
Abstract
BACKGROUND:
The relationship between physical function and the development of complications in people after abdominal surgery is not well known. The objective of this study was to prospectively examine the relationship between simple physical functioning tests and complications following abdominal surgery.
METHODS:
Participants were recruited from an elective surgery waiting list. The following variables were measured pre-surgery; functional capacity (Six Minute Walk Test, 30 Second Sit to Stand Test), grip strength (hand dynamometer), self-report physical activity [International Physical Activity Questionnaire, (IPAQ)]. At 30 and 60 days post-operatively IPAQ and self-reported recovery were collected by telephone. Data related to complications and length of stay was extracted from the medical chart.
RESULTS:
Forty-nine participants (25M/18F) were recruited with a mean (SD) age of 59.5 (14.7) years. The complication rate was 41.9% (n = 18). Factors which differed between the complications and no complications groups were; longer operating time (p = 0.05),>2 co-morbidities (p = 0.033), body mass index >30 (p = 0.005), lower activity levels (p = 0.02), VO2 Peak (p = 0.017) and 6-minute walk distance (p = 0.019). There was an increased length of stay (p < 0.001) and sedentary time (p = 0.007) in the complications group. Activity levels reduced in the whole group (p < 0.001) even though self-report physical activity and recovery were high.
CONCLUSION:
A number of potentially modifiable physical functioning factors differed in the complication versus no complication groups. Future studies should evaluate whether optimizing physical functioning pre-operatively could alter complication rates and recovery in patients undergoing abdominal surgery.
Background
Previously, abdominal surgery was mostly open surgery. In recent decades, there has been a paradigm shift towards more minimally invasive techniques such as closed and laparoscopic techniques [1] which are generally associated with a lower rate of complications [2].
Lowering the rate of complications is an important therapeutic target in abdominal surgery as complications can result in significant and costly mental and physical sequelae [3–5]. Known factors associated with complications include age, body mass index (BMI)>25, open surgical approach, multiple co-morbidities, high American Society of Anesthe-siologists (ASA) scores and poorer physical function [6–10]. The World Health Organization (WHO) ICF framework [11] defines functioning as an all-encompassing term for the interaction between three explicit constructs: body function and structure (physiological and anatomical structure of the body systems), activities (execution of a specific task within a standardized environment), and participation (involvement in everyday life situations). Mapped to the ICF framework, elements of physical functioning such as strength can be assessed as an element of body function and physical tests such as sit to stand and assessment of mobility can be assessed under activities and participation.
Cardiopulmonary exercise testing (CPET) can be a useful risk assessment tool but may be unavailable due to cost and specificity of skills needed to conduct this type of testing [12]. In addition, the maximal nature of CPET testing precludes some from this form of testing. Viable alternatives to CPET testing which may help guide whether complications develop or not have yet to be identified [13].
In recent times, surgical outcomes have broadened from hard outcomes such as complication rate and cost to the more nebulous multidimensional construct of ‘quality of recovery’ [14]. The relationship between simple, easily conducted, low cost, submaximal tests that mimic common daily functions (walking, standing, gripping etc.) and complications in abdominal surgery patients is not well known. The relationship between patient reported physical recovery - a likely indicator of quality of recovery and complications has also not been established.
The primary aim of the study was to prospectively examine the relationship between simple physical functioning tests and complications following abdominal surgery in a real world setting. A secondary objective was to evaluate physical function performance differences in patients undergoing abdominal surgeries (colorectal, cholecystectomies & hernia repairs) between those who develop complications and those who do not and determine their impact on physical recovery.
Methodology
In this prospective cohort study a real world ap-proach was used; the study was based around routine care pathways, aiming to enhance study adherence and include participants who were truly representative of an abdominal surgery population [14]. The study took place at the pre-operative assessment unit and surgical wards of a model 4 acute hospital which is a specialist cancer centre between September 2016 and July 2017. Ethical approval was gained from the HSE Mid-Western Regional Hospital Ethics Committee and study procedures were in accordance with the Declaration of Helsinki.
