
Abstract
INTRODUCTION:
Health professionals have been subject to increased levels fatigue when compared to population norms. It remains unknown if physiotherapists report high levels of sleep deprivation. This paper explores levels of sleep deprivation, and its potential impact on professional performance.
METHODS:
A survey was distributed through the Irish Society of Chartered Physiotherapists. The survey explored work characteristics, sleep quality using the Pittsburgh Sleep Quality Index, daytime sleepiness using the Epworth Sleepiness Scale, and the professional and non-professional causes of sleep deprivation in the profession. Pearson correlation and independent t-tests were used on SPSS to explore relationship between variables.
RESULTS:
There was a total of 559 valid respondents. Females accounted for 82% and public sector employees accounted for 63% of respondents. Over half (50.1%) of respondents said they felt sleep deprivation impacted on their practice. Most physiotherapists (63.3%) of respondents said they did not feel that their practice impacted sleep. The PSQI global score was 5.6 indicating “poor” quality of sleep. The ESS global score was 6.0 indicating ‘higher normal daytime sleepiness’. Potential causes of sleep deprivation included professional issues relating to burnout and work-life balance, and non-professional reasons such as parenthood.
DISCUSSION AND CONCLUSION:
A mismatch exists between self-reported sleep deprivation and validated measurements of sleep indicating poor self-awareness of the impact of sleep in optimising professional performance. A work-life balance is needed to facilitate a safe and efficient workforce. Individual and organizational efforts should be made to improve sleep quantity and quality to reduce personnel fatigue and enhance physiotherapists professional performance.
Introduction
Sleep deprivation in healthcare practice has been found to be higher than average, and results in an increased cognitive workload [1]. Increased levels of fatigue have been reported in healthcare staff such as doctors [2] and nurses [3]. The link between fatigue, sleep deprivation and decremented aspects performance is well established [4]. Sleep deprivation is linked to decreased professional performance, especially in the cognitive and affective domains [5]. A slower reaction time [6], an inability to recognise error [7] and a reduction in procedural place-keeping adherence [8] have been associated with sleep deprived personnel. Emotional affect is altered in fatigued states [9] which may impact on non-technical skill performance such as patient empathy, shared decision-making and appropriate patient management. It may also impact on collegiality and amongst peers and teamwork [10].
Physiotherapy is a diverse profession which has parallels to careers such as medicine and nursing. A physiotherapists professional performance can be typically broken down into cognitive and affective domains –and in some specialised treatments such as suctioning, an aspect of technical skill performance. As a career, physiotherapy plays a vital role in patient postoperative care, rehabilitation and in promotion of preventative healthcare measures, as well as being key stakeholders in ensuring patient safety [11]. Known ‘human-factors’ to affect patient fatigue, including fatigue, may have contributed to cases of physiotherapy error resulting in malpractice cases relating to treatment, patient monitoring, equipment provision issues and diagnosis [12]. A degree of self-awareness of the ‘human factors’ such as fatigue is important to ensure self-monitoring and self-regulation to reduce risk of professional error-making [13]. If significant levels of sleep deprivation are reported, this may increase risk of human-related errors, particularly in aspects of practice which have direct impact on patient care such as appropriate clinical decision making [14]. This could have ramifications financially and personally for practitioner and patient alike. Compliance with regulations to protect workers against fatigue such as the European Working Time Directive (EWTD] have not been researched in physiotherapy, yet it can be assumed that such adherence is high given most physiotherapists do not play a key role in continuity of patient care (excluding on-call physiotherapists). Nonetheless, this research aims to explore sleep in Irish physiotherapists as it remains unknown if physiotherapists report high levels of sleep deprivation and whether this impacts on their professional performance.
Objectives
The specific objectives of this research were to To identify if physiotherapists report significant levels of sleep deprivation To identify if sleep deprivation in physiotherapy impacts on self-reported professional and personal activities To highlight self-reported causes of sleep deprivation in physiotherapy
Methodology
Research participants
Registered chartered physiotherapists from the Irish Society of Chartered Physiotherapists (ISCP) were invited to complete the survey. A sample size of at least 340 respondents was required to reflect participation levels of ISCP members in published survey studies and to mitigate bias. This is approximately 11.3% of a 3000 membership database, inclusive of a margin of error of 5% and a confidence interval of 95%. Valid responses were considered those which completed the survey in full.
