
Abstract
BACKGROUND:
One-third of individuals with acute low back pain (LBP) experience recurrent symptoms within 12 months but the underlying mechanisms are unclear. One explanation is that individuals experiencing recurrent LBP develop altered central pain processing that predisposes to symptom recurrence. We compared central pain processing between individuals experiencing their first episode of acute LBP, recurrent acute LBP, and pain-free controls.
METHODS:
A cross-sectional study was conducted to evaluate central pain processing in 11 individuals experiencing their first episode of acute LBP, 11 individuals with recurrent acute LBP, and 11 pain-free controls. Outcome measures included pain and disability, pressure and heat pain thresholds (PPTs and HPTs), nociceptive flexor withdraw reflex (NFR) and conditioned pain modulation (CPM).
RESULTS:
The NFR latency was shorter in individuals experiencing their first episode of acute LBP when compared with pain-free controls (p = 0.01). Descending inhibitory pain control measured by CPM was less efficient in both acute LBP groups when compared with pain-free controls. HPTs and PPTs did not differ between people with and without acute LBP. There were no differences between the two LBP groups for any outcome measure.
CONCLUSIONS:
These data demonstrate altered central pain processing in the acute stage of LBP. However, the degree of impairment did not differ between individuals with a first episode vs. recurrent acute LBP. These findings suggest that altered central pain processing in acute LBP is not related to a previous history of LBP.
Keywords
Introduction
Approximately one-third of people with an acute episode of low back pain (LBP) experience recurrence of symptoms within 12 months, with previous episode(s) of LBP being the only consistent predictor of recurrence [1]. The mechanisms that predispose an individual to symptom recurrence are unclear, although the development of impaired central pain processing, including increased sensitivity of spinal and cortical neurons to sensory stimuli (‘central sensitisation’) and impaired descending inhibitory pain control, in response to an acute episode of LBP may contribute [2–7]. However, whether central pain processing differs between individuals experiencing a first ever episode of acute LBP and those with a history of recurrent acute LBP is unknown.
Preliminary evidence suggests central pain processing is altered in some people with acute LBP. For instance, some individuals with acute LBP have lower pressure pain thresholds, higher pain in response to electrical stimuli at remote sites (areas outside the back), enlarged reflex receptive fields and lower nociceptive flexor withdrawal reflex (NFR) thresholds than healthy controls [8, 9]. These findings suggest widespread hyperalgesia, allodynia to mechanical and electrical stimuli and enhanced spinal excitability in people with acute LBP, manifestations thought to reflect central sensitisation. In contrast, evidence for impaired descending inhibitory pain control in acute LBP is mixed, with three studies demonstrating no change and one demonstrating that although the magnitude of the descending inhibitory pain control response is unchanged in acute LBP, the duration of the response is reduced [8, 10– 12]. One explanation for these mixed findings could be that the degree of impairment in descending pain inhibition is related to a previous history of LBP. Unfortunately, it is not reported whether individuals with a prior history of LBP were included in their acute LBP cohorts. It is unknown whether changes in central pain processing are consistent in people with acute LBP regardless of pain history, or whether those with recurrent LBP display greater central sensitisation and/or impaired descending pain control, than those presenting with a first episode of acute LBP.
This study aimed to compare central pain processing between individuals experiencing i) their first episode of acute non-specific LBP, ii) recurrent acute non-specific LBP, and iii) pain-free controls. We hypothesised that: (1) individuals experiencing acute LBP, with or without a previous history of LBP, would have more evidence of central sensitisation and impaired descending inhibitory pain control than pain-free controls, and (2) individuals with recurrent acute LBP would demonstrate greater central sensitisation and impaired descending inhibitory pain control than those experiencing their first episode of acute LBP.