Study procedure
The lead study investigator (M.F.) accessed the waiting list for elective surgeries and performed a preliminary eligibility screen based on medical chart details. A list of highlighted potential participants for study inclusion was given to pre-operative unit nursing staff who routinely phoned patients to arrange the pre-operative visit. During this phone call, the nursing staff briefly mentioned the study to those pre-identified. If they were agreeable it was explained that a physiotherapist (M.F.) would follow up with a phone call to explain the study further. The study investigator (M.F.) then telephoned the potential participant and explained the study in greater detail and asked if they would like further information. Those agreeable to receiving further information were posted a participant information leaflet and a consent form at least 7 days before their appointment date. Those who had received this phone call were approached by M.F. at the pre-operative clinic and if they definitively met all eligibility criteria and were agreeable to study participation a consent form was then completed. Data collection then proceeded in the pre-operative assessment clinic alongside their routine pre-operative assessment.
Inclusion and exclusion criteria
The inclusion criteria were as follows; (i) written consent to participate in the study, (ii) eighteen years or above, (iii) planned for elective abdominal surgery (defined as any surgery that breaches the abdominal wall to include laparoscopic, laparoscopic assisted and open surgeries) and (iv) ASA score <4. The exclusion criteria were as follows; (i) previous abdominal surgery within one year prior to study entry, (ii) unable or unwilling to give informed consent, (iii) inability (cognitive) to perform the pre-operative tests, as characterised by inability to understand the information in the patient information leaflet, (iv) current systemic acute illness (v) scheduled for non-abdominal surgery (vi) unstable angina or myocardial infarction in the previous month, (vii) physical limitation precluding inability to participate in pre-operative tests.
Test battery
The following pre-operative test battery was collected by M.F. Demographics collected included the following; age, sex, co-morbidities, smoking status, weight (kg), height (cm) and BMI (kg/m2). Height was using a SECA 213 –portable height measure and weight was measured using the SECA 876 digital scales. Co-morbidities were scored using the Charlston Co-morbidity Index [15]. Spirometry was performed to obtain vital capacity (VC), forced vital capacity (FVC), forced expiratory pressure in one second (FEV1), FEV1/FVC ratio and peak expiratory flow rate (PEFR). Reliability was ensured via a standardised approach [16] using the Vitalograph Model 2120 Hand Held REF 79XXX. Peak cough flow was performed by attaching a naso-oral mask to a peak flow meter (Mini- Wright Peak Flow Meter, Clement Clarke International). Participants were requested to inhale maximally, in a seated position, prior to placing the mask over their nose and mouth, and coughing forcefully. This was repeated three times to give numerical scores. The highest score was recorded [17]. The six-minute walk test was performed as per the ATS guidelines 2002 [18]. Predicted distance was calculated against normative data based on age, sex, weight and height [19]. Peak oxygen uptake (VO2Peak) was also calculated [20]. The thirty second sit to stand test was performed by asking participants to go from a seated to standing position and vice versa, as many times as possible in thirty seconds, without the use of their hands to assist. The same standard height chair (17 inches) was used [21]. Grip strength was recorded, using a Baseline hydraulic hand held dynamometer. Participants were asked to squeeze the dynamometer maximally for a period of 3 seconds, the result was recorded and the test repeated twice more. An average of the three scores was recorded in pounds (lbs). Self-reported physical activity data was collected by the researcher using the short form International Physical Activity Questionnaire (IPAQ) which is a self-reported measure of activity levels in the previous seven days [22]. MET minutes per week were calculated using the scoring protocol [23]. ASA score [24] and surgical grade was determined by the assessing Anaesthetist. Nutritional status was assessed using the Malnutrition Universal Screening Tool (MUST) [25]. This screening tool is based on BMI score, weight loss score and acute disease effect score.
Postoperatively, the researcher collected the following data from the medical charts, on the day of hospital discharge: type of surgery and incision type, date of surgery, length of stay, initial twenty four hour post-operative analgesia, morbidity and mortality. The Clavien-Dindo Classification was used to categorise the various complications into grades, which has been proven to be reliable [3]. Perioperative or postoperative complications, re-excisions, repeat surgeries, were recorded from the medical chart on the day of discharge. Re-excisions and re-operations were regarded as within 6 weeks from the initial surgery, including re-admission as a result of complications.
Participants were then contacted by phone by M.F. 30 and 60 days postoperatively and questioned in relation to the following: complications post discharge, telephone IPAQ and percentage of physical recovery ranging from 0–100% [26]. This research study was reported in line with STROCSS criteria [27].
