
Abstract
BACKGROUND:
Unimanual activities are suggested as an effective intervention for the moderately or severely affected chronic stroke patients and bimanual activities for mildly affected cases in mirror therapy.
OBJECTIVE:
To observe the feasibility of unimanual mirror therapy to improve the motor skills of the effected hand in mild chronic stroke patients.
METHODS:
In this is case series study, n = 20 mildly affected chronic stroke patients were screened for participation in a nursing home setting. They were 45–60 years of stroke included ischemia (n = 3) and aneurysm (n = 1) of anterior cerebral artery, median time:3 years. The gross (Fugl-Meyer Assessment test), fine motor (Box and Block Tests) skills, the tripot pinch grip power (JTech Commander PichTrack) were assessed at baseline and post intervention. The intervention supervised included unimanual activities of the non-affected hands for 30 min, 5 days/week for 6 weeks.
RESULTS:
N = 4 participants were recruited from a nursing home setting; median age: 45, Gender: 3M; 1W. The causes of stroke included ischemia (n = 3) and aneurysm of anterior cerebral artery (n = 1). The median years of stroke was 3 years. The improvement in the gross motor skills (25%) of affected sides after unimanual training may be considered as feasable. There were also increase in tripot pinch grip power of the non-affected (34%) and affected hands (17%). The improvement in fine motor skills were 19% in affected hands the 10% in non-affected hands.
CONCLUSIONS:
The unimanual mirror therapy resulted in improvements in gross and fine motor skills and tripod pinch grip power of the affected hands of mild chronic stroke patients. This case series provides further evidence that mirror therapy is effective to improve function in patients with mild chronic stroke.
Introduction
Stroke or cardiovascular accident is a primary cause of disability and a secondary cause of death worldwide. Feigin et al., [1] reported that every year 15 million people have a new or recurrent stroke, which may occur due to a sudden blockage of brain arteries resulting with ischemic stroke or a sudden burst of brain vessels resulting with hemorrhagic stroke in the brain tissue or in the subarachnoid area [2]. According to the Global Burden of Disease Study, 80 million people had stroke globally in 2016. Among them 40.1% were women and 39% were men [3]. A recent report of Public Health England [4] estimated the rate of stroke as 1.07% among 1000 person in 2016, and reported a slight increase compared to the outcomes of 2013 that was 1.03% among 1000 person. Although the reporting of stroke globally is well documented in Global Burden of Disease Study, the recording and reporting of the incidence of stroke in Turkey as a middle-income country are limited. They were 72,844 incidence of ischemic stroke and 25,194 incidence of hemorrhagic stroke in Turkey in 2016 [3]. Elsewhere, it was reported that the incidence of stroke in Western Anatolia was 0.9% with 0.68% among males and 1.21% among females; the mean age (standard deviation) of stroke as 72.4±8.1 years [5]. Another recent study done by Boru et al. [56] among 2906 people in a rural area of Istanbul, stated that the rate of incidence was 1.7%. These reports on incidence of stroke are variable, this may be related to the general consideration that the incidence of stroke in lower- and middle-income countries have a tendency to increase and in high-income countries to decrease [3]. The main reason of this thought to be the increased awareness among the general population of the risk factors for cardiovascular diseases and stroke [1, 2]. However, as a chronic condition stroke may have serious consequences on the daily living functions of patients having physical, sensorial or cognitive disabilities (7). The improved stroke survival is the leading cause of the increased lived years of disability globally [3]. Thus, in addition to the preventive measures for stroke, improving the quality of life of people with stroke especially during their activities of daily life is increasing its importance worldwide.
Mirror box therapy (MBT) is a relatively novel sensorimotor training strategy aiming to promote functionality in stroke patients as an additional intervention to conventional neuromuscular rehabilitation techniques [8–10]. The visual input of the non-aff-ected side on the mirror is perceived as originating from the affected side [11, 12] therefore, the patients perceive that the activities are performed by the aff-ected side [13, 14]. Although this is a unilateral movement (daily living activities performed with one hand) we may define it as bilateral (daily living activities performed with both hands) if the affected hand is also actively involved to the perceive movement. This is a cortical activity may be explained by the flow of the information from the posterior parietal cortex to the premotor cortex via visual feedback on the mirror to compensate the missing normal somatosensory feedback of the limbs due to the stroke [15]. The other consideration of MBT is the inverse creation of the limb image on the mirror creating a visual illusion that activates the mirror neurons located in the ventral and inferior premotor cortex normally responsible for observing and imitating the movements [16, 17]. However, self-awareness and spatial attention enhanced by the superior temporal gyrus, precuneus and posterior cingulate cortex are also effective to visualize the image of the moving limb on the mirror as if it is the affected side to reduce its learned non-use [13].
