
Abstract
BACKGROUND:
Functional mobility requires an ability to adapt to environmental factors together with an ability to execute a secondary task simultaneously while walking. A complex dual-tasking gait test may provide an indication of functional ability and falls risk among community-dwelling older adults.
PURPOSE:
The aim of this cross-sectional study is to investigate age-related differences in dual-tasking ability and to evaluate whether dual-tasking ability is related to executive function.
METHODS:
Forty-one community-dwelling healthy older and forty-one younger adults completed a dual-tasking assessment in which concurrent tasks were incorporated into the Functional Gait Assessment (FGA). The manual dual-task involved carrying a glass of water (FGA-M) while the cognitive dual-tasks involved numeracy (FGA-N) and literacy (FGA-L) related tasks. FGA scores under single (FGA-S) and dual-task conditions together with associated dual-task costs and response accuracy were determined. Executive function was assessed using The Behavioural Assessment of the Dysexecutive Syndrome (BADS).
RESULTS:
FGA-N and FGA-L scores were adversely affected in both groups compared to FGA-S (p≤0.001). However, score reductions and dual-task costs were significantly greater for older adults compared to younger adults on FGA-N (p≤0.05) and FGA-L (p≤0.001), with older adult performance on FGA-N associated with falls risk (p≤0.05). Executive function did not appear to be related to dual-tasking ability.
CONCLUSION:
Findings suggest that cognitively demanding tasks while walking, have a deleterious effect on dynamic balance and could place older adults at a greater risk of falls.
Introduction
Effective, safe gait is essential for independence and longevity among eldery adults [1]. Postural control, fundamental to a person’s ability to stand and walk independently, requires sensorimotor processes [2], with the integration of afferent information from many musculoskeletal and neural systems including vestibular, the visual and somatosensory systems [3, 4]. Furthermore, this complex motor skill utilises cognitive function, in the form of two intimately linked domains, attention and executive function [5] and hence, is no longer considered an automatic task. In a seminal study, Lundin-Olsson, Nyberg [6] illustrated the attentional demands of gait since those who ‘stopped walking when talking’ were more likely to fall in the future. Considerable work has demonstrated the value of executive functioning in complex gait situations [7, 8], that are representative of routine environmental challenges. When walking under divided attention conditions, executive function plays an important role in allocating attentional resources, ensuring successful completion of a given task. The importance of executive function becomes more apparent as the difficulty of the secondary task increases [9], which may even expose gait instability among healthy subjects.
Various studies have illustrated that both healthy young and older adults walk slower while performing a secondary task [5]. Older healthy adults not only reduce gait speed but also become less stable with increased gait variability when dual tasking [8] and this is associated with an increased future falls risk [10]. With aging, gait loses automaticity, placing greater demands on declining frontal-dependent executive control resources [11, 12]
Functional community mobility requires an ability to perform a secondary task simultaneously while walking, and to adapt to external environmental factors. The aim of the dual-task gait assessment is to compare task performance while walking and concurrently completing an attention-demanding task, to baseline performance of either one of the individual tasks [13]. Deficits in performance while dual-tasking, referred to as dual-task costs (DTCs) [14], are thought to represent interference as both tasks compete for brain cortical resources. Therefore, if information processing is limited, it may be important to prioritise one task over the other. The posture first strategy, originally proposed by Shumway-Cook et al. [15], suggests that when dual-tasking, postural control will be favoured over the execution of a secondary task, to prevent a loss of balance.
Much of the dual-task interference related research utilises spatiotemporal gait parameters as outcome measures, which often require sophisticated equipment and a laboratory and therefore may lack clinical utility [8, 16]. A possible exception to this is gait speed, however such a one dimensional measure cannot adequately capture the multidimensional nature of gait [17]. This may partly explain its insufficient sensitivity [18] with Menant et al. [19] concluding that dual-tasking tests of gait speed did not demonstrate a superior predictive ability for falls over single task tests.
The Functional Gait Assessment (FGA) is an easy to administer, reliable and valid gait assessment tool requiring minimal space or equipment [20]. Currently, dual-task protocols do not sufficiently assess the skills necessary for everyday functional mobility. Complex gait tests such as a dual-tasking FGA, which evaluate a range of clinical gait activities, may be a better tool to investigate age-related differences in dual-tasking ability. Such an assessment tool could also serve to partly address the standardisation concerns, which have prevented the development of evidence-based recommendations for clinical practice. Therefore, the main objective of this cross-sectional study was to compare dual-tasking ability on the FGA between healthy older and younger adults, with this information relevant for future dual-task assessment and intervention protocols. A secondary aim was to assess the relationship between dual-tasking performance on the FGA and executive function. It was hypothesised that dual-tasking would interfere with postural stability, presenting a greater challenge to healthy older adults, and that these dual-tasking effects on this complex gait test would be related to executive function.
Materials and methods
Participants
A convenience sample of independently mobile, community-dwelling younger (n = 41, Male = 19; mean age = 37 years, range = 23 –58) and older adults (n = 41, Male = 18; mean age = 68.3, range = 60 –88) were recruited from the university and community via flyers and word of mouth. Participants were included if they were between 18 and 90 years, and able to ambulate without an assistive device.
Those aged 60 and older were considered older adults. Subjects were excluded if they reported history of falling within the previous 6 months, dementia, as evidenced by a diagnosis of dementia, an unstable medical condition or pathology likely to directly impact on gait (e.g. visual, neurologic, vestibular, orthopaedic).
Protocol
The study was reviewed and approved by the National Hospital for Neurology and Neurosurgery and Institute of Neurology Joint Ethics Committee and that the procedures followed during the study were in accordance with the Helsinki Declaration of 1975, as revised in 1983.
Each participant completed the following assessments: Behavioural Assessment of the Dysexecutive Syndrome (BADS) test: an ecologically valid and reliable battery comprising of six sub-tests, which evaluate a range of executive function constructs [21]. The six sub-tests include:(1) Rule shift cards; to evaluate cognitive flexibility (2) Action program; to assess ability to identify and implement a solution to a practical problem. (3) Key search; test assesses ability to plan a strategy to solve a problem (4) Temporal judgment; involves judgment and abstract thinking (5) Zoo map; to assess spontaneous planning abilities, and (6) Modified six elements; to assess the ability to plan, organise and monitor behaviour. Timed Up and Go test (TUG): a reliable and valid dynamic test which involves standing up from chair (approximate seat height 46cm), walking three metres at normal pace, turning around and walking back to the chair, sitting back down again [22]. A cut-off score of 13.5 suggests an increased falls risk in community dwelling older adults, with a higher specificity than sensitivity reported in the literature [23]. FGA: a reliable and valid [20] standardised measure of functional gait, which is scored on a 4-level (0–3) ordinal scale with a maximum score of 30 achievable; a cutoff score of 22/30 predicts falls in community dwelling older adults [24]. FGA was performed under single and dual-task conditions (Table 1).
Functional Gait Assessment (FGA) Dual Task Conditions
Abbreviations: FGA-M, Functional Gait Assessment manual task; FGA-N, Functional Gait Assessment numeracy task; FGA-L, Functional Gait Assessment literacy task.
To reduce potential practice or learning effects from trial to trial, a different letter or number was used across successive trials. The responses were recorded using a recorder and scored following the testing session according to the total number of responses and number of errors made. Since all measures were completed in one session, rests were suggested at various stages in between testing during the session, to help minimize the effect of fatigue. No instruction on task prioritisation was communicated.
Data analysis was undertaken using the Statistical Package for the Social Sciences Version (SPSS) 22.0 (IBM Corporation, Chicago, IL). A level of significance of p≤0.05 was set for this study. Normality of the continuous variables was tested with the Shapiro-Wilk test and appropriate descriptive statistics were calculated. Where the normality assumption was violated, equivalent non-parametric tests were used. Independent-samples t-test was performed to assess between-group differences in the TUG score with data reported as mean±SD. The Mann Whitney U test was utilised to evaluate between-group differences in FGA scores and BADS scores. Median and inter-quartile values (Q1 –Q3) are presented. Given the non-normal distribution these values are better represented by the median rather than the mean, with the median less sensitive to outliers [25]. A Chi-Squared test was performed to evaluate the distribution of BADS overall classification.
Dual-task costs (DTCs), characterised as the percentage change difference in performance relative to the single-task performance was calculated for all three tasks (FGA-M, FGA-N and FGA-L) using the following equation:
All DTCs were classified such that a negative value signified a performance decrement and a positive value illustrated a dual-task benefit. Between-group DTC differences were evaluated using the Mann-Whitney test.
Response accuracy was assessed under the two dual-task conditions, FGA-N and FGA-L, utilising the following equation:
Spearman’s rank correlations investigated whether BADS scores were correlated with DTCs or FGA scores under the different dual-task conditions.