Statistical analysis
Descriptive data was reported using percentages and numbers. Data was analysed for normality using the one sample Kolmogrov-Smirnov test. Mean (SD) was used to summarise parametrically distributed data and median (IQR) used to summarise non-parametrically distributed data. Mann Whitney U tests were used to evaluate non-parametric data and Independent T tests were used as the parametric alternative. These were used when variables were split into groups based on the presence or not of complications. Relationships over time were analysed using the Wilcoxon Signed Rank Test when analysing activity, inactivity and recovery. Data was analysed using IBM SPSS© version 24 and results were deemed significant if P ≤ 0.05 in all cases.
Results
One hundred and ninety-two people were screened for study participation between September 2016 and June 2017. Of these, 49 were assessed and 43 underwent related surgical procedures. From study entry, no participants were lost to follow up. A flow chart of participants through the study is shown in Fig. 1.
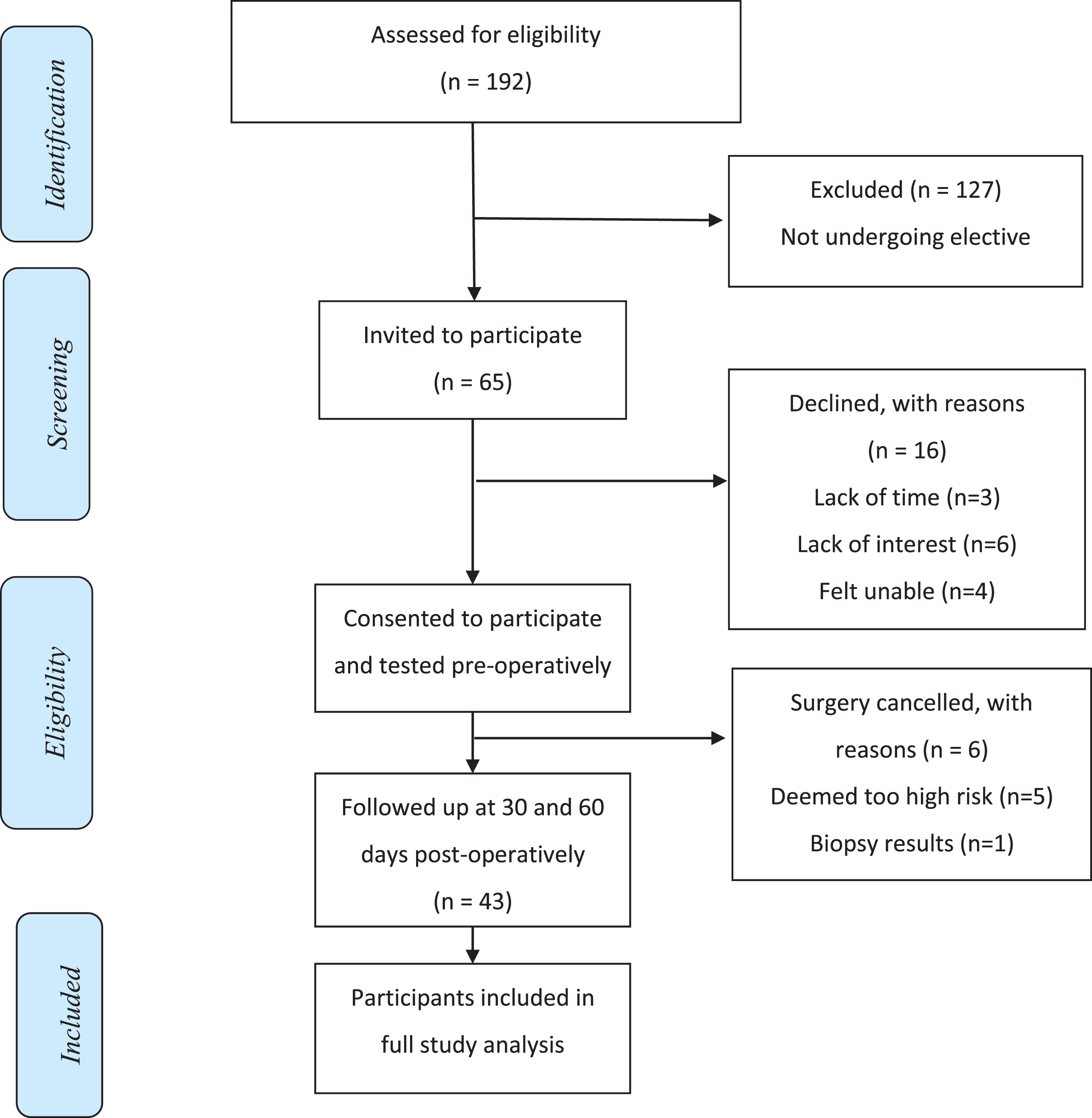
Flow diagram of participants through the study.