Methods
Study design and participants
A cross-sectional study design was used to evaluate central sensitisation and descending inhibitory pain control in: (1) 11 individuals experiencing their first episode of acute non-specific low back pain (LBP), (2) 11 individuals with recurrent acute non-specific LBP, and (3) 11 pain-free controls. All participants were age- and sex-matched. As there have been no studies of central pain processing in a first episode of acute LBP on which to base a sample size calculation, a convenience sample was used. Acute, non-specific LBP was defined as pain occurring between the 12th thoracic vertebra and the gluteal fold that lasted more than 24 hours but less than four weeks, and resulted in functional limitation [13]. Participants experiencing their first episode of LBP had no prior history of LBP. Participants with recurrent LBP had experienced an acute onset of LBP in the past four weeks, following a period of at least one month without LBP [14, 15]. The average time between the last episode of LBP and the current acute episode was 12.7 months (range: 2– 24 months). Pain-free controls had no current pain or history of any chronic pain condition. Participants were recruited from primary care clinics and the community and were included if they were at least 18 years of age and could provide written, informed consent. Individuals who presented with suspected nerve root involvement, suspected spinal pathology (fracture, tumour, cauda equina syndrome), other major diseases/disorders, neurological conditions, a history of spine surgery, psychiatric conditions, any chronic pain conditions or contraindications to conditioned pain modulation techniques (e.g. loss of sensation) were excluded. Participant characteristics are summarised in Table 1. All procedures were approved by the Human Research Ethics Committee (H10465) of Western Sydney University (Sydney, Australia) and conformed to the Declaration of Helsinki.
Participant Characteristics (mean±standard deviation)
Participant Characteristics (mean±standard deviation)
NRS- Numerical Rating Scale; PCS- Pain Catastrophising Scale; RMDQ- Roland Morris Disability Questionnaire; DASS-21- Depression Anxiety Stress Scale-21.
Pain and disability
Pain severity at testing and average pain during the past seven days were assessed using an 11-point numerical rating scale (NRS) anchored with ‘no pain’ at zero and ‘worst pain possible’ at 10. The duration of the current episode of LBP was recorded for all participants at the time of testing. Disability was assessed using the Roland Morris Disability Questionnaire (RMDQ), a reliable and valid tool in the LBP population [16]. The RMDQ has 24 items with the score totalled from the number of items checked by each participant. A higher score indicates greater disability.
Central sensitisation
Three measures were used to assess sensitisation of the central nervous system: Nociceptive flexor withdrawal reflex (NFR): Surface electromyography was recorded from the biceps femoris muscle on the side of worst LBP (or the matched side in pain-free controls). Electrical stimuli were delivered to the sural nerve within the retromalleolar pathway according to a variable interval schedule of 20 s. Each trial consisted of a volley of five 1 ms rectangular pulses with a 3 ms inter-pulse interval. Stimulus intensity was increased in 4 mA increments until a NFR was detected and then decreased in 2 mA increments until the reflex was absent. The NFR threshold was determined as the lowest stimulator intensity that elicited a NFR. The stimulus intensity was then set at 120 % of the NFR threshold and five trials recorded. The NFR was identified as the multiphasic response occurring 90– 180 ms after each stimulus. The magnitude of the reflex response was assessed as the area under the curve (root mean square). During the NFR assessment, participants rated their pain severity on an 11-point NRS [17]. The NFR is a reliable experimental test (intersession coefficient of variation = 16.9%, intraclass coefficient [ICC] = 0.82) [18]. Heat pain thresholds (HPTs): were measured using the conditioned pain modulation system (Thermal Sensory Analyzer, TSA-2001, Q-Sense-CPM, Medoc Ltd, Ramat Yishai, Israel). A 30×30 mm Peltier-based thermode was placed on the skin. The temperature started at 32°C and increased at a rate of 0.5°C/s. Participants were instructed to push a button when the sensation of heat first turned to one of pain. For both LBP groups, HPTs were measured at the site of worst LBP, the opposite side of the lumbar region and the ventral aspect of the forearm on the side of worst pain. For pain-free controls, HPTs were measured 3 cm lateral to the L3 spinous process bilaterally and over the ventral aspect of the forearm of the dominant hand. Three measures were made at each site and the average at each site used for analyses. HPT measures have been shown to be reliable in LBP populations (coefficient of repeatability [CR], 7.4°C) [19]. Pressure pain thresholds (PPTs): A handheld pressure algometer (Somedic, Hörby, Sweden, probe size 1cm2) was applied at the site of worst LBP and over a remote site (thumbnail ipsilateral to the side of worst pain) in both LBP groups. For pain-free controls, PPTs were measured 3 cm lateral to the L3 spinous process on the side of the dominant hand and over the thumbnail of the dominant hand. Pressure was applied at a rate of 40 kPa/s and participants used a hand-held trigger to indicate when the sensation of pressure first changed to one of pain. Three measures were made at each site and averaged for analysis. PPT measures have demonstrated acceptable reliability in LBP population (CR, 162.7 kPa) [19].
