurrently by a digital inclinometer (gold standard).
Participants
Potential participants were included if they 1) had sufficient shoulder ROM (at least 75% of the normal ROM [34]) for the movements performed in this study, 2) were able to understand and apply the instructions correctly, 3) had no reports of shoulder pain or shoulder pathology in the last six months and 4) were at least 18 years of age.
Recruitment
We conveniently recruited the participants from the student population within the School of Rehabilitation of the Université de Sherbrooke via ads posted in the student lounge and messages on social media. After being screened for inclusion criteria, we obtained participants’ full and written informed consent. At the end of the procedures, the volunteers who participated in the study received an amount of ten dollars ($10) to offset any travel or parking expenses. The project was approved by the Ethics Review Board of the Centre Hospitalier Universitaire de Sherbrooke (Project # 2016-1279).
Instruments
iPod™: This study investigated the validity of the gyroscopic functions of the iPod™ (5th generation) via the Gyroscope application. This generation of iPod™ is equipped with a LIS331DLH accelerometer, a L3G4200D gyrometer, both manufactured by STMicroelectronics [35]. Angles, at starting and end-positions, were acquired through the Gyroscope application - Gyroscope, by Acrossair - was downloaded from the Canadian Apple App store. The Gyroscope application is easy to use and simply displays angles computed by the operating system; we chose this application since it offers better external validity when comparing our results with previously published papers who utilized an application using the gyroscope-based sensors [32, 36–38]. For all measurements, we used the angles provided the by the “pitch”. The pitch represents the front-to-back rotation (up and down movement was our reference axis) and was used because of the positioning of the iPod™ on the participant arm’s. Digital inclinometer: the reference measurements were obtained via an ACU360 Acumar™ digital inclinometer. We chose the digital inclinometer as a gold standard measure for three main reasons: 1) this instrument has a resolution of 1° according to the manufacturer, 2) the inclinometer could be positioned along the surface of the iPod™ as it has a flat surface, which facilitated the concurrent measurements and reduced potential information bias, and 3) it has good psychometric properties, with sufficient reliability and validity in the measurement of shoulder ROM to be considered a reference/criterion measure - See appendix 2. [39, 40].
Data collection procedures
a) Training of the evaluator
In order to minimize errors generated by the therapist, the evaluator, a third year physical therapy student, had previously received entry-level training for shoulder ROM assessment and also underwent a supervised training with an experienced physical therapist (mock sessions) with two participants to further refine positioning of the instruments and practicing with the procedures. The data obtained from these two participants were not used in the analysis.
b) Landmarking
Before positioning the instruments on a participant, the research assistant identified and marked, using a pen and ruler, 1) the axis of the humerus in the sagittal and frontal planes (anterior and posterior), 2) the styloid process of the radius and applied a four cm proximal marker to this structure on the dorsal surface of the forearm (for the measurement of ER). These reference points were used for the subsequent positioning of the cuff (arm-band) containing the iPod™ on the participant’s arm. Landmarks were made on the dominant upper limb of the patient. Landmarking was made by a different person than the evaluator to accelerate the procedures.
c) Positioning of instruments
The arm band containing the iPod™ was fitted on the participants dominant arm on the anterior aspect of the humerus for FLEX, posterior aspect for EXT and lateral aspect for ABD (Fig. 1). For the ER movement, the cuff was positioned on the posterior aspect of the forearm (Fig. 2). At all times, the cuff containing the iPod™ had to remain aligned with the humerus (between the two markers) or styloid process of the radius (for ER). In order to evaluate the concurrent validity, for all measurements, the digital inclinometer was placed on the iPod™ screen, which optimized the positioning maximized alignment of both instruments for concurrent data acquisition, therefore reducing measurement bias between the two instruments. This methodological choice reduced a potential measurement bias, yet it does not truly replicate clinical practice. Also, the two instruments were calibrated simultaneously before taking measurements in order that both instruments showed “0 degrees” when placed on the same flat surface (Fig. 3).