Eighteen females (41.9%) and 25 males (58.1%) participated in this study. Smokers accounted for 11.6% (n = 5) of study participants. Thirty-three (76.7%) participants had at least one or more comorbidities according to the Charleston Comorbidity Index with a median (IQR 25–75) score of 3 (1,5). The mean (SD) age of participants was 59.5 (14.7) years with a range of 29–79 years. Mean (SD) BMI was 29 kg/m2 (5) and nutritional status was generally very good with only five participants (11.7%) entering into the medium-high risk category as per the MUST score.
Mean recorded weekly MET minutes were 2618 (3209) which equates to a mean of 6.23 MET hours in activity, on a daily basis. Mean weekly sitting was 2045 (1116.14) minutes which equated to 4.9 hours sitting daily. A total of 19 surgeries were performed, which broadly fell into the categories of: colostomy/ileostomy reversals (n = 7, 16.3%), hernia repairs (n = 10, 23.3%), colorectal surgery (n = 21, 48.4%) and cholecystectomies (n = 5, 11.6%).
Rate of complications
The complication rate pre-discharge was 41.9% (n = 18). This corresponded to 30.2% (n = 13) at 1 month and 21% (n = 9) at the 2-month time point post-surgery. At 30 days postoperative, 3 more participants had developed complications after their discharge. This resulted in an overall complications prevalence of 48.8% (n = 21). Six participants were readmitted which resulted in an additional 38 nights hospital care. There were no reported cases of mortality. A total of 34 various complication types were recorded with a breakdown of 21 (64.8%) medical and 13 (35.2%) surgical complications. These ranged from relatively minor such as cellulitis to respiratory failure requiring intensive care admission.
Main findings
A number of patient-related variables (Table 1), physical functioning variables (Table 2) and surgical-related variables (Table 3) differed when participants were divided dichotomously into those who developed complications and those who did not.
Patient-Related Variables and Spirometry separated by presence or absence of postoperative complications
Patient-Related Variables and Spirometry separated by presence or absence of postoperative complications
*P≤0.05 was deemed significant in Mann Whitney U Test/Independent T test, all data presented as mean and SD unless otherwise stated. SD; standard deviation, BMI; body mass index, VC; vital capacity, FVC; forced vital capacity, FEV1; forced expiratory volume in 1 second, PEFR; peak expiratory flow rate, PCF; peak cough flow.
Physical Functioning variables and self-report recovery separated by presence or absence of postoperative complications
*P≤0.05 was deemed significant in Mann Whitney U/Independent T tests, all data presented as mean and SD unless otherwise stated. SD; standard deviation, 6MWT; 6 minute walk test, VO2 Peak; peak oxygen uptake, MET; metabolic equivalent.
Surgery related variables separated by presence or absence of postoperative complications
*P≤0.05 was deemed significant in Mann Whitney U Test/Independent T tests, all data presented as mean and SD unless otherwise stated. SD; standard deviation.
Preoperatively, BMI was greater in the complications group compared to the no complications group (p = 0.005). Co-morbidities were also higher (p = 0.033) in the complications group versus the no complications group. Weekly MET minutes pre-surgery were lower in the complications group compared to the no complication group (p = 0.02) and higher physical functional capacity was shown in favour of the no complications group (p = 0.017).
Pre-discharge findings included the following. Operating time was significantly different between groups (p = 0.05), [median (IQR) of 142.5(105, 245) minutes in the complications group versus a median (IRQ) of 90 (60, 180) minutes in the non- complication group]. A significant difference was found between the groups in relation to LOS and complications (p < 0.0001). LOS increased from a median (IRQ) of 2 (1, 4.5) nights in those without complications to a median (IRQ) of 8.5 (7, 14.2) nights in those who did experience complications. Complications also caused 6 readmissions which resulted in an extra 38 nights hospital care.
At 30 days postoperative results significant differences were observed between groups in relation to self-perceived physically recovery (p = 0.008) in favour of the no complications group.
At 60 days post operatively, significant differences were observed in weekly MET minutes between groups (p = 0.02). Significant differences were apparent between groups in relation to weekly sitting minutes at 60 days post-surgery (p = 0.03) also, in favour of the no complications group.
Figures 2 and 3 show changes in physical activity levels from preoperative assessment to 60 days postoperative. A significant reduction in activity was seen for the total group from pre-surgery to 60 days post-surgery (p < 0.001) with 69.8% of people not returned to baseline activity levels by 60 days. Both groups showed significant reductions in activity levels with the complications group achieving 31.8% (p = 0.009) of baseline reported activity and the non-complications groups achieving 58.6% (p = 0.002). In relation to sitting time, the complications group reported sitting 55% longer than baseline figures (p = 0.007). No significant differences were found in relation to age, spirometry, peak cough flow, sit to stand and dynamometry.
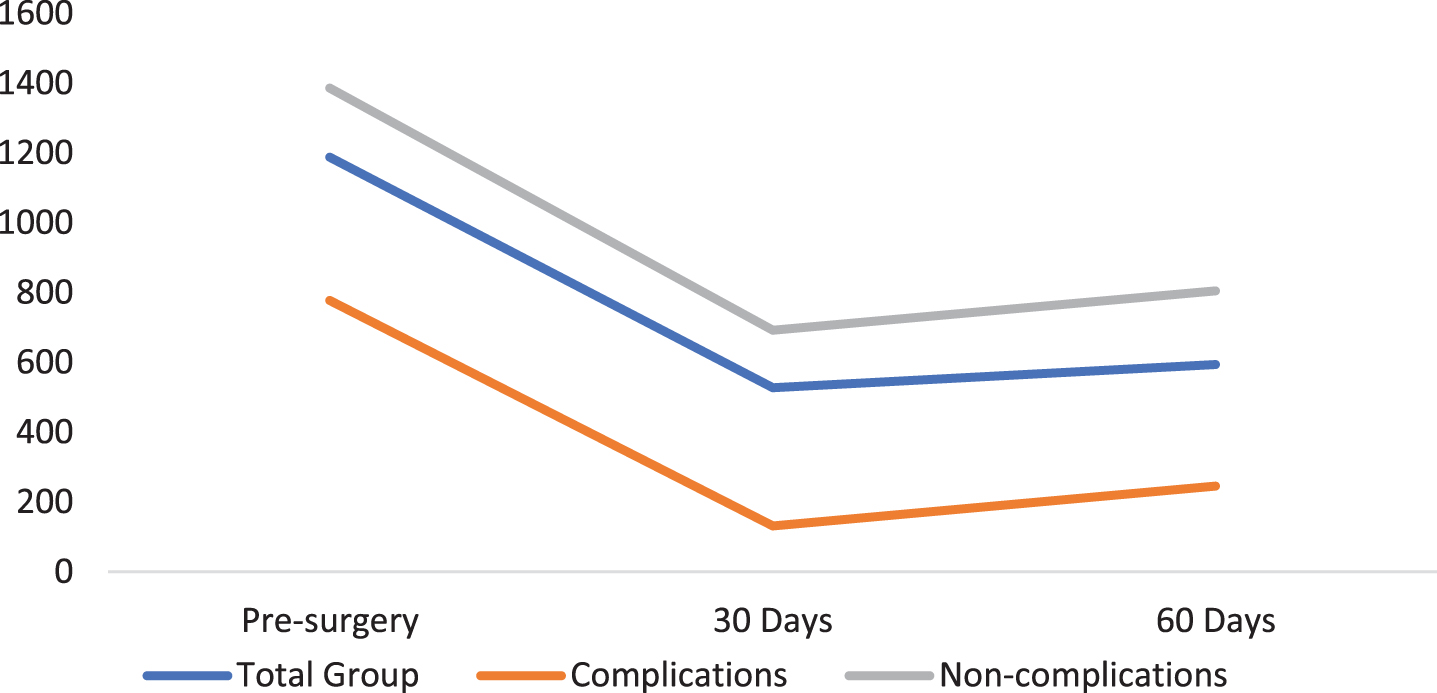
Weekly MET-minutes at all-time points, total (n = 43), complications (n = 18) & non-complications groups (n = 25).
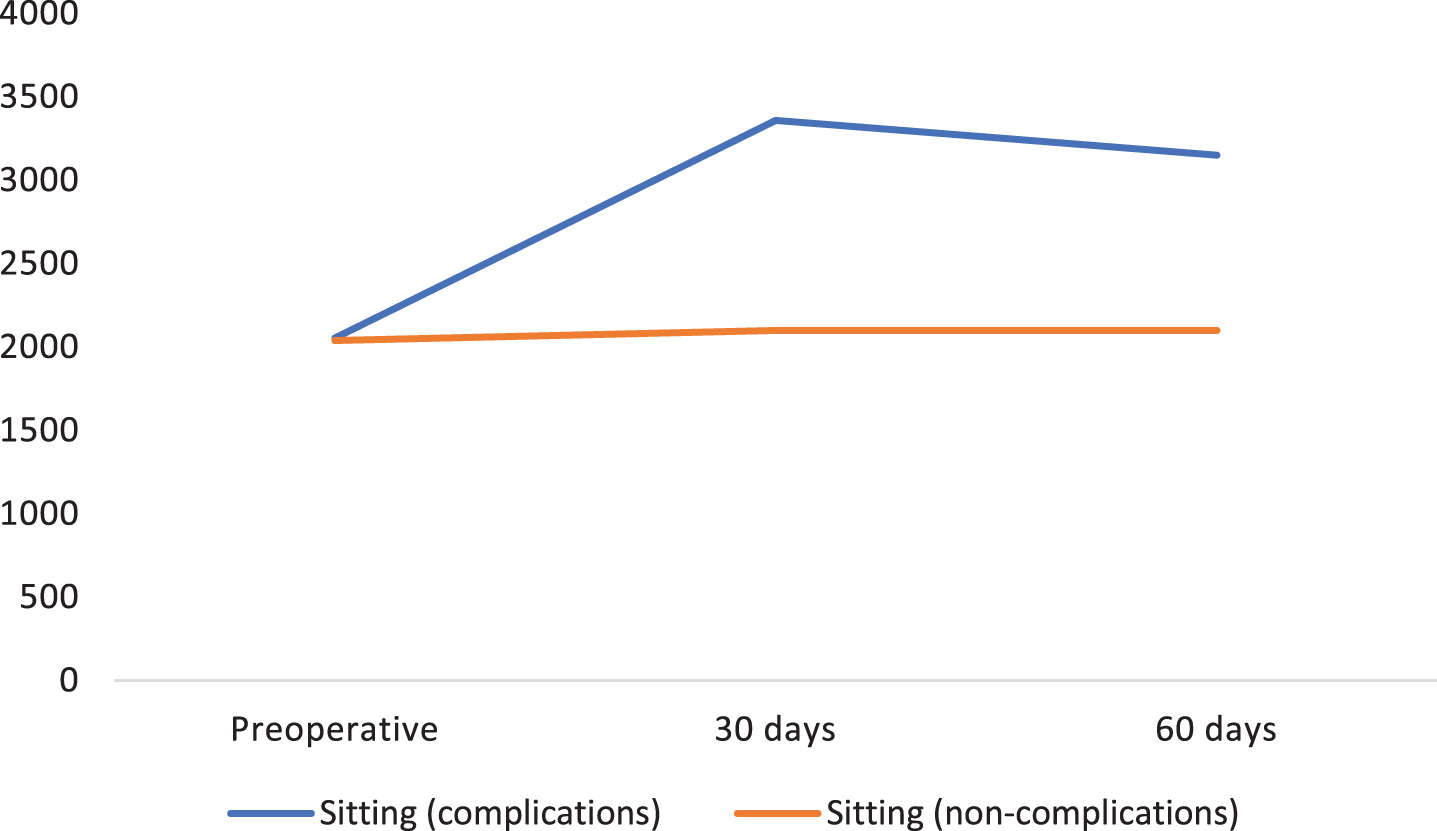
Weekly sitting (mins) –All time points (Complications (n = 18) vs Non-complications (n = 25)).
The main finding of interest was the divergence in physical functioning variables between those who developed complications and those who did not in a sample undergoing abdominal surgery in a real-life clinical setting.
The following physical function differences emerged between the complications and no complications groups; preoperative walking distance, VO2Peak, self-reported physical activity and sedentary time. Non-physical function differences which emerged between the groups were BMI >30, co-morbidities and longer surgical procedures.
In relation to the 6MWT distance the following cut off points as risk factors for post-operative pulmonary complications (PPCs) have been previously reported;<300 m as associated with morbidity [28] and <325 m as associated with PPC’s [29]. The findings of this study show a median of 490 m in the complications group which points to a possibly higher threshold than previously thought in terms of risk of post-operative complications.
The complication rate reported here of 48.8% (n = 21) is comparable to previous studies [30, 31]. BMI as a risk factor for PPCs has been previously reported with a BMI of >25 kg/m2 shown to be associated with an increased the risk of complications [7, 32]. The presence of preoperative comorbidities as a risk factor for complication development shown in the present study is supported by previous research in this area [4, 35]. Our findings build on previous studies associating high BMI and co-morbidities with complications.
In relation to the impact of complications, our results showed LOS increased from a median (IRQ) of 2 (1, 4.5) nights in those without complications to a median (IRQ) of 8.5 (7, 14.2) nights in those who did experience complications which is similar to previous findings which showed an almost 80% increase in LOS caused by complications [30]. The reduction in activity levels also adds to the findings of previous studies [25, 35].
Recovery can be considered as a returning to pre-surgery levels or better [36]. The relationship between recovery and physical variables such as physical activity and physical functioning are not well known [26]. In the present study the no complications group reported near full self-reported physical recovery by 60 days’ post-surgery, but their activity levels remained significantly lower than baseline, with very minimal changes in their sedentary time from pre-operative levels to 60 days post-operatively. This finding is supported by a previous study [26] that also found no relationship between preoperative physical activity and subjective self-recovery measurements. Similarly, a recent study [37] in a population of critical care survivors, high levels of physical recovery were reported but variables such as frailty and physical function lagged behind. The discrepancy between self-reported physical recovery and physical-focussed variables highlights the complexity of this multi-dimensional construct [38].
Perhaps due to the sedentary nature of most people’s lifestyles [39] it is possible to ‘feel’ physically recovered without returning to own baseline levels of physical activity. In any case an implication is that even when patients ‘feel’ or perceive to be physically recovered there is a lag time between ‘feeling’ recovered and return to own premorbid level of physical activity. It is also possible that memory of physical ability is somewhat unreliable [40] and self-scoring of percentage recovery is somewhat arbitrary and may be inherently difficult. Expectations of recovery are highly individualised [36] and not well known. In any case, with only 30% of participants achieving baseline levels of physical activity by 60 days post-operatively, it would appear that the majority are still, perhaps unknowingly, restricting their activity levels. Given the low-cost and associated risks, it would appear well advised for clinicians to reinforce the physical activity message to patients at all pre and post-operative time-points. Possible rehabilitation needs of this cohort also deserves consideration in future studies.
Possible limitations of this study were that participants self-elected to participate in the study, and so the study sample may be representative of a more functionally independent population. Also the severity of complications was not reflected in the analysis. Participants who underwent colorectal surgeries were involved in the enhanced recovery after surgery protocol (ERAS), however this factor was not evaluated specifically in this study and may have influenced complications and recovery patterns, although we have no reason to believe clinical pathways in this centre are different to other centres. We employed a self-report measure of physical activity which was convenient for use in this setting, although the tendency for over-estimation and self-report bias [40] must be acknowledged. A further limitation was the inability to perform a power calculation due to the lack of research in the area, therefore the application of inferential statistics may not have been suitable. The lack of power may have been the reason a clear difference was not shown between the complications (median age 71 years) and non-complications (60 years) groups, although it has been suggested that physiological age may be more useful than chronological age as a predictor of complications in major abdominal surgery [35] which may partly explain our results. We also did not account for the possible effect of multiple testing and due to the study design causality could not be assumed. Notwithstanding these limitations, strengths of the study included 100% participant retention likely due in part to the “real world” approach. This study has also shown the usefulness of some low cost, fast, psychometrically strong physical function tests which have good clinical utility and could be easily replicated.
Comparing the physical functioning tests outlined in this study to CPET would be a useful next step to establish the criterion validity of these measures. Recovery should be examined at multiple time points in future studies, both qualitatively and quantitatively to account for a possible dichotomy in patient and clinician views and to accurately map recovery trajectories.
Conclusion
This study highlighted a divergence in general patient characteristics as well as physical functioning variables between participants who developed complications versus those who did not. Objectively measured physical recovery was suboptimal even though self-assessed levels of recovery were high. This study indicates that simple low-cost physical functioning testing may be useful prognostically but this requires further exploration.
Longitudinal analyses with multiple time-points should be conducted to map the recovery trajectory after abdominal surgeries and future studies would elucidate if short term optimisation of physical functioning pre-operatively could result in lower complication rates.