Results
FGA score
Both FGA-N (z = –2.76, p≤0.05, r = 0.30) and FGA-L (z = –3.23, p≤0.001, r = 0.36) scores were significantly lower in the older compared to the younger group (Table 2). There were no significant differences between age groups under FGA-S and FGA-M conditions.
Functional Gait Assessment (FGA) scores and risk of fall for both groups
Functional Gait Assessment (FGA) scores and risk of fall for both groups
Abbreviations: Q1, Quartile 1; Q3, Quartile 3; FGA-S, Functional Gait Assessment single task; FGA-M, Functional Gait Assessment manual task; FGA-N, Functional Gait Assessment numeracy task; FGA-L, Functional Gait Assessment literacy task. a = The risk of fall was calculated based on a total score of 22 or less (24). *p≤0.05, **p≤0.001. *†A significant relationship between dual-task condition and fall risk, p≤0.05.
The only dual-task condition significantly associated with falls risk was FGA-N, χ2(1) = 7.57, p≤0.05 (Table 2), with 51.2% of the older group scoring 22 or less. Within the younger group, falls risk was independent of dual-task condition.
Dual-task cost (DTC) was significantly different between age groups, with greater cost observed in the older age group for FGA-N (z = –2.37, p≤0.05, r = 0.26) and FGA-L (z = –2.53, p≤0.05, r = 0.28), but not FGA-M (Table 3).
Dual-task cost (DTC) for both groups
Dual-task cost (DTC) for both groups
Abbreviations: DTC, Dual-Task Cost; Q1, Quartile 1; Q3, Quartile 3; Functional Gait Assessment single task; FGA-M, Functional Gait Assessment manual task; FGA-N, Functional Gait Assessment numeracy task; FGA-L, Functional Gait Assessment literacy task, *p≤0.05.
There were no statistically significant differences between groups for response accuracy under both FGA-N and FGA-L conditions (Table 4).
Response accuracy for cognitive tasks for both groups
Response accuracy for cognitive tasks for both groups
Abbreviations: Q1, Quartile 1; Q3, Quartile 3; FGA-N, Functional Gait Assessment numeracy task; FGA-L, Functional Gait Assessment literacy task.
BADs age corrected score did not show significant differences between-groups. When comparing performance between the younger and older age groups for each sub-test, significant differences were observed for Test 3 (z = –2.79, p≤0.05, r = 0.35) and Test 5 (z = –3.01, p≤0.05, r = 0.35) (Fig. 1), which evaluate planning and behavioural regulation respectively [26] (Fig. 1).
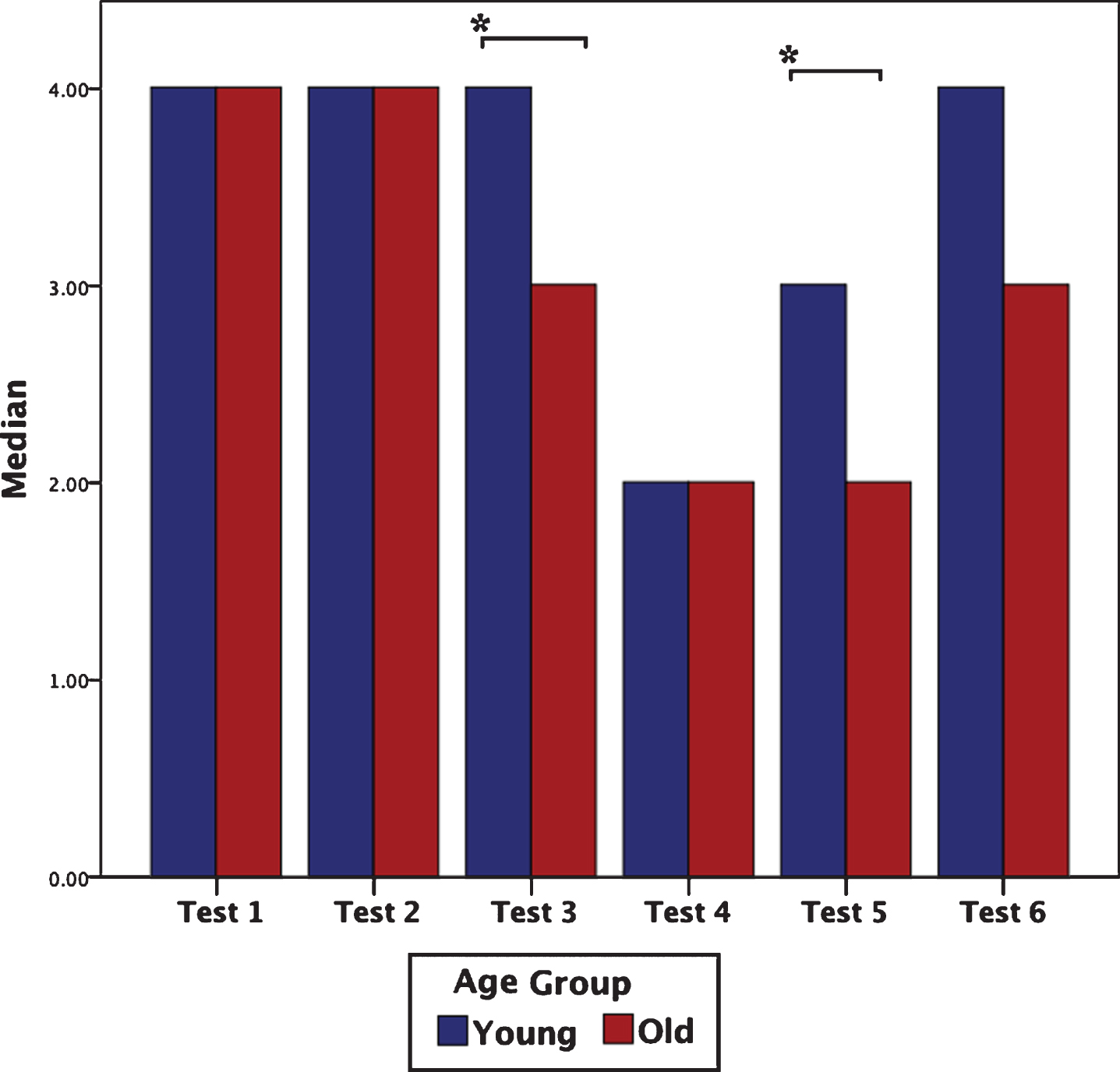
Median Behavioural Assessment of the Dysexecutive Syndrome (BADS) sub-test scores for both groups. Abbreviations: Test 1 = Rule Shift Cards; Test 2 = The Action Programme; Test 3 = The Key Search Task; Test 4 = The Temporal Judgement Test; Test 5 = The Zoo Map Test; Test 6 = The Modified Six Elements Test. *p≤0.05.
In both the younger and older groups, no statistically significant correlations were noted between the BADS age corrected score or tests sub-scores and the FGA-S, FGA-M, FGA-N, FGA-L and the associated DTCs (p > 0.05).
TUG score
The TUG scores were statistically different be-tween the two age groups (t (80) = –3.402, p≤0.001, d = 0.75) with a longer duration noted for older (8.68s±1.81s) compared to younger (7.47s±1.38s) subjects.
Discussion
In this study, we compared dual-task ability on a dual-tasking FGA tool between healthy younger and older adults and we investigated whether a relationship exists between executive function and dual-tasking ability on the FGA. This study adds to emerging evidence on dual-task interference during more attention-demanding gait tasks. Complex dual gait tasks assess the ability to walk in diverse and challenging environments and hence, may provide a more accurate indication of functional ability compared to simple dual gait tasks. Therefore an investigation into age-related differences in dual-tasking ability, on a ecologically valid dual-tasking FGA tool, could provide valuable information for future dual-task assessment and intervention protocols.
The main findings from this study indicate that additional cognitive tasks had a destabilising effect on dynamic balance for both younger and older adults, however, older adults were significantly more affected. No other study to date has investigated age-related differences in dual-tasking ability while utilising a dual-task FGA test, although the findings of this study are consistent with a body of work pertaining to spatiotemporal gait parameters. Reduced gait speed together with increased stride-to-stride variability in stride length, stride velocity and/or stride time has been reported in older adults compared with younger adults, under cognitive dual task conditions [27–29] with increased stride-to-stride variability a marker of gait instability which predicts falls [30]. A strength of the present study, in contrast to previous studies evaluating age-related differences [27–29], is that it utilised the recommended DTC formula [31] to account for dual-task interference on dynamic balance. This will facilitate between-study comparisons in the future [31] with the DTC also important as it accounts for baseline differences in single task performance, providing a true dual-task change [32].