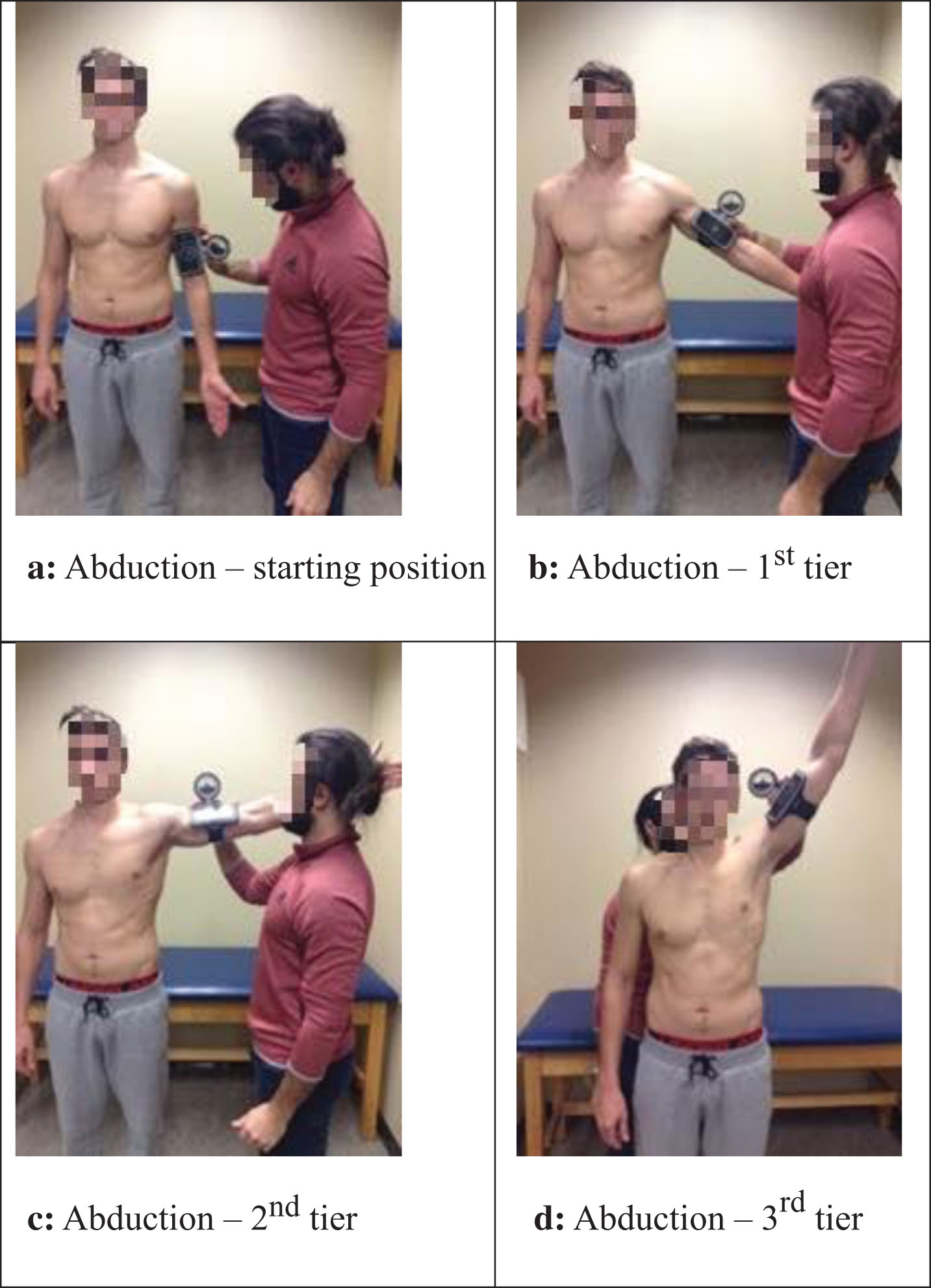
Positioning for the ABDUCTION movement. a: Abduction –starting position. b: Abduction –1st tier. c: Abduction –2nd tier. d: Abduction –3rd tier.

Positioning for the EXTERNAL ROTATION movement. a: External rotation –starting position. b: External rotation –1st half. c: External rotation –2nd half.

Simultaneous calibration of iPod™ and the inclinometer on a flat surface.
For the movement of FLEX and ABD, from a vertical starting position (Fig. 1a) the participant had to perform two consecutive repetitions in three different amplitudes, namely the first tier (0–59°) (Fig. 1b), second tier (60–119°) (Fig. 1c) and third tier of available amplitude (120–180°) (Fig. 1d). For EXT and ER, given the more limited total amplitude available, we requested two repetitions in only two different amplitudes (first half and second half of available ROM (Fig. 2)). Measures were taken in the following order: FLEX, EXT, ABD and ER. The entire measurements were taken by the same evaluator, in the presence of an observer. The observer gave the following verbal indications to the participant.
FLEX: Raise your arm forward, keeping your thumb up all the way, stopping at the requested tier. EXT: Bring your arm back, keeping your thumb forward throughout, the movement stopping at the requested half. ABD: Raise your arm to the side, keeping the palm of your hand forward throughout the movement, stopping at the requested tier. ER: While keeping your elbow on the side of your body and the palm of your hand towards the table, please raise your forearm towards the ceiling, stopping at the requested half.
With the exception of ER, measures were taken while the participant remained standing, with his/her opposite (non-dominant) side on the door frame to limit any compensation. For the ER movement, the patient was side lying on their non-dominant side, while their dominant elbow was on their side (Fig. 2). In order to optimize the positioning of the instruments, once the subject reached the desired amplitude, the evaluator made sure to realign the cuff between the markers before taking the final angle. This was done to optimize alignment and mimic clinical practice, thus limiting potential information bias. For all movements, the observed identified and corrected compensations (if any) and recorded on paper the angles verbally given by the evaluator.
Sample Size
To detect a minimal ICC of 0.80 (1–β= 0.80; α= 0.05), a minimum of 26 participants was required. This sample size was calculated a priori using the “ICC.Sample.Size” of the R software [41].
Statistical analysis
As one trial does not influence the next one, the values obtained for each trial were considered independent from one another. Thus, we had a total of 56 values for each tier of each movement (two trials×28 participants). Using SPSS v24.0 software, ICCs values (using a “two-way mixed model with absolute agreement [ICC [1, 2]]) were calculated for each of the four movements under evaluation for each tier (or half). The quantitative interpretation of the ICCs were: an ICC value of less than 0.50 indicates poor validity; an ICC value in the range of 0.50 to 0.65 indicates moderate to good validity, and an ICC value of greater than 0.65 shows good validity [42]. Also, Bland-Altman graphs were computed to determine the extent of a systematic difference (accuracy) between the measurements taken with the iPod™ and the gold standard (digital inclinometer). Bland-Altman plots values were used to identify the mean difference (MD) between the two instruments (MD and the 95% confidence interval for the limits of agreement). This analysis is a graphical method to compare two measurements techniques where the horizontal lines are drawn at the MD, and at the limits of agreement (LoA), which are defined as the MD plus and minus 1.96 times the standard deviation of the differences. If these limits do not exceed the maximum allowed difference between methods, the two methods are considered to be in agreement and may be used interchangeably.
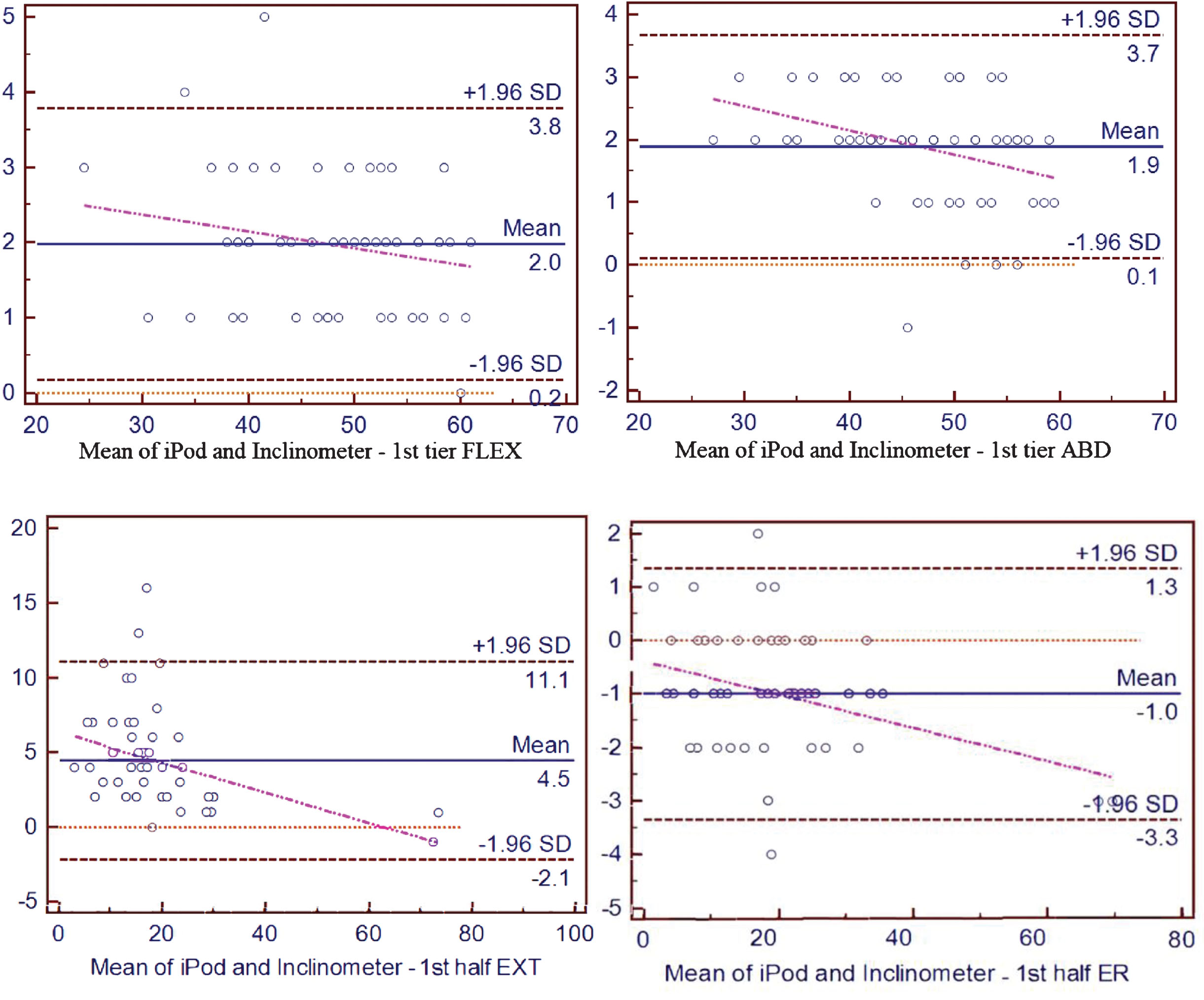
Bland-Altman plots for 1st tier/half of each movement.
We collected data on 28 healthy volunteers (12 men, 16 women). The mean age of our participants was 21.8±1.6 years and the mean body mass index was 23.03±3.64. The complete results of the criterion validity of the measurements are presented in Table 1. When compared to the gold standard used in this study (digital inclinometer), good validity is observed for a) FLEX (ICCs between 0.941 and 0.995 with a measurement difference ranging between –1.9° and 2.0°), b) ABD (ICCs between 0.966 and 0.993 with a MD ranging between –1.2° and 1.9°), c) ER (ICCs between 0.988 and 0.992 with a MD ranging between –1.5° and –1.0°) and d) EXT (ICCs between 0.907 and 0.921 with a MD ranging between 3.8° and 4.5°).
The Bland-Altman plots (Fig. 4) and their values, including the MDs and the 95% limit of agreement (LOA) of the iPod™ measurements compared to the digital inclinometer are also shown in Table 1. Except for the movement of EXT, the MD between the measurements taken with the iPod™ and our gold standard are smaller than the minimal detectable change (MDC).
Criterion validity (ICCs) and Bland-Altman (mean difference and Limits of Agreement) measures comparing the iPod™ versus the digital inclinometer
Criterion validity (ICCs) and Bland-Altman (mean difference and Limits of Agreement) measures comparing the iPod™ versus the digital inclinometer
The purpose of this study was to investigate the concurrent criterion validity of the gyroscopic functions of the iPod™ in the measurement of the shoulder joint. The results demonstrate that the measurements obtained by the gyroscopic functions of the iPod™ have an excellent criterion validity compared to the ones obtained by the gold standard in this study for the measurement of the four main movements of the shoulder.
To our knowledge, only Boissy et al. [37] has compared the shoulder joint ROM values concurrently obtained by the gyroscopic functions of the iPod™, to the ROM values obtained via a digital inclinometer. In our study, we added the movement of EXT to the three movements (FLEX, ABD and ER) they previously measured. Our results seem to have a superior level of agreement than the ones they reported (MDs = 1.3° –9.5°) [37] by taking an optical motion tracking system as their gold standard. Although the optical motion tracking system should be more precise than a digital inclinometer, the fact that we placed the smartphone directly on top of the digital inclinometer (our gold standard) has certainly helped to reduce measurement errors related to different positioning of the two instruments and possibly explain the superior level of agreement we observed.
Not surprisingly, we obtained higher validity scores than other studies who compared the smartphone measurements to the ones obtained by a goniometer. Werner et al. [32], found moderate to good validity of the smartphone measurements (ICCs = 0.62 to 0.79) for the movements of FLEX, ABD, ER. Mitchell et al. [38] results were comparable to our findings (ICCs = 0.93 –0.94), but were for the ER movement only [38]. Johnson et al. [43] also reported similar findings (MDs = –1.7° –1.4°), but their results were also limited to the measurement of ABD and taken on one single participant [43].
Shin et al. [36] also obtained less accurate validity scores (ICCs = 0.72 –0.97) and very variable level of agreement (LOAs = 10° –40°) than the results of this study. Interestingly, their smartphone (“Clinometer” application) was positioned in an arm-band on the ventral side of the forearm for all the movements. This finding suggests that when the arm-band in positioned on the forearm (versus humerus), it can bias the measurements as the elbow can move and not truly reflect gleno-humeral movement; thus the arm-band should be positioned proximal to the articulation, for clinical or research purposes.
Accuracy of measurements
The accuracy of the measurements we obtained by the iPod™ appears to be good, as all are smaller than the MDC values provided by Kolber et al. [39], which are: 8° for FLEX, 4° for ABD and 9° for ER. Unfortunately, the MDC for extension is not empirically available, but according to the values reported by Kolber, a 5° MDC could be considered acceptable. We observed greater MD and measurement errors for the EXT movement. Positive MD suggests that the iPod™ overestimate movements compared to the digital inclinometer. Accordingly, considering the 95% LoA for EXT could surpass that threshold, we can certainly question the accuracy of the iPod™’s measurement for the EXT movement. This could be explained by a potential “gimbal lock” effect when the iPod™ is in a vertical position. This position causes two of the three axes to overlap during the initial (vertical) position. Thus, it is possible that this device, or its positioning, could not accurately detect very small changes in movements at the vertical starting position [44]. Further testing may be necessary for this movement to explore if the positioning of the apparatus or patient could be optimized in order to reduce the measurement error. Moreover, it may be interesting to determine if the morphological characteristics of the participant could affect the precision of the instrument during this movement, as the iPod™ positioning on the posterior aspect of the humerus may be influenced by a bulging triceps during the start of the extension movement. However, considering that therapist manipulation of the iPod™ during measurement is likely to increase the measurement error, it is essential to continue to develop procedures that allow minimal manipulation of the device. Thus, we would encourage the use of an armband to minimize the errors associated with the manipulation of the instrument by the evaluator.
When we compare our accuracy results to other studies, we observe that Werner et al. [32] also reported that the average values of the MDs ranged from 5.5° to 7.6° (95 % LOA =±8.8° to 11.6°); these values are higher (worse) than the ones we observed. Moreover, these authors found that the accuracy (standard error of measurement) of the measurements were dependent upon the level of training. This outlines the importance of procedure standardization and training prior to data acquisition (as we did in our methods), as experience or skills of healthcare professionals certainly can represent a source of error and influence the validity of measurements. The fact that their gold standard was an universal goniometer and that the measures were not taken simultaneously could also explain the high variability in the MDs and 95% LOA.
Yet, the same authors found higher ICCs than we did. The fact that their participants were symptomatic patients (with ROM deficits) may suggest that smartphone clinometers might be more valid/accurate within restricted ROM. However, as ROM values were not reported in the study, we cannot speculate on this. On the other hand, we examined the concurrent criterion validity in a wide range of possible amplitudes and we did not observe that the accuracy was influenced by total ROM.
Do the results we obtained apply towards other types/brands of smartphones? A recent study by Wellmon et al. [45] showed very good concurrent validity (MD of –0.4 to 1.2) between three phones of different manufacturers that have different types of gyroscopes, but used the same application to quantify changes in angular displacement. Thus, we do not anticipate major limitations from this aspect. Yet, future studies should continue to address this particular aspect.
Strengths and limitations
We put forward different methodological considerations to enhance the external validity and limit potential information bias. First, we separated movement amplitudes into thirds (or halves). It allowed us to gather data within a wide range of possible ROM for each movement tested and provided evidence of criterion validity of the instrument in a variety of angles. We also trained only one evaluator, standardized the procedures and the instructions to the participants and corrected any compensation from the participant –these action minimized potential measurement errors resulting from the evaluator or the patient, thus better exposing the true errors occurring from the instrument or arising from the patient. Third, we minimized measurement errors between both instruments, as both measures were taken concurrently and the fact that the inclinometer was positioned on the surface of the iPod™. We believe that these elements have helped improve the internal validity of our results, thus reflecting the true criterion validity of the instrument.
Yet, this study is not without limitations. First, there is a lack of standardized gold standard measurement of range of motion [11]. Yet as we reported in appendix 1, the digital inclinometer is likely the most “golden” gold standard available clinically. Second, although we found that the iPod’s™ measurements were valid, we only measured angles in one axis (pitch). However, the shoulder joint has 3 degrees of liberty, where motion simultaneously occurs in three axis. Thus, the measurements we took (using the pitch only as our gold standard also only used one axis) may not truly reflect these complex and multi-axial displacements. To minimize this type of error, future applications might consider computing angles based on quaternions, where angles from the three axis of the gyroscope (pitch-roll-yaw) are pondered, rather than only rely on one axis (pitch). Still, the MDs we observed between both instruments remain clinically acceptable. Another limitation is the fact that we did not include measurement of test-retest reliability, which would have provided information of the clinical procedures themselves as well as the calculation of SEM. It could also have been interesting to include symptomatic participants, in order to better study the impact of patient compensation on the results. Finally, since the speed at which the movements performed was not manipulated, the potential effect of this variable on the outcomes could not be studied.
Recommendations for practice
Smart phones are affordable and accessible to most clinicians. Yet, proper training and standardization are required to obtain valid data. Based on our results, we propose these clinical recommendations: Standardization of the clinical procedures (anatomical landmarking, instruction placement on the arm, verbal instructions, etc.) and correction of any compensation. The use of an armband to fix the device in place may limit measurement errors from both the therapist (placement error) or patient (morphological differences). As the MD of shoulder EXT measurements were greater than the LoA, these ROM measurements must be interpreted with caution.
Conclusion
Our results provide evidence that the gyroscopic functions of the iPod™ are valid for the measurement of the shoulder joint mobility in a wide range of amplitudes. We found that the measurement errors and MD between the iPod and our gold standard are smaller than the MDC for all movements, except shoulder EXT. Future studies should investigate ways to improve accuracy of shoulder extension measurements.
Conflict of interest
None to report.
Footnotes
Appendix
Appendix 1: Characteristics of the different studies that have examined the validity of smartphones for shoulder range of motion ICC: Intraclass correlation coefficient. CCC: Concordance correlation coefficient. Appendix 2: Reliability and validity of the digital inclinometer in the measurement of shoulder ROM Report 1: (39). Report 2: (40). SEM: Standard error of measurement, MDC90: Minimal Detectable Change at 90% confidence interval.
Study
Population
Application used
Gold standard
Movements studied
Validity
Reliability
Limitations of the study
(95% CI)
Intra-rater
Intra-rater
(95% CI)
Inter-rater (95% CI)
(36)
41 symptomatic patients
Clinometer on Android
Double armed goniometer
Flexion, abduction, external rotation and internal rotation
ICC≥0.72 (0.42–0.98) Limit of agreement (LOA) = 10°–40°
ICC≥0.90 (0.64–0.99) (except ICC = 0.79 for active internal rotation)
ICC≥0.70 (0.31–0.95) (except ICC = 0.64 and 0.68 for active and passive internal rotation)
•Gold standard (Goniometer)(11)
(46)
Healthy volunteers (23) and symptomatic patients (14)
mROM
2 inertial sensors
Abduction
Pearson r = 0.964 (p < 0.001)
ICC = 0.988 (0.997–0.994)
ICC = 0.994 (0.988–0.997)
•Only one movement studied
(43)
1 healthy volunteer
Customized magnetometer app
Standard goniometer
Abduction
Mean Differences (Bland-Altman plots) = –1.7° and 1.4°
CCC≥0.992 (0.967–0.999)
CCC≥0.989 (0.966–0.998)
•Only one movement studied;.
•Only one subject;
•Gold standard (Goniometer)(11)
(32)
Healthy volunteers (24) and symptomatic patients (15)
Clinometer on iPhone
Standard goniometer
Flexion, abduction, external rotation and internal rotation
Healthy: Mean ICC = 0.79 (0.89–0.99)
N/A
Healthy:ICC = 0.72 to 0.86 (0.58 to 0.92)
•Gold standard (Goniometer)(11)
Symptomatic: Mean ICC = 0.98 (0.17–0.94)
Symptomatic: ICC = 0.85 to 0.97 (0.48 to 0.99)
(38)
94 healthy volunteers
(1)GetMyROM (2)DrGoniometer
Standard goniometer
External rotation
(1) ICC = 0.94 (0.92–0.96)
(1) ICC = 0.79 (0.70–.086)
(1) ICC = 0.94 (0.87–0.98)
•Gold standard (Goniometer)(11)
(2) ICC = 0.93 (0.42–0.98)
(2) ICC = 0.81 (0.72–0.87)
(2) ICC = 0.92 (0.85–0.96)
•Only one movement studied;
(37)
25 healthy volunteers
Gyroscope
Optical motion tracking system (Optotrak)
Flexion, abduction and external rotation
Mean difference (Bland-Altman) = 3.4°
N/A
N/A
•The gold standard is not a biomechanical tracking system
Pearson r = 0.87–0.99 (except mid-abduction = 0.56 and mid-flexion = 0.78
Movement
Study
Intra-rater Reliability
Inter-rater Reliability
Validity (95% CI)
SEM
MDC90
(95% CI)
(95% CI)
FLEX
1
0,83 (0.65–0.92)
0,58 (0.13–0.80)
–
1,64°
8
2
0,95 (0.89–0.98
–
0,86 (0.71–0.94)
2 °
ABD
1
0,91 (0.81–0.96)
0,95 (0.89–0.97)
–
2,26 °
4
2
0,97 (0.94–0.98
–
0,85 (0.69–0.93)
2 °
IR
1
0,87 (0.73–0.94)
0,93 (0.85–0.97)
–
4,27 °
8
2
0,97 (0.96–0.99)
–
0,95 (0.94–0.99)
2 °
ER
1
0,94 (0.88–0.97)
0,88 (0.75–0.94)
–
2,63 °
9
2
0,98 (0.93–0.98)
–
0,97 (0.89–0.96)
2 °