Thus, MBT has been shown to promote motor recovery and functionality of the affected side and increase mobility and muscle strength in stroke patients [10, 18]. The bimanual activities are sugges-ted for mild chronic stroke cases and and unimanual activities for moderate to severe stroke cases with increased tone [10, 11]. Arya and Pandian [19] in their single-group design study searched the effectiveness of task-based mirror therapy on motor reco-very of upper extremity in chronic stroke patients (n = 13) who were asked to perform tasks with their non-affected upper extremity while observing in the mirror box along with conventional management. They reported that the task-based mirror box therapy improved wrist and hand motor performance from 41% to 54% in chronic stroke patients, and bimanual activities are more beneficial then unimanual activities in moderately affected chronic stroke cases [19]. However, unimanual mirror therapy was found more beneficial than bimanual mirror therapy for functi-onal improvement of affected side as reported by Selles et al. [20]. Selles et al. [2014] stated that this may be due to the disinformation, which occurred between visual feedback and the proprioceptive sense during bilateral mirror therapy and they explained that the actual proprioceptive feedback achieved from paretic hand in the mirror box and the visual feedback achieved from the mirror box image of the non-affected hand activities were not congruent to each other during bilateral training in the mirror box. The-refore, they suggested unimanual mirror therapy for moderate to severely impaired and bimanual mirror therapy for less affected cases of subacute or chronic stroke patients [20]. Although bilateral activities have been studied by researchers in mirror therapy of mil-dly stroke patients with different functional abilities [9, 17], to our knowledge, task-based unimanual act-ivities common to daily living life (such as collecting coins, selecting a particular beads among others or point a spot on a fabric while the other hand is at rest) have not been studied extensively for the mildly affected stroke cases. Therefore, the aim of this study was to conduct a case series to explore if unimanual mirror therapy resulted in improved motor skills of the affected hand of the mildly affected chronic stroke patients.
Methods
Patients
This is a case series study 20 chronic stroke patients in a nursing home were screened for eligibility (Fig. 1) The inclusion criteria, which were: (1) mild to moderate spasticity in the upper limb, with a score of 2 on the Modified Ashworth Scale (MAS), with marked increase in muscle tone, manifested by a “catch” in the middle range and resistance throughout the remainder of the range of motion, but with effortless movement of the affected part(s) [21, 22], (2) a minimum of Brunnstrom Motor Healing (BMH) Stage 3 [23, 24], (3) sufficient cognitive ability to follow instructions (Mini-Mental State Examination score≤24) [25], (4) ability to use the affected hand to perform activities of daily living (ADL). Patients with any cardiovascular or respiratory problems that may have prevented their participation in the procedures and those who did not volunteer to participate were excluded. The study was performed between June 2015 - January 2016. The Non-in-vasive Clinical Research Ethical Committee of Medipol University provided ethical approval (140-30.3.2015), and all participants provided informed consent. We used the CARE checklist when writing our report [26].
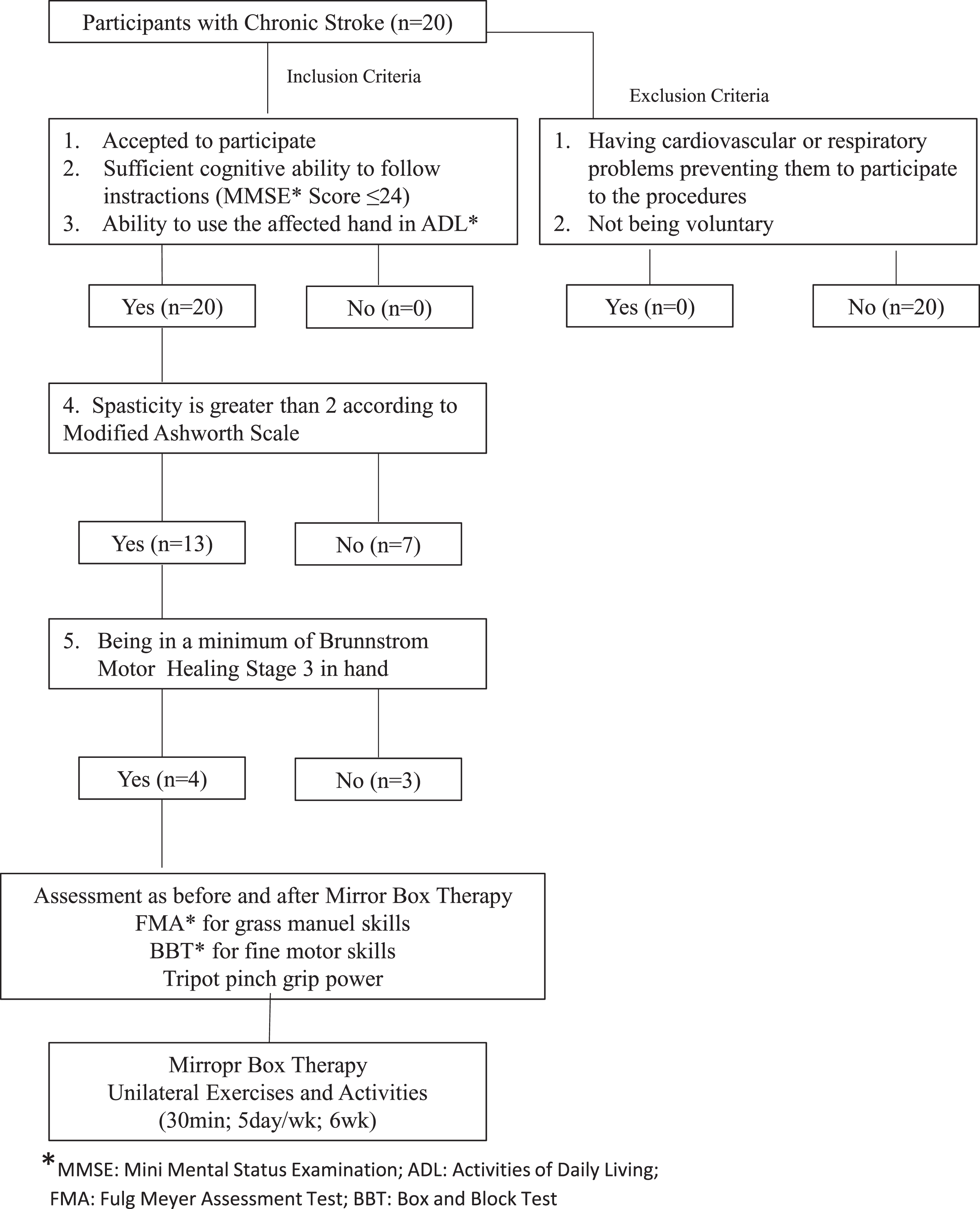
Flow chart of the selection of patients and the study desing.
Assessment
Both hands were assessed by using the Fugl-Meyer Assessment Test (FMA) for gross manual skills [27], the Box and Block Test (BBT) for fine motor skills [28], and a dynomometer (JTech Commander PichTrack) for measuring the tripot pinch grip power [29], before and after the mirror box treatment sessions by the same physiotherapist (HNO). The FMA is a quantitative assessment tool of upper-extremity gross motor skills in stroke patients. The FMA assesses motor recovery with total scores for the whole body ranges from 0 to 66 and for the hand 0–14. The individual items rated on a 3-point scale as: cannot perform: 1, can perform partially: 2, can perform completely: 3. Any increase in the achieved outcome is considered as improvement clinically. The FMA’s intraclass correlation coefficient for the upper extremities has been reported at 0.97 [30, 31]. The BBT is used to assess gross manual dexterity in patients. The patients were tested while sitting on a chair in front of a table at their waist height where a box with two divisions was placed; one side contained blocks of different sizes (n = 150) and the side other was empty. Participants were asked to transfer as many blocks as possible from one side to the other within one minute (transferring only one block at a time). The highest number of blocks transferred within one minute at baseline and post intervention is compared, as a measure of improvement. The BBT’s intraclass correlation coefficient was reported to range from 0.89 to 0.97 [32]. The tripot pinch grip power was tested while the patients sat in front of a table, with their forearms resting on the table at a neutral position; they were asked to squeeze the handles of a make mode dynamometer (lb.) with their first, second, and third fingers as if pinching [33]. The test was repeated three times, and the best score was recorded in pounds. The intraclass correlation coefficients for both the affected and unaffected hands in patients with different orthopedic and neurological hand problems were reported at >0.90 [34].
Treatment
The activities were performed by the non-affected hand while the affected hand was inside the mirror box, which was a prism open at both ends with dimensions of 30×30×30 cm and covered with a mirror on both sides in one of the rooms of exercise unit in the nursing home which the participants are familiar with. The patients were able to observe image of their non-affected hand that is the moving hand on the mirror and were expected to have the impression that as if they were performing the activities with their affected hand (Fig. 2). The treatment procedure was explained to each participant before the intervention started, and the participants were asked to practice each procedure (2 min each) for acclimation to the procedures of the MBT. The treatment were performed for 30 min for 5 days/week for 6 weeks, for a total of 30 sessions. All the acclimitatisation exercises and the unilateral mirror therapy activities were supervised throughout the treatment session by the same physiotherapist (HNO) for the uniformity of the study. These activities were: Range of motion exercises of both affected and non-affected hand and wrist joints such as flexion, extension, radial deviation, ulnar deviation, supination, and pronation bilaterally were performed repetitiously for 5 min, The same range of motion exercises were performed by the non-affected hand and wrist joints while the affected hand was inside the mirror box. Activity of daily living (ADL) exercises were performed by the non-affected hand while the affected hand was inside the mirror box. They were all unimanuel activities for fine motor skills (placing beads and pegs in a hole, flipping a card, copying shapes on a paper with a ball-pen, and transferring beans to another box, pointing on collors) and gross motor skills (squeezing spongles, building blocks).

Unimanual activities of mirror box therapy.
The data were analyzed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). The descriptive statistical data as the means, standard deviations, and percent values were done for each participant.
Results
The achieved results for each case who were selected according to the inclusion criteria were as follows (Table 1);
Characteristics of cases
Characteristics of cases
*ACA: Anterior Cerebral Artery.
He had no spasticity, his lower extremity was well coordinated (BMH Stage: 6/6), and he was able to use his upper limb and hand in his activities of daily living but facing mild difficulty in using fingers separately from each (BMH Stage: 5/6).
They were able to use their affected hands in their daily living to support their non-affected sides. Although the first and second cases were having difficulty in using their fingers separately during the bilateral functional activities, they all expressed that they always had to look at their hands during the activities.
The outcomes achieved from the functional tests as fine and gross motor skills and pinch power before and after mirror box therapy are available in Table 2 and Table 3. According to these outcomes, we found improvement only in the gross motor skills (25%) of the affected hands of the patients. There was also an increase in the pinch grip power of the non-affected hands (34%) possibly due to the strenthening effects of the given exercises.
The outcomes of cases as before and after the mirror therapy
†MBT: Mirror Box Therapy.
Comparison of the outcomes of unimanual activities among the cases
†MBT: Mirror Box Therapy, *AffH: Affected Hand, **nAffH: Non Affected Hand.
In the review study of Stoykov and Corcas [11] it is stated that bimanual gross motor skills seem to be more beneficial than unimanual activities in mirror therapy having mild stroke. Selles et al. [20] supported this outcome by suggesting unimanual mirror therapy for moderately impaired chronic stroke cases. However, this study, demonstrated an improvement in unimanual motor skills of the affected hand in mild chronic stroke patients. We observed that activities with unimanual mirror therapy have potential to improve the unimanual gross motor skills of the affected hands (25%) of mildly chronic stroke cases active in their daily living.
Although, this is a case study of four, this outcome may be considered as an exercise design emphasizing on unimanual activities of non-affected side during mirror therapy. A recent study by Gehan et al. [34] stated the significant effect of mirror therapy on motor function of the upper extremity and affirmed the importance of unimanual activities. Thieme et al. [8, 14] and Christina et al. [19] reported both bimanual and unimanual mirror therapy as an effective intervention for the upper limp recovery and functionality in activities of daily living of chronic stroke cases in neurologic rehabilitation. Thus, in the light of our outcomes, we may suggest unimanual activities to be included into the mirror therapy regimes in addition to bilateral activities to improve the function of the affected hands.
Though there were minor changes in the fine motor skills and tripot pinch grip of the affected hands of the cases in the current study, these may also be taken in considerations for the future studies. Possible reasons for these minor changes may be due to the higher dexterity and power in hands required for these movements [28]. However the longer sessions of mirror therapy may result in more beneficial improvements for fine motor skills and tripot pinch grip [35].
Therefore, we suggest unimanual mirror therapy activities of the non-affective side as an associated intervention to the individualized physiotherapy program for the patients with mild chronic stroke [35]. However, compared to individualized exercise therapy programs mirror therapy stimulates the patients to increase their attention and to focus on the performed activity [29]. In this context, we may suggest for the future studies to observe the effect of enthusiasm and motivation of patients in repeating the activity against the mirror while watching their illusions.
Unfortunately, we have not observed any difference in the affected side of fine and gross motor skills of the fourth patient though presented some improvement in non-affected side in both skills. This could be in relation to the lack of interest of the patient on the effectiveness of the mirror box therapy. However, since we did not assessed the motivations nor the quality of life of the participants during our interventions, these may be considered as a limitation of this study. Therefore, searching the motivation and quality of life of the participants by means of reliable questionnaires could be considered for future studies. The other limitation of this study is methodologically in which the same physiotherapist performed the mirror therapy and the assessments, which may have created bias. Future studies should consider having a different interventionist and assessor.
We conclude that unimanual mirror therapy results in improvements in gross motor skills of the affected hands of chronic stroke patients in minimum 6 weeks (30 sessions of 30 min each). However, we believe that comparative studies on MBT may have added value for future studies.