Descending inhibitory pain control
Descending inhibitory pain control was assessed as the change in pain perceived in one body region (test stimulation [TS], pressure pain threshold) as a result of pain induced in another body region (conditioned stimulation [CS], heat pain). Pressure (pressure pain threshold) was used as the test stimulus and heat pain (1°C above the heat pain threshold) as the conditioned stimulus using a conditioned pain modulation (CPM) System (Thermal Sensory Analyzer, TSA-2001, Q-Sense-CPM, Medoc Ltd, Ramat Yishai, Israel). Three PPTs were measured before the application of heat pain (TS1). Heat pain was then applied via a 30×30 mm thermode. Three PPTs were re-measured 30 seconds after applying heat pain (TS2). Participants were instructed to rate their pain on a numerical rating scale (0– 100) at 0 s, 30 s and at the end of the trial. Pain scores were maintained between 50 and 80/100 during testing. These pain scores were not used in the analyses. Participants completed two trials in random order: i) pressure at the site of worst LBP and heat on the opposite forearm; ii) pressure at the ipsilateral forearm and heat on the low back opposite to the side of worst pain. This is a standard procedure (type and sites of stimuli) to induce a CPM response [20]. The magnitude of the CPM response was measured as TS2 minus TS1. A positive value indicates a normal CPM response. The CPM paradigm has shown good intrasession reliability (ICC > 0.75) [21].
Psychosocial questionnaires
Psychosocial factors were assessed using (i) The Pain Catastrophising Scale- a reliable and valid, 13-item self-report instrument to assess patients’ thoughts and feelings about pain in the domains of magnification, rumination and helplessness [22] and (ii) The Depression Anxiety Stress Scale- 21 (DASS 21) - a reliable and valid, 21-item self-administered questionnaire to measure negative emotional states of depression, anxiety and stress [23]. Higher scores in the subscales indicate more severe condition of depression, anxiety and stress. Pain-free controls completed only the DASS-21.
Statistical analyses
Pain characteristics (severity and duration), and scores from the RMDQ and the Pain Catastrophising Scale were compared between individuals with a first episode of acute LBP and those with acute, recurrent LBP using Wilcoxon signed rank tests. The scores from the DASS 21 were compared between groups (first episode, recurrent, pain-free) using the Kruskal-Wallis test. Outcome measures for sensitisation and descending inhibitory pain control were compared between groups (first episode, recurrent, pain-free) using a one-way analyses of variance (ANOVA). Data that were not normally distributed were log transformed. ANOVA on ranks was performed where data were not normally distributed after log transformation. Post-hoc tests were performed using the Holm-Sidak method corrected for multiple comparisons. Cohen’s d effect sizes were calculated to analyse effect estimates: d≤0.2 is small, 0.5 represents medium, ≥0.8 is large (24). A P < 0.05 was considered significant. SigmaPlot (Systat Software Inc.) was used to analyse the data. Results are presented as means and standard deviations in the text unless otherwise stated.
Results
Pain characteristics and psychosocial factors
Participants in both LBP groups had experienced a similar duration of pain (W = – 1, Z = – 0.06 p = 1.0), and had similar pain severity at the time of testing (W = 3, Z = 0.15, p = 0.92) and in the past seven days (W=– 7, Z = –.042, p = 0.73) (Table 1). There were no differences between the two LBP groups in RMDQ score (W = 17, Z = 0.87, p = 0.43), PCS total scores (W = – 13, Z = – 0.58, p = 0.58) or any of the subscales (rumination W = – 32, Z = – 1.43, p = 0.18; magnification W = – 12, Z = – 0.6, p = 0.56; helplessness W = – 1, Z = – 0.05, p = 1.0). There were no between– group differences for the DASS 21 (depression: Kruskal-Wallis H (2) = 2.25, p = 0.33; anxiety: Kruskal-Wallis H (2) = 3.62, p = 0.16; stress: Kruskal-Wallis H (2) = 2.34, p = 0.31).
Central sensitisation measures
Nociceptive withdrawal reflex
NFR responses could not be elicited in two participants experiencing their first episode of LBP as they were unable to tolerate electrical stimuli to the sural nerve. There was a significant between-group difference in NFR latency (F2,28 = 5.23, p = 0.01). Post hoc analyses revealed a shorter NFR latency in individuals experiencing their first episode of acute LBP when compared with pain-free controls (p = 0.01, Cohen’s d = 1.44), but no difference between those with a first episode and recurrent acute LBP (p = 0.09) or between those with recurrent acute LBP and pain-free controls (p = 0.25) (Fig. 1). There were no between-group differences for NFR amplitude (ANOVA on Ranks H (2) = 1.39, p = 0.50), threshold (ANOVA on Ranks H (2) = 3.68, p = 0.16) or NFR pain intensity (F2,28 = 0.92, p = 0.41).
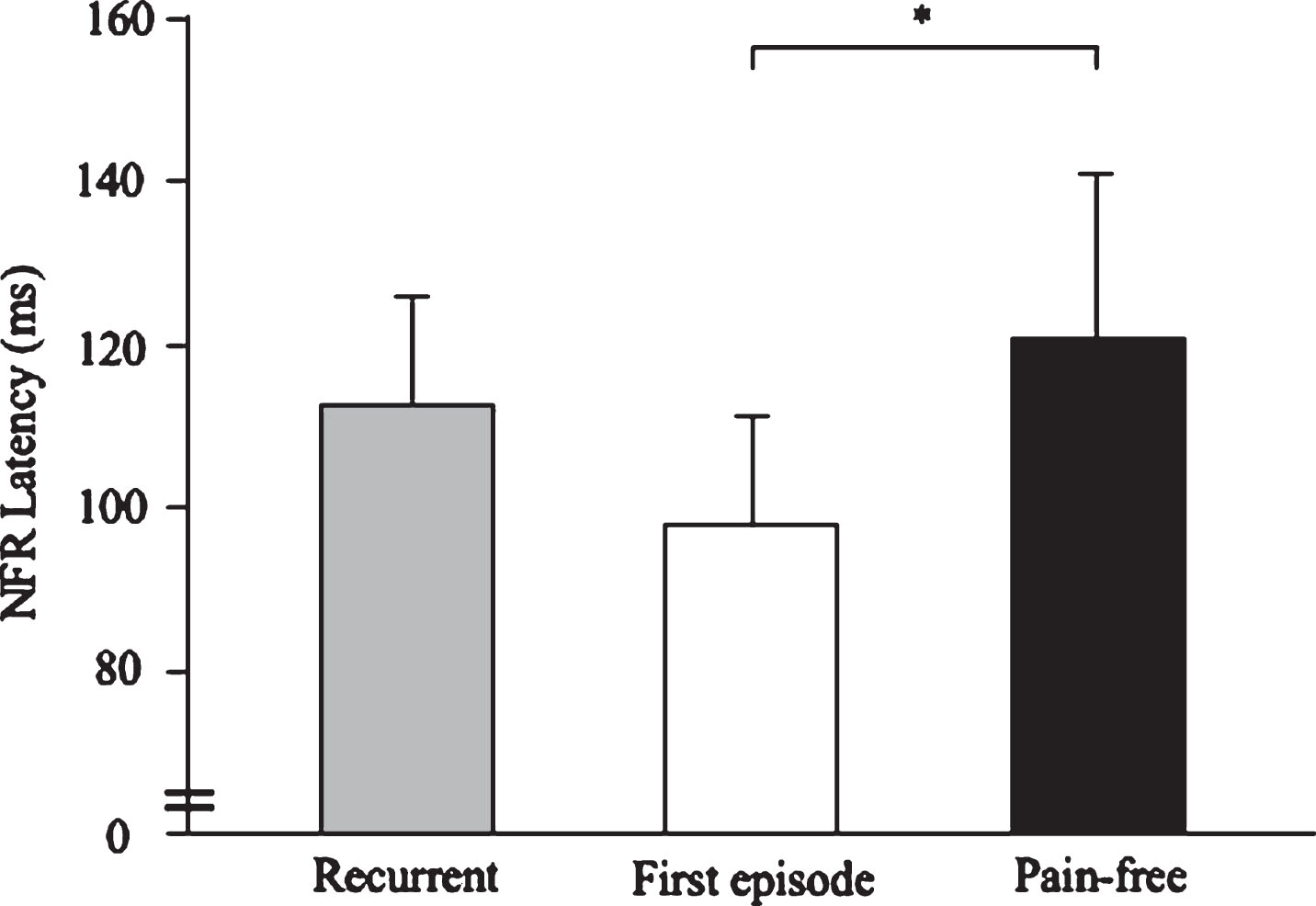
Group data (mean and standard deviation) demonstrating the latency of the nociceptive flexor withdraw reflex (NFR) in individuals with recurrent acute low back pain (LBP), individuals with their first episode of acute LBP, and pain-free controls. *p = 0.01 between groups.
HPTs could not be assessed in two participants experiencing their first episode of LBP due to a loss of thermal sensation and PPTs could not be assessed in one participant experiencing their first episode of LBP due to the intensity of their pain. There were no significant between-group differences in HPTs at the lumbar (LBP site F2,28 = 0.39, p = 0.68; opposite to LBP site F2,28 = 0.73, p = 0.49) or forearm (F2,28 = 0.20, p = 0.82) sites. Similarly, there were no between-group differences in PPTs measured at either the lumbar (ANOVA on Ranks H (2) = 3.38, p = 0.18) or thumb (ANOVA on Ranks H (2) = 3.49, p = 0.18) sites.
Descending inhibitory pain control
Responses could not be assessed in three participants experiencing their first episode of LBP (two participants did not have HPT measures while the conditioned stimulus was unable to induce the required pain intensity within the safety limit of the CPM device in one participant) and in one pain-free participant (unable to induce the required pain intensity within the safety limit). In one additional pain-free control, the CPM response was only elicited when PPTs were measured at the lumbar site. When heat pain was applied at the lumbar region opposite to the side of worst LBP, the change in PPT at the forearm was different between groups (F2,25 = 5.95, p = 0.01) (Fig. 2). Post hoc analyses revealed a greater increase in the PPT in pain-free controls (reflective of a normal CPM response) when compared with individuals experiencing their first episode of LBP (p = 0.01, Cohen’s d = 1.62) and in those with acute recurrent LBP (p = 0.04, Cohen’s d = 1.10). There was no difference between individuals with acute recurrent LBP and those with a first episode of LBP (p = 0.28). When heat pain was applied at the forearm opposite to the side of LBP, there was no difference in the PPT response between groups (F2,26 = 3.16, p = 0.06).
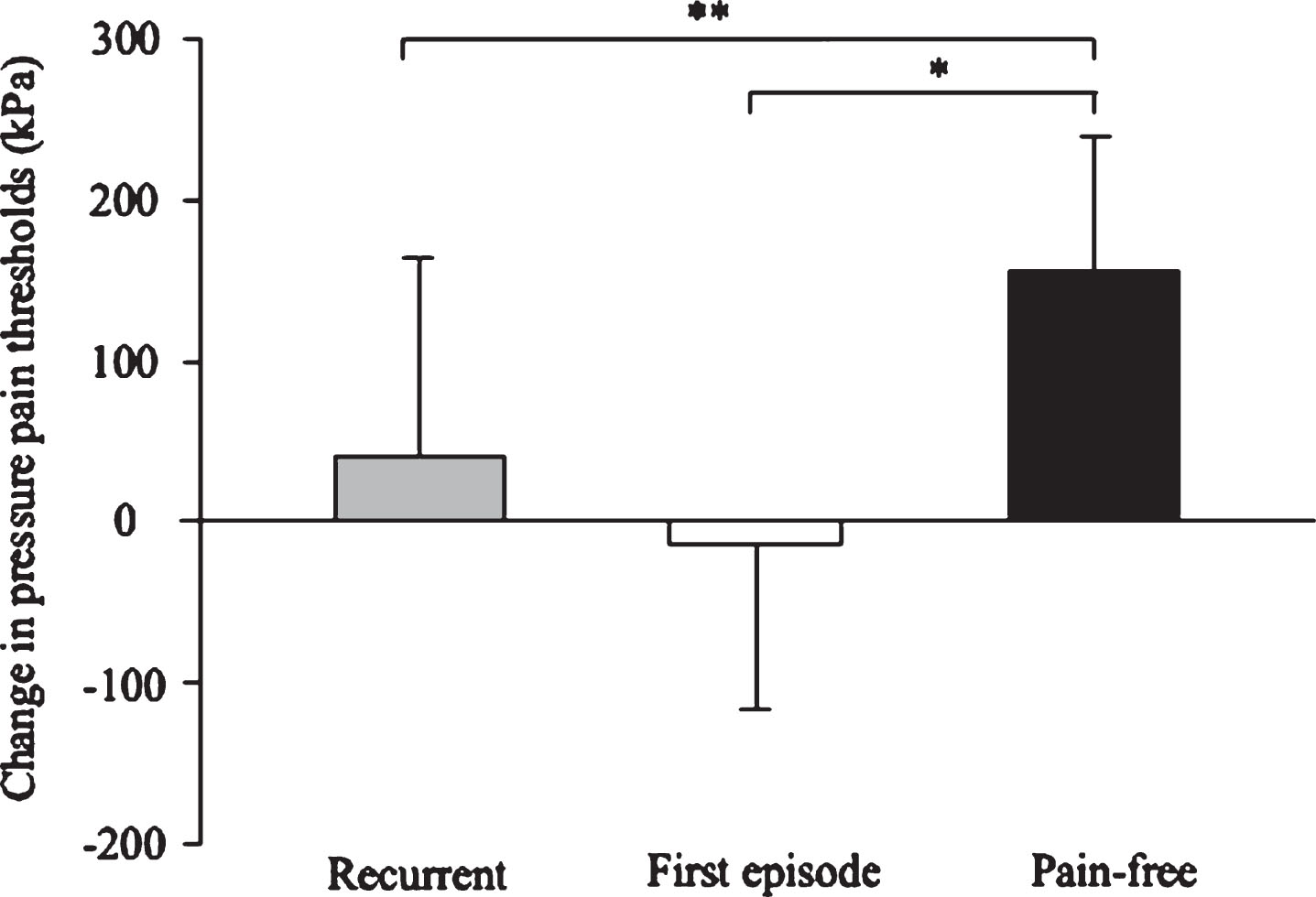
Group data (mean and standard deviation) demonstrating the conditioned pain modulation (CPM) response in individuals with recurrent acute low back pain (LBP), individuals with their first episode of acute LBP, and pain-free controls. *P = 0.01 between groups and **P = 0.04 between groups.
This preliminary study is the first to compare central pain processing, including central sensitisation and descending inhibitory pain control, between individuals with a first ever episode of acute LBP and those with recurrent acute LBP. Individuals experiencing a first episode of acute LBP had increased spinal excitability (shorter NFR latency) when compared with pain-free controls but there was no difference between the two LBP groups. Individuals experiencing acute LBP, with or without a previous history of LBP, demonstrated less efficient descending inhibitory pain control when compared with pain-free controls. Our findings provide some evidence that descending inhibitory pain control is altered in the acute stage of LBP. However, contrary to our hypothesis, individuals with recurrent acute LBP did not demonstrate a greater degree of impairment than those experiencing their first episode of acute LBP. These findings suggest that LBP recurrence may not be related to altered central pain processing in the acute stage of pain.
Recurrent episodes of acute LBP are common, and it is now acknowledged that this clinical pattern reflects a persistent condition with a variable course, rather than a series of unrelated occurrences of pain [7, 25]. This definition suggests the presence of biopsychosocial changes that do not resolve during a period of relative remission, predisposing to recurrence of LBP. A number of authors have suggested that altered central pain processing may be one mechanism that contributes to recurrence of LBP [2–7].
Central pain processing can be evaluated in humans through exploration of central sensitisation and descending inhibitory pain control mechanisms. These mechanisms are believed to play a critical role in determining an individual’s pain experience [26–28]. For instance, pain facilitation occurring via central sensitisation mechanisms produces hyperalgesia in response to injury (or the threat of injury) that is thought to enhance the healing of injured tissue [4, 29]. Conversely, descending inhibitory pain control downregulates nociceptive input resulting in analgesia that is thought to assist with escape from potentially dangerous situations [26, 30]. Although these mechanisms are adaptive in the short-term, central sensitisation and deficient descending inhibitory pain control have been implicated in the pathogenesis of musculoskeletal pain when pain is idiopathic and persists beyond normal tissue healing times. For instance, systematic reviews demonstrate increased spinal excitability in a range of chronic musculoskeletal pain disorders including primary headache, fibromyalgia, chronic knee pain and whiplash injury [31], widespread hyperalgesia in chronic shoulder and osteoarthritis knee pain [32, 33], and impaired descending inhibitory pain control in fibromyalgia, headache, arthritis, and some visceral and neurological conditions [34]. These findings provide a basis for the hypothesis that central sensitisation (manifesting as increased spinal excitability and widespread hyperalgesia) and deficient descending inhibitory pain control may contribute to the development of chronic and recurrent musculoskeletal pain [2–6]. However, evidence in support of this hypothesis is limited as i) few studies make the distinction between chronic continuous, and chronic recurrent pain, and ii) research investigating central pain processing in recurrent musculoskeletal pain conditions is scarce.
Only two studies have examined central pain processing in recurrent LBP, reporting normal descending inhibitory pain control and an absence of widespread hyperalgesia in this population [35, 36]. Notably, both studies provide evidence of altered central pain processing in chronic continuous LBP [35, 36]. Our data extend these findings by examining central pain processing in the acute stage of LBP, demonstrating that although descending inhibitory pain control is less efficient during an acute episode of LBP, this does not differ based on a previous history of LBP. Taken together, these data suggest that altered central pain processing is not a distinguishing feature of recurrent acute LBP and suggest that changes in central pain processing may develop as a consequence of sustained, rather than episodic, pain.
Although longitudinal studies that examine the same individuals during periods of remission and recurrence are needed to confirm that altered central pain processing does not play a role in recurrent LBP, the findings of this preliminary study suggest that other mechanisms may be important. Although evidence is limited, previous studies have shown that individuals with recurrent LBP have delayed activation of the deep back muscles on the previously painful side and greater trunk stiffness while performing trunk perturbation tasks during a period of remission [37, 38]. These data have been interpreted to reflect the adoption of maladaptive movement strategies that persist even when pain is absent and that may compromise spinal loading and predispose to LBP recurrence [37–39]. This hypothesis is supported by a loss of discrete motor cortical organisation of the paraspinal muscles in individuals experiencing chronic recurrent LBP [40], suggesting a possible association between motor cortical reorganisation and recurrent LBP. In addition, psychosocial factors such as depression, anxiety, pain catastrophizing and pain self-efficacy may be relevant to the development of recurrent LBP. For example, symptoms of depression and work-related factors (e.g. low decision authority and low job satisfaction) increased risk of recurrent LBP and may play an important role in symptom recurrence [41–43]. Indeed, evidence suggests that psychosocial factors can influence central pain processing [28, 45]. However, in the current study psychosocial factors were not different between those experiencing their first episode of acute LBP and those with recurrent acute LBP. Further research is needed to identify the biopsychosocial factors that contribute to the development of recurrent LBP.
This preliminary study has several limitations. As the first study to compare central pain processing in individuals with recurrent acute LBP and those with a first episode of acute LBP, there were insufficient data on which to base a sample size calculation. While we can likely rule out the large effects of the past history of LBP on altered central pain processing in the acute stage of LBP, we acknowledge that we may not be powered to detect less notable effects. Future studies with a larger sample size are needed to confirm the current findings. Further, research indicates that a history of three or more previous episodes of LBP triples the odds of recurrent pain within 12 months [46]. Thus, individuals reporting 3 or more previous episodes of LBP may have greater changes in central pain processing than those reporting one or two previous episodes of LBP. However, our sample size was insufficient to investigate an effect of the number of previous LBP episodes on central pain processing. Finally, the average acute pain intensity at the time of testing was relatively mild (2.7 and 2.8 points on a 11-point NRS) for the two acute LBP groups. Future studies should seek to include individuals with a greater intensity of acute pain to represent a wider acute LBP population.
Conclusion
This study confirms the presence of altered central pain processing in acute non-specific LBP compared with pain-free controls. However, there is no difference in central pain processing between individuals with a first episode and recurrent acute LBP. These data suggest that altered central pain processing in acute LBP is not related to an individual’s previous history of LBP.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This research was supported by the National Health and Medical Research Council of Australia [grant number 1059116]. WJC (1094434) and SMS (1105040) received salary support from the National Health and Medical Research Council of Australia and VB from Western Sydney University Postgraduate Research Award Scholarship. The authors report no conflicts of interest.