Survey design
Participants were asked a series of demographic questions including their level of training, job specification, sectoral area, and specialty. Participants were asked if they feel their work as a physiotherapist impacts on their level of sleep and if sleep deprivation impacts on their work performance. If so, they are asked to disclose what particular tasks they find most impacted. Participants then completed two validated tools –the Pittsburgh Sleep Quality Index Measure (PSQI) and the Epworth Sleepiness Scale (ESS). The PSQI is used to assess sleep quality and sleep patterns under seven domains –subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction [15]. The Epworth Sleepiness Scale [16] assesses sleepiness during daytime activities.
Statistical analysis
Data was analysed for normal distribution and statistical tests were applied using Statistical Package for Social Sciences (SPSS). Pearson Correlations were used to examine relationships between demographics, binary questions and validated questionnaires. Independent t-tests compared significant differences between validated questionnaire and binary question outputs. When exploring open-ended questions, a modified thematic Analysis approach was taken [17]. The data was first coded using thematic coding, then quantified using a magnitude coding strategy and further differentiated into demographic differences to establish primary reasons for self-reported sleep deprivation in physiotherapists.
Results
Demographics
There was a total respondent list of 613 respondents of which 559 valid respondents completed the full survey. The breakdown in demographics is seen in Table 1 below. More females worked in the public sector (67.32%) while more males work in the private sector (60.2%) (p < 0.05). More females worked in hospital outpatient (20.04% v 9.18%) while more males worked in private practice (46.94% v 24.4%) (p < 0.05).
Demographic Breakdown of Physiotherapists
Demographic Breakdown of Physiotherapists
When asked if physiotherapists felt their work as a physiotherapist resulted in sleep deprivation, 63.3% of respondents said they did not feel that their professional practice impacted sleep. There were differences between the age groups 25–34 year olds (48.85%) and 45–54 year olds (40.19%) and 35–44 year olds (29.5%) in levels of reported sleep deprivation resulting from physiotherapy work (p < 0.05). Figure 1 shows the trend between age, reported sleep deprivation and impact on professional performance.
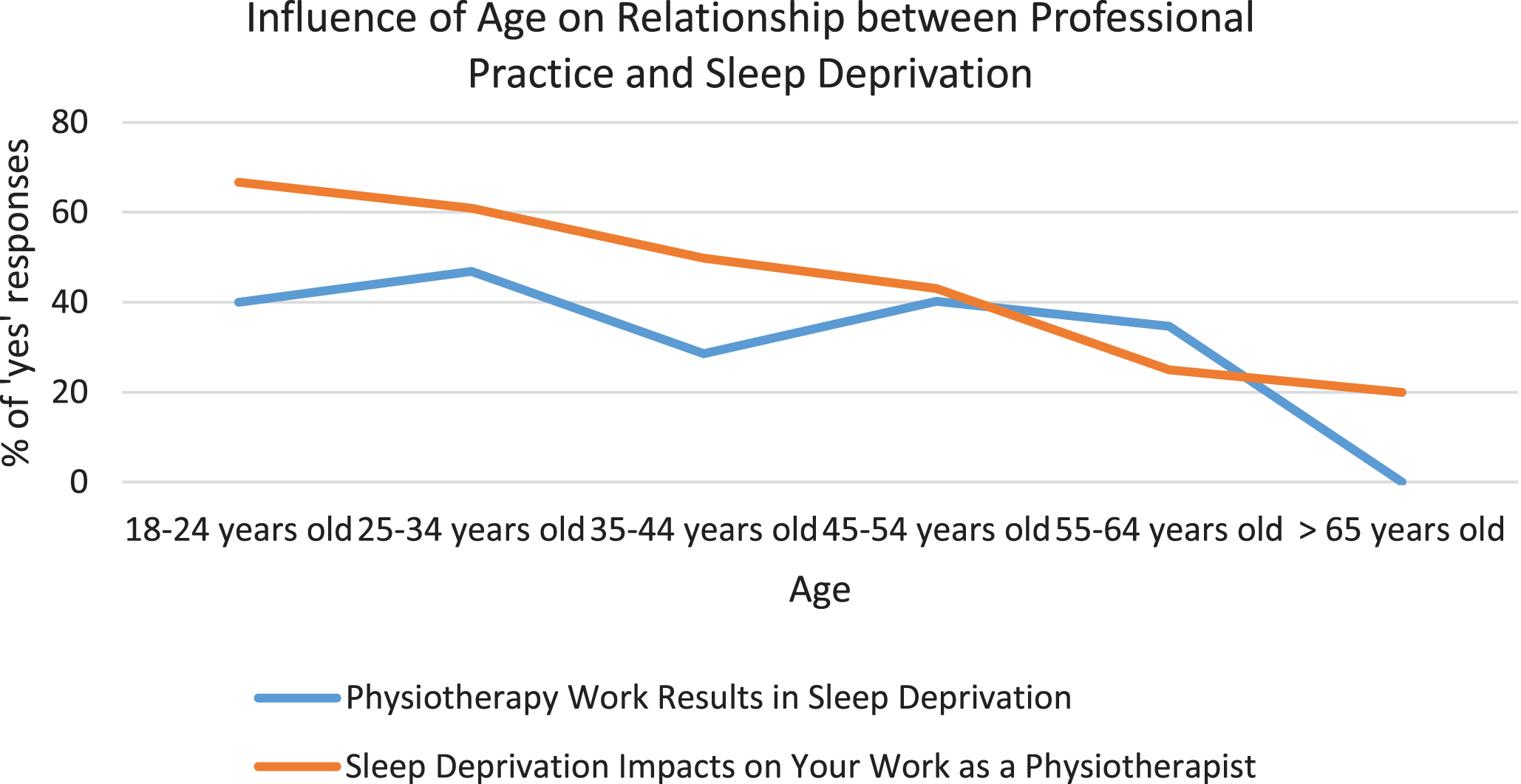
Graph showing higher self-reported ‘yes’ responses in younger physiotherapists to sleep deprivation impacting on physiotherapy practice, and physiotherapy practice resulting in sleep deprivation.
On objective assessment using PSQI scores, a global score of 5.6 was found indicating a “poor” quality of sleep. Scores for the summative component scores are seen in Table 2.
Summative Scores for the Components of the Pittsburgh Sleep Quality Index and Epworth Sleepiness Scale showing ‘poor’ quality sleep according to the PSQI and ‘higher daytime sleepiness’ according to the ESS
Summative Scores for the Components of the Pittsburgh Sleep Quality Index and Epworth Sleepiness Scale showing ‘poor’ quality sleep according to the PSQI and ‘higher daytime sleepiness’ according to the ESS
On overall PSQI scores there were differences between age groups as seen in Fig. 2.
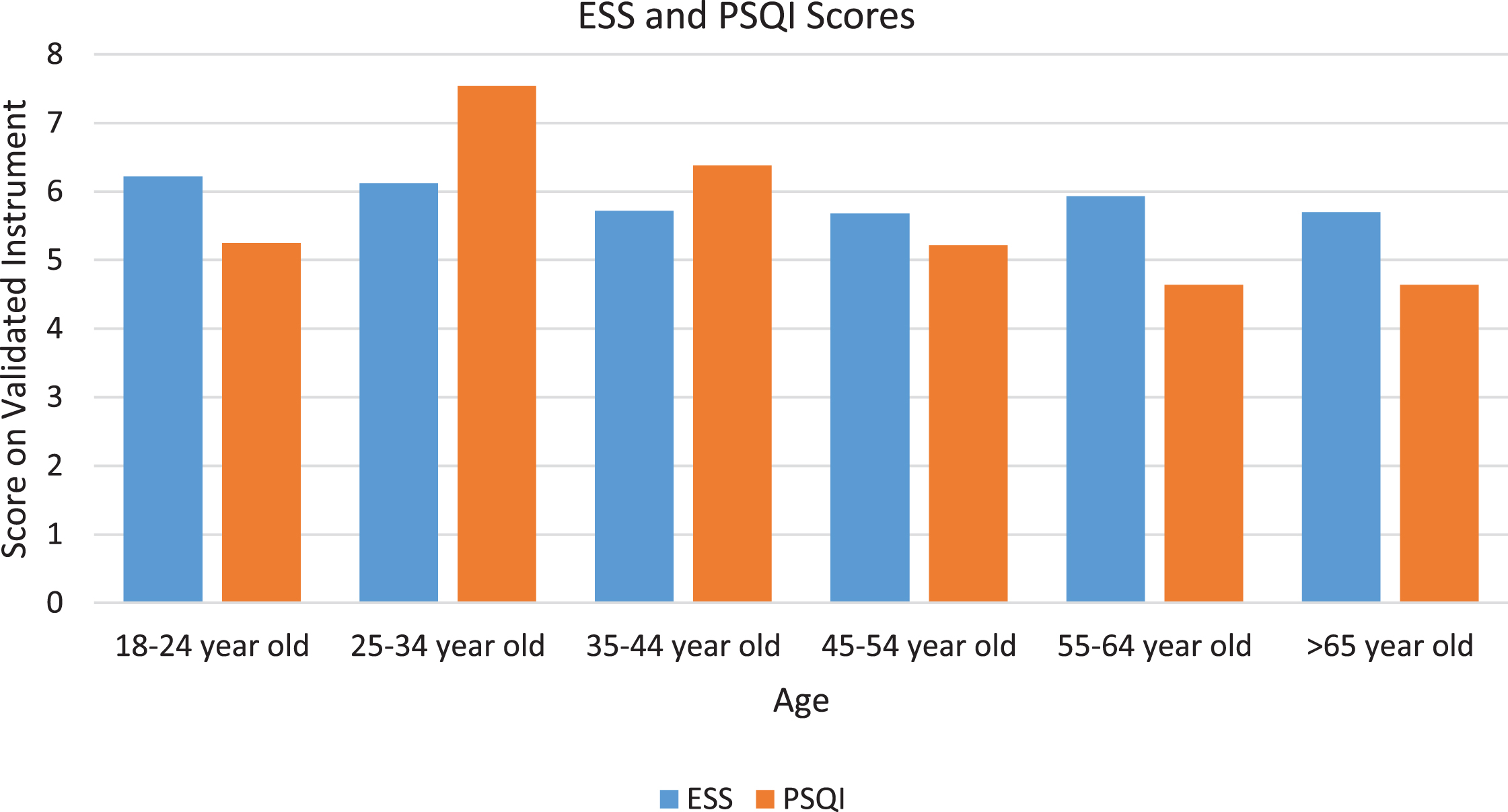
Breakdown in daytime sleepiness and sleep quality scores across physiotherapy age groups showing worse sleep quality in physiotherapists aged 25–44.
On individual aspects of the PSQI there were a number of significant differences between age groups and professional levels (p < 0.05). PSQI component scores for age groups and professional levels are seen in Table 3. Respondents who reported ‘no’ to the question ‘do you feel your work as a physiotherapist is impacting on your sleep’ were more likely to report a ‘very good’ sleep quality (28.8% in ‘no’ respondents v 3.9% in yes’ respondents). Respondents who reported ‘yes’ to the question ‘do you feel your work as a physiotherapist is impacting on your sleep’ were more likely to report a ‘fairly bad’ sleep quality (36.07% in ‘yes’ respondents v. 11.47% in ‘no’ respondents). Respondents who reported ‘no’ to the question ‘do you feel sleep deprivation impacts on your work as a physiotherapist’ were more likely to report a ‘very good’ sleep quality (32.6% in ‘no’ respondents v 6.79% in ‘yes’ respondents).
Mean scores and standard deviations for age and professional level breakdown on the Pittsburgh Sleep Quality Index. * indicates a statistically higher score at the level of p < 0.05 compared to other demographics
When asked if physiotherapists self-reported sleep deprivation impacts on their professional practice, 50.1% of respondents responded ‘yes’. The most affected activities are seen in Fig. 3.
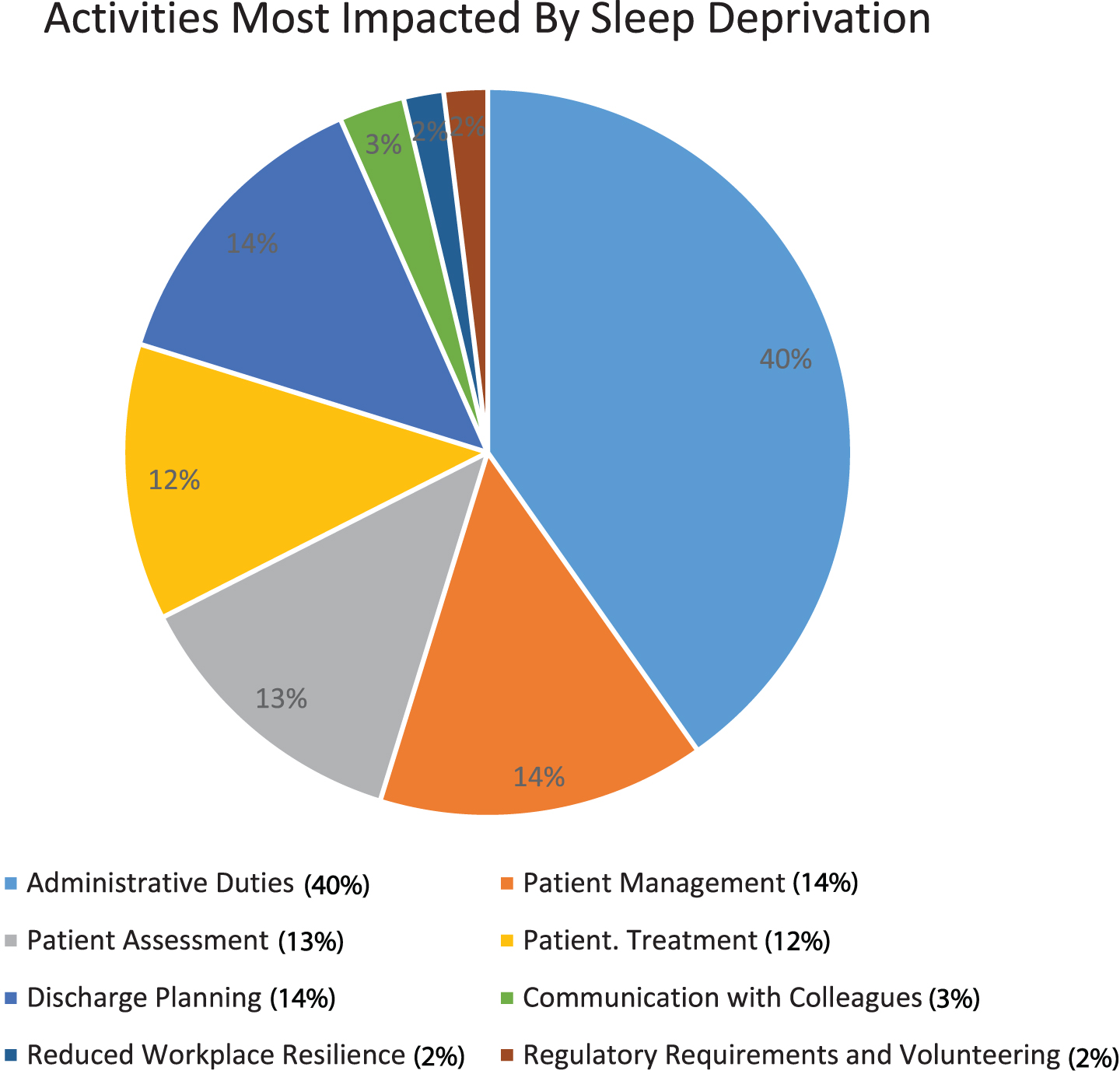
Percentage breakdown of activities most affected by sleep deprivation in all participants physiotherapy professional practice.
Physiotherapists aged 18–24 (66.67%) and 25–34 (60.84%) reported a higher ‘yes’ percentage to sleep deprivation impacting on self-reported professional activities compared to 35–44 (49.76%), 45–54 (42.99%). and 55–64 year olds (25%). Those who reported ‘yes’ to work being impacted by sleep levels were more likely to say ‘yes’ to sleep deprivation impacting on their work as a physiotherapist (77.1% in ‘yes’ respondents v 22.93% in ‘no’ respondents). Staff grade physiotherapists reported a higher ‘yes’ percentage of 60.91% compared to senior physiotherapists (47.37%) and private practitioners (46.94%). Public sector employees were more likely to report sleep deprivation impacting on ‘discharge planning’ (12.21%) when compared to private sector employees (3.85%). Musculoskeletal physiotherapists reported sleep deprivation impacting ‘patient assessment’ at a greater level (25.9%) than paediatric physiotherapists (5.9%).
On objective assessment using the Epworth Sleepiness Scale, the global score was 6.0 indicating ‘higher normal daytime sleepiness’. Scores for the summative component measures are seen in Table 2. On overall ESS scores there were differences between age groups as seen in Fig. 2. On individual aspects of the ESS there were significant differences between age groups (p < 0.05). ESS component scores for age groups and professional levels are seen in Table 4.
Mean scores and standard deviations for age and professional level breakdown on the Epworth Sleepiness Scale. * indicates a statistically higher score at the level of p < 0.05 compared to other demographics
Mean scores and standard deviations for age and professional level breakdown on the Epworth Sleepiness Scale. * indicates a statistically higher score at the level of p < 0.05 compared to other demographics
When asked if physiotherapists had any other comments relating to the topic of sleep deprivation in the profession, there was 99 respondents coded thematically in Fig. 4.
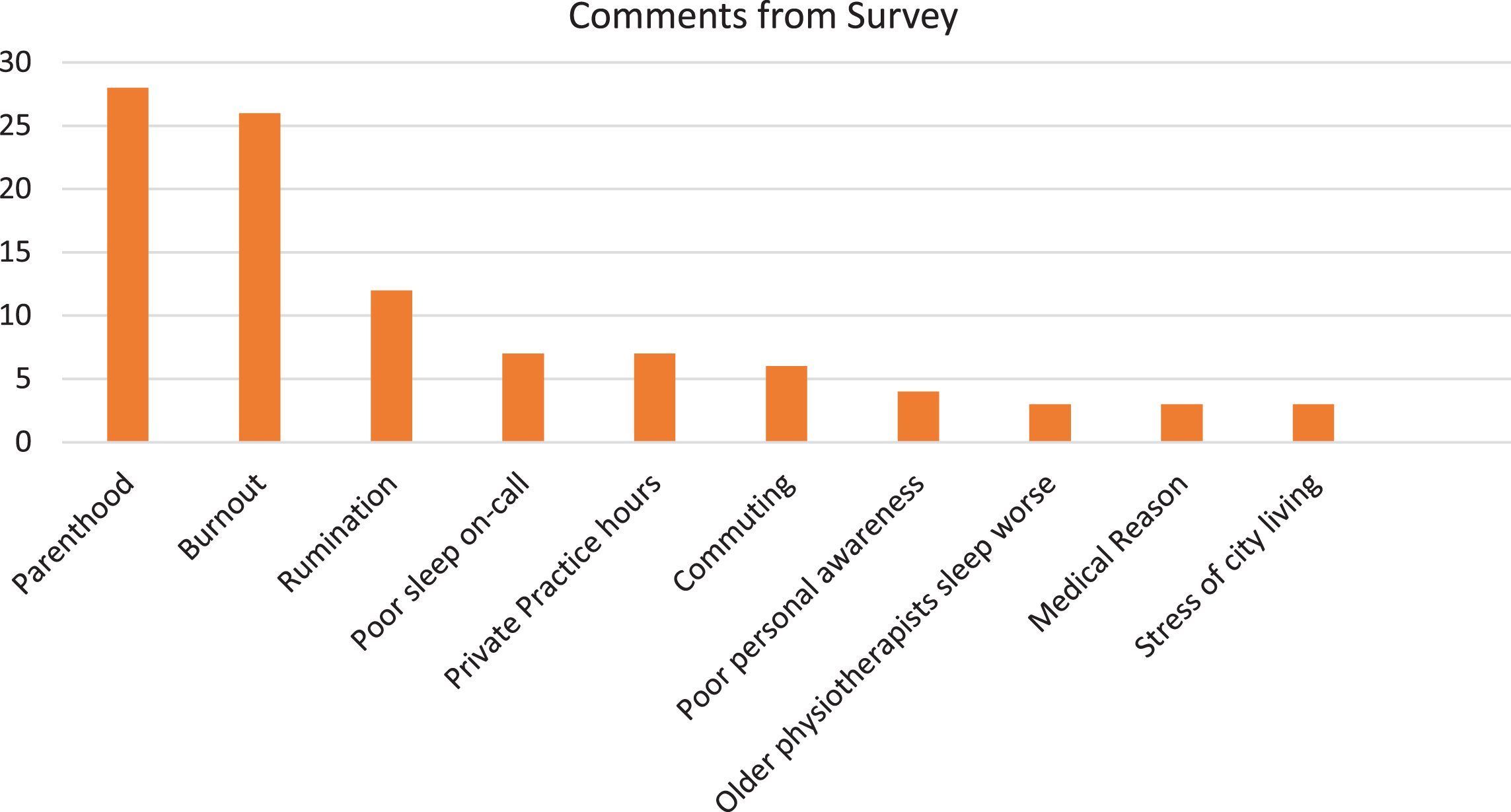
Coded Responses from ‘Any other comments’ section of the survey.
The discussion around sleep has been at the forefront in recent years given the increase in research showing the decremented health associated with sleep deprivation including an increased risk of diabetes [18], hypertension [19] and dementia [20] to name a few. In addition, research focusing on work performance and sleep deprivation has been explored in industries such as aviation [21] and more closely aligned, surgery [1] and nursing [22]. There is a growing amount of evidence to suggest that cognitive performance is affected in sleep deprived or fatigued states –in particular with reaction time [6] and their flexibility and innovation in decision making [23]. While most of these studies have been conducted in laboratory conditions, they may have some applicability to physiotherapy practice.
Physiotherapists poor sleep quality may impact performance
When looking at the objective validated tools to assess sleep deprivation [24], physiotherapists are not sleeping well. A global sum of “5”or greater indicates a “poor” quality of sleep, with higher scores, as in our study which found 5.6, indicating a greater decrement in sleep quality. A wholly score of 6.0 indicating ‘higher normal daytime sleepiness’ in the Epworth Sleepiness Scale was found pathological sleepiness (>15) yet higher ESS scores, indicating poor sleep quality, have been reported in healthcare personnel compared to general population norms [25, 26]. Increased sleepiness and fatigue are likely to have implications for occupational task performance, particularly in tasks which require high sustained vigilance, and involve newly learned skills [27], as well as cognitive and affective tasks such as clinical decision making and effective communication. In parallel professions, such as medicine, a meta-analysis of sixty studies found that continued wakefulness in medicine reduced physician’s performance significantly through decreased vigilance, cognition, memory recall and clinical performance [28]. Prolonged sleep deprivation is even likely to negatively impact intuitive procedural based technical skills [29]. Sleep deprivation in physiotherapy is likely to impact quality of life-long learning opportunities [27] with medical residents reporting a negative association between long working hours and effective learning [30]. This has ramifications for upskilling and continuous professional development. Finally, sleep deprivation may impact quality of patient care through increased likelihood of error-making [31, 32] and associated practices such as comprehensiveness in subjective and objective patient examination [33]. Additionally, more nuanced competencies such as professionalism, which are important for non-technical skills like patient empathy, teamwork, and professional identity are likely to be impacted by sleep deprivation as demonstrated in medicine [34]. Such decremented performance places increased risks to both physiotherapists and patient alike.
There exists a mismatch between self-reported sleep deprivation resulting from work (two-thirds of physiotherapists reporting that their work does not impact on their sleep levels), and sleep impacting on work (just over half of physiotherapists reporting sleep deprivation impacts on their work) in conjunction with the objective validated tools. This would support research that individual’s perception of subjective sleepiness and impairment is poor resulting in underreporting [27]. In fatigued states, this may lead physiotherapists to overestimate their ability and continue to work, leading to a cycle of activating compensatory psychophysiological mechanisms, which results in increased strain and delayed onset cumulative fatigue [35]. The self-perception of whether people feel they are sleep deprived versus the validated tools may suggest that there is a lack of awareness as to what constitutes a good quality of sleep. This is particularly worrying given that many studies have found that humans do not adapt to chronic levels of sleep restriction, but rather perform sub-optimally [36] at the detriment to physical and mental health. It has also operational implