
Abstract
PURPOSE:
Abnormal breathing patterns, decrease in respiratory muscle strength and endurance are some of the alterations, which are observed in non-specific low back pain (NS-LBP). The purpose of this study was to determine the efficacy of the Feldenkrais method (FM) on respiratory muscle strength, Maximum Voluntary Ventilation (MVV), Total Faulty Breathing Scale (TFBS), Cloth Tape Measure (CTM) and core stability among NS-LBP participants.
METHODS:
Participants were recruited from a rehabilitation clinic and randomized either to experimental group (EG) or the control group (CG). For the EG (FM and routine physiotherapy), and for the CG routine physiotherapy alone were carried out three days per week over a period of 8 weeks. Outcome measures including Respiratory Muscle Strength, MVV, TFBS, Numeric Rating Scale (NRS), CTM, and Pressure biofeedback device (PBU) were evaluated at baseline and 8 weeks.
RESULTS:
Forty participants were assigned to an EG (n = 20) and CG (n = 20) based on the study criteria. There was a significant increase in inspiratory muscle strength (MIP) (p = 0.004) for the EG, but no significant change in the CG (p = 0.455). There was also a significant increase in the expiratory muscle strength (MEP) for the EG (p = 0.001), but no changes in the CG (p = 0.574). In addition, decrease in pain, increase in xiphoid process chest expansion and improvement in core stability were observed in EG and improvement in MVV was observed in CG.
CONCLUSIONS:
FM is a potential training program that can improve respiratory variables among NS-LBP.
Introduction
Feldenkrais is an educational approach whereby people correct their faulty movement patterns through self-exploration of their own bodily movement [1]. The Feldenkrais method (FM) is recommended as an alternate therapy in the field of musculoskeletal practice and is increasingly being used in current practice [2, 3]. The FM approach is directed through two methods which are Awareness Through Movement (ATM) and Functional Integrations (FI). The fundamental principles related to efficient use of the neuro-musculoskeletal system in FM are reduction of effort, attending body’ parts, speed of movement, coordinated well-learnt action, co-contraction of muscles and respiratory mechanic principles [1]. A key aspect of FM is to pay attention to and develop awareness of breathing to maximize movement patterns, which eases the aggravating symptoms [4]. The FM breathing mechanic principles focus mainly on movement of the diaphragm and movement of the rib cage [1].
Recently, there has been renewed interest regarding the involvement of respiratory characteristics in NS-LBP [5–7]. A case-control study of 18 participants with Chronic LBP and 29 healthy subjects examined the function of the diaphragm during postural limb activities in performing isometric flexion of upper and lower limbs. The study concluded that participants with chronic LBP had an abnormal diaphragm position and the steeper slope of diaphragm using Magnetic Resonance Imaging [5]. An earlier study hypothesized that the increased respiratory demand compromises spinal control, especially in individuals with LBP [6]. The study was carried out comparing healthy controls to participants with LBP using trans diaphragmatic pressure; findings suggested that the individuals with LBP exhibit greater diaphragm fatiguability compared to healthy controls [6]. Additionally, a recently published study suggested that eight weeks of IMT showed an increased reliance on back proprioceptive signals during postural control, increased in inspiratory muscle strength, and reported a deficit associated with LBP severity [7]. In addition, it was projected that the models such as multifactorial model, a model of movement dysfunction, and ‘Puzzle’ model theorized that there existed a relationship between LBP and respiratory variables [8–10]. These studies suggest a relationship between LBP and respiratory characteristics. Therefore, the exercises that are related to the respiratory component of FM will be advantageous to LBP population, and there is a clear need to explore this area of research.
The existing body of research on FM suggests that FM helps to manage pain for people with LBP following a single session of ATM which was implemented through pre-recorded tape for visualization and breathing sequences [11]. Recently, investigators have examined the efficacy of FM for relieving pain in people with LBP and investigated the improvement of interoceptive awareness, which is the ability to detect internally generated bodily signals involved in maintaining the homeostasis [12]. The intervention used in the study was based on ATM lessons for a period of five weeks. It has been observed that FM was more effective in improving visual analogue scale (VAS) and McGill Pain Questionnaire, Present Pain Intensity scores [12]. In light of recent evidence in FM, it is becoming extremely difficult to ignore the potential impact of FM on LBP, as it is known that no single intervention is superior to the other for management of LBP. The main challenge faced by these two experiments is the implementation of ATM. However, research has consistently shown that there is improvement following FM irrespective of different ATM approaches. Although, research has been carried out regarding FM and LBP and musculoskeletal disorders, no single study explored the potential impact of respiratory characteristics on NS-LBP [13–15].
The present study looked at the potential of ATM sessions to influence respiratory characteristics among participants with NS-LBP as FM has a respiratory mechanism as one of the principles related to efficient use of the neuromusculoskeletal system. Hence, the study hypothesized that inclusion of FM would be advantageous to the LBP participants in ameliorating respiratory parameters.
Materials and methods
Design
The trial was a prospective design with pre-test and post-test evaluation and followed the Consolidated Standards of Reporting Trial statement for Non-pharmacologic treatment [16]. This study received ethics approval from local Research Ethics Committee [600-IRMI (5/1/6)/ REC/256/16], and all participants provided informed consent before entering the study.
Participants
Eligible participants were male or female aged between 18–55 years, diagnosed by the physicians with chronic LBP [17, 18] with the pain intensity of LBP in the range of a minimal pain intensity (2/10 –5/10) by the numeric rating scale (NRS). Participants were excluded if they had any respiratory disease, pregnancy or a history of surgeries to the lumbar spine [7]. The study criteria were based on a recent study used by Mohan et al. (2018) [19]. The study was conducted in a Centre of Physiotherapy at a public university. Initially, leaflets were displayed in the physiotherapy department of the university hospital. Potential patients who approached the researcher were recruited and allocated consequently.
Randomization-sequence generation
Two research assistants that were final year Physiotherapy students who are trained in the protocol were randomly assigned and delivered the protocol; either for the experimental group (EG) or for the control group (CG). Participants were randomly assigned to EG or CG by block randomization using computer randomization method and drawing lots from the concealed envelops. The assessors remained blinded to the treatment conditions throughout the study.
Interventions
The CG received routine physiotherapy using mo-dalities such as infrared rays or interferential therapy or shortwave diathermy, spinal flexion or extension exercises whereas the EG received a predesigned exercise protocol along with routine physiotherapy (Appendix 1).
Both groups received treatment for a period of 8 weeks. The participants in both groups were ins-tructed to carry out the exercises 3 days per week. Once a week, the training was supervised by a research assistant, and the exercises were progressed based on the patient’s level of pain. If the level of pain remained the same or reduced then the exercise was progressed. If the patient was unable to maintain the lumbar stability with a pressure of+/- 10 mmHg using a pressure biofeedback device (PBU), the exercise was not progressed.
Outcomes
The primary outcomes were the respiratory muscle strength variables: maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP), maximum voluntary ventilation (MVV) for measuring respiratory muscle endurance [19]. Secondary outcome measures were Total Faulty Breathing Scale (TFBS) for assessing faulty breathing pattern [20], Cloth Tape Measure (CTM) for measuring chest expansion at the level of axilla, 4th Intercostal space and xiphoid [21], NRS for measuring pain level and PBU for core stability [19, 22]. The stability was tested using 7 levels (level 1 –level 7) with the participant in supine lying with knees bent and feet flat on the floor, and the levels of testing were described in previous literature [22]. The measurement procedures for all the outcome measures were based on the procedures used by Mohan et al. 2018 [19]. The reliability measures of TFBS and CTM were established in earlier studies [20, 21]. All the outcome measures were evaluated at baseline and after 8 weeks of treatment by a blinded assessor.
Sample size
MIP which is considered as one of the primary outcomes in the study was used to calculate the sample size using the G*power program 3.1.0 for two tails, paired test. The mean and standard deviation (SD) of MIP were taken from an earlier study for sample size estimation [7]. The estimated sample to obtain a power of minimum 80% at a significant alpha level of 95% required a total of 34 participants. Therefore, at least 17 participants with NS-LBP were in both EG and CG to identify a difference between the two interventions. However, to account for the possibility of drop-out during the therapeutic treatment program, 10% of the sample size was added, therefore at least 20 participants per group were included in this study.
Statistical methods
The data was analysed using SPSS statistical software, version 20.0. The measurement variables were subjected to descriptive and inferential analysis. Description of demographic variables and study variables are presented as mean, standard deviation, frequency and percentage. Results were tested for normal distribution using the Shapiro-wilk test. Demographic details between the groups were tested using Mann-Whitney U-test. Based on the assumption of normality, Wilcoxon signed rank test were used to compare baseline and post intervention of the EG and CG.
Results
A total of 40 participants (n = 40; 8 males, 32 females) were recruited and randomized. EG (n = 20) aged with mean±SD 22.85±2.10 years and CG (n = 20) aged with mean±SD 24.00±2.57 years. The demographic characteristics showed that there were no significant differences in participants details between EG and CG at baseline. This indicates that the participants in both groups had similar characteristics with regard to age, gender and body mass index (BMI) at the start of the study. The clinical background and the results of the baseline and post values were presented in Table 1–Table 4 for primary and secondary variables. Three participants from each group dropped out during the training because unable to meet the required follow-ups (Fig. 1). MVV values were lower in both baseline and post intervention values in CG as compared to EG.
Demographic Details of Participants between Experimental and Control Groups [mean±SD; number (%)]
Demographic Details of Participants between Experimental and Control Groups [mean±SD; number (%)]
Note: No significant differences in participants’ demographics between groups (p > 0.05).
Comparison of the Primary Outcome variables (MVV, MIP, MEP) between Experimental and Control Groups [data represented as mean (95% CI)]
Note: aSignificant change within group (p < 0.05) from pre- to post.
Comparison of the Cloth Tape Measure (CTM) at different levels and Numerical Rating Scale (NRS) between Experimental and Control Groups [data represented as mean (95% CI)]
Note: aSignificant change within group (p < 0.05) from pre- to post.
Comparison of Total Faulty Breathing Scale (TFBS) and lumbo-pelvic core stability using pressure biofeedback device between Experimental and Control Groups [represented as number (%)]
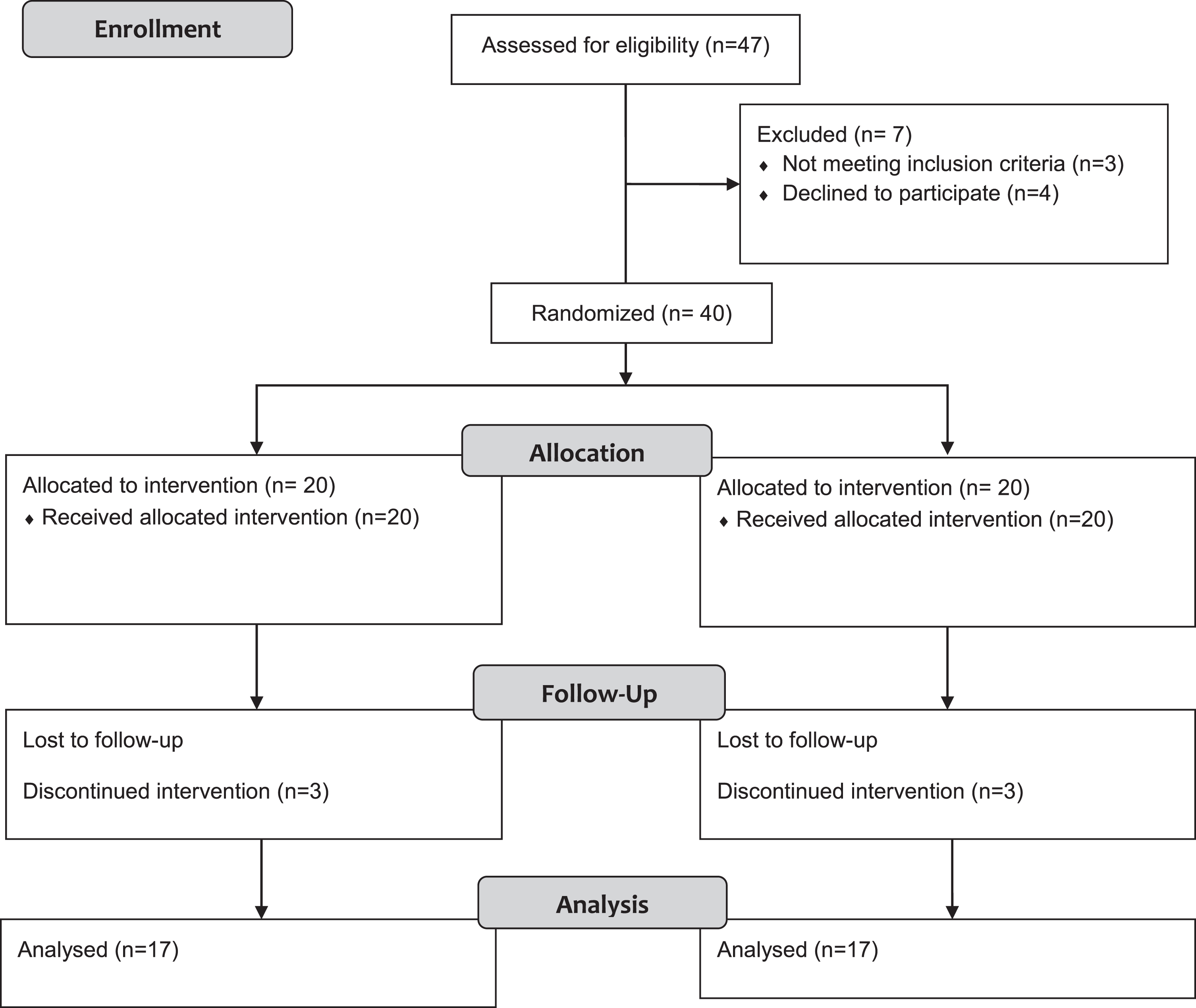
Flow of participants.
There was a significant increase in MIP values from baseline to post intervention (p = 0.004) in the EG. Similarly, with regard to MEP values, there was significant increase in the values (p = 0.001) for the EG. On the other hand, there were no significant changes for the MIP and MEP in the CG. There was no significant increase in MVV scores in the EG from baseline to post intervention (p = 0.367). There was a significant increase in respiratory muscle endurance score in CG (p = 0.005).
Secondary outcome variable
In relation to chest expansion the participants in the EG showed improvement at the level of xiphoid process (p = 0.004) but did not show improvement at the level of the axilla and 4th ICS (p = 0.582, and 0.084, respectively). With regard to the CG, the participants did not show improvement in chest expansion for axilla, 4th ICS and xiphoid (p = 0.480, 0.679, 0.317, respectively).
In relation to NRS values, there was significant reduction in the pain (p = 0.004) for the EG, but there was no reduction in pain for the CG (p = 0.746). TFBS scores did not change for the either EG or the CG (p > 0.05). The scores for the core stability component for the EG (p = 0.001) and for the CG (p = 0.414) showed that there was improvement in lumbo-pelvic stability in the EG alone.
Discussion
This study achieved its aim by improving certain respiratory variables and reducing pain in people with NS-LBP following FM training in EG. Similarly, there were effects on respiratory muscle endurance and on pain among CG exercise training protocols. Specifically, the FM was effective in respiratory muscle strength components, pain and in promoting breathing pattern components. These results corroborate the findings of a great deal of the multifactorial model, a model of movement dysfunction and system-based classification of ‘Puzzle’ model proposed for the relationship between respiratory variables and LBP [8–10]. Therefore, the hypothesis of improving respiratory variables and reducing pain following a predesigned FM was supported.
With regard to respiratory muscle strength, there was improvement in both MIP and MEP following FM exercise sessions as compared to CG exercise sessions. The results of the study cannot be compared with other studies related to FM as this is the first study to use these outcome measures in this manner. Most of the studies are qualitative in nature and the outcome measures used are mostly related to pain and interoceptive awareness [11, 12]. There was also significant improvement in respiratory muscle endurance following CG, that might be due to the type of exercises which was interspersed from the initial exercise session onwards. It is known that the FM promotes respiratory mechanics rather than respiratory muscle endurance [1].