In order to investigate whether FGA performance with a secondary dual-task is suitable for determining falls risk, the FGA scores under the three dual-task conditions were compared to a previously determined cut off value for FGA-S, which predicts a fall within six months, in community-dwelling older adults [24]. Only performance on FGA-N was significantly associated with falls risk for older adults, with 51% scoring less than 22. This finding adds to growing literature linking dual-task interference to falls risk [10]. The concept of prioritization may serve as a possible explanation for the observed decline in dynamic balance while performing a secondary cognitive task. In this study, participants were not given explicit instructions regarding task prioritisation. However, the performance of secondary cognitive tasks had a deleterious effect on dynamic balance in the older group, with FGA-N significantly associated with an increased falls risk. This, together with the comparable cognitive performance between both age groups suggests that healthy older adults do not prioritise gait, under cognitive dual-task conditions, consistent with previous findings [33, 34]. This is in contrast with the “posture first strategy”, in which all attention is directed toward maintaining balance and preventing falls. However, recent research suggests this is dependent on environmental factors, individual characteristics and the complexity of motor and cognitive task demands [35, 36]. The effect of dual tasking on the posture first strategy has recently been attributed to the neural insufficiency model; increased brain activation in the context of diminished gait performance [11, 38].
The cognitive tasks used in our study, classified as mental tracking tasks [2] were utilised since emerging evidence suggests that they are most disruptive on gait performance, compared to other types of secondary tasks [2, 39] and may have superior falls predictive ability [39]. However, the effects of the cognitive mental tracking tasks did not appear to be equal. Results indicate that the numeracy task was the most difficult with the greatest median score reduction and DTC observed in both groups. This is consistent with literature indicating that the effect of the secondary task is dependent on its complexity [40]. Since significant dual-task decrements were observed under both cognitive dual-task conditions, this might demonstrate that the type of secondary task is relevant with a cognitive task more challenging than a dual-manual task.
Subclinical age-related differences were observed with respect to the BADS total profile and standardised scores, which were not significant when age was removed as a confounding factor. This result was not surprising given the existing literature on the high vulnerability of the frontal lobe to age-related changes and the associated subclinical decline of executive functions with advancing age [41]. When performance was analysed for each sub-test, the results indicated that the planning and behavioural regulation abilities of the older group were significantly reduced compared to the younger group as reflected in the BADs subscore in two tests (key search & zoo map test). While age-related deficits in performance on The Zoo Map Test have been reported elsewhere [42], no studies to our knowledge have observed these findings with respect to The Key Search Test.
The results from this study indicate that executive function is not related to dual-tasking ability on a complex dual-tasking FGA. This finding is in sharp contrast to existing literature [7, 44] and is particularly unexpected given that executive function is considered most relevant in complex gait situations [9, 45–47], akin to the various FGA items. The contrasting results may be partially explained by differences in methodological design. This study utilised the FGA clinical gait tool to assess dynamic balance under dual-task conditions, whereas the majority of the existing research evaluated selected gait parameters such as speed and stride-time variability [7, 44]. These spatiotemporal parameters are not considered representative of dynamic postural control, with step width and step width variability thought to more accurately reflect this key feature of gait [17]. Furthermore, to our knowledge, only one study examines the interplay between executive function and gait has utilized the BADS [48] in a cohort post-stroke. Another possible explanation is the relatively young age (mean age 68.3) of the older adult group, compared to other studies [7, 37] although studies exist with similar older adult groups indicating an association between executive function and dual task ability [8, 43].
Present findings bring forth several issues with possible clinical importance. Foremost, older adults did not appear to prioritise the dynamic balance tasks in accordance with the posture first strategy under cognitive dual-task load, with performance on the FGA-N significantly associated with falls risk. This may have future application for multi-task training and falls risk assessment.
A number of limitations are acknowledged with a lack of test order randomization foremost. However, the observation that dual-task interference was greatest on the second last task (FGA-N) rather than the last (FGA-L), suggest these systematic bias had limited impact. Another limitation is that the secondary cognitive tasks were not assessed in the single-task condition, i.e. when sitting, and as such, their relative DTC cannot be determined.
Conclusion
In conclusion, this study utilised a dual-tasking FGA tool with findings providing additional evidence that attentional processes are involved in walking and that attention-demanding cognitive tasks have a destabilising effect on dynamic balance. The resultant postural instability is however, more pronounced in the older participants with performance under numeracy dual-task conditions significantly associated with falls risk. Executive function did not appear to be significantly related to dual-task ability. However, this study was conducted on a relatively homogenous population and hence, these results should be interpreted with caution. Further research involving a large heterogeneous population is warranted to validate these findings.
Conflict of interest
The authors have no conflict of interest to report.
Funding
This research received partial funding from the Ménière’s Society, UK.
Footnotes
Acknowledgments
The authors would like to thank all those who participated in the study and acknowledge the support of their departmental colleagues.