Even though, the results of the study cannot be compared directly with earlier research, the results could be compared with relation to respiratory muscle strength. Firstly, trunk stabilizing functions of diaphragm which could have been achieved by promoting symmetry through FM sessions. Secondly, it is assumed that suboptimal position of diaphragm would have been improved because of FM. Potential future studies could explore if there is an association between diaphragm position and the development and recurrence of LBP.
The reason behind including pain and lumbo-pelvic instability as one of the outcome measures is, pain can alter an individual’s breathing pattern and lumbo-pelvic instability leading to low back pain. The EG reported a greater decrease in pain score compared to the CG. This indicates that the present study results with relation to pain score was supportive of the hypothesis that FM could alter pain through increased body awareness and symmetrical postural alignment [1]. Physiologically, FM is believed to stimulate the neuro-plastic properties of the nervous system. This could have reduced pain through exploration of normal movement, improving a person’s neuro-muscular self-image through sensory-motor awareness [1]. In addition, it could be argued, FM might have an impact on descending pain control pathways, may utilise several neurotransmitters in their interaction with the dorsal horn cell pain transmission neurons contributing to a reduction in pain. Fear avoidance that could reduce movement because of an emotional component of pain would have been mitigated through mindful learning of FM [12]. These skills might have helped in organizing the body to transfer to other forms of mental activity there by reducing pain.
There were changes in xiphoid level chest expansion following FM lessons, but there were no changes in any of the levels of chest expansion in the CG. There was also improvement in breathing pattern from moderate to mild following EG interventions as measured by the TFBS.
The changes in breathing pattern and chest expansion would have happened because of emphasis on the body through mindfulness, which is not being considered in their image of movement [12]. In addition, the respiratory mechanics, which are promoted through efficient use of neuro-musculoskeletal system would have facilitated an appropriate breathing pattern and improved chest expansion [4]. The brain becomes aware of using a symmetrical breathing pattern through neuroplasticity as a result of mindfulness and body awareness following FM.
The significant changes in lumbo-pelvic core stability were observed in FM lesson group alone, and this was not observed in the routine physiotherapy exercise group. A total of three participants were in level 5 in EG, whereas only one participant achieved level 5 in CG. This signifies lumbo-pelvic stability improved through proper positioning and alignment following FM training sessions.
Limitations
The findings of the study could be viewed in light of a few limitations. First, no long-term follow-up tests was conducted which could establish longer-terms effects of the intervention. Second, most of the participants were younger females which could limit external validity of the findings. Thirdly, the participants had mild-moderate pain intensity, and this data might not be applicable for those participants with severe pain. In addition, the study did not consider data imputation technique for the dropped-out participants, and there was a significant difference in baseline value between the group which need to be interpreted carefully while interpreting the study results.
Conclusions
FM technique is suggested to be a potential additional exercise for participants with LBP which could improve respiratory, pain and lumbo-pelvic stability components. Further research is needed to compare FM with other forms of physiotherapy exercises in order to clarify their effects, and the potential of combination of exercises with FM in treating LBP.
Footnotes
Appendix 1 - Feldenkrais Method Training Protocols
When the heels are pointing to the left and the right leg needs to roll onto its inner edge, and draw up the knee towards the abdomen. Then let it straighten again. Do the exercise for several times and then rest.
For each and every exercise the participants are supposed to stand up easily, walk around a bit, and feel comfortable.
All the above mastered techniques were carried out together for a period of 1 hour with rest periods in between the exercise program.
There was one session per week, which were supervised for 1 hour for 8 consecutive weeks and the subjects were instructed to perform the exercises 3 days in a week. Each exercise was progressed until 5 weeks and for the last three weeks the whole set of exercises was given.
Acknowledgments
The authors would like to thank the study participants who participated in this study and Dr. Kathyrn Collins, Bournemouth University, who spent her valuable time in editing and proofreading the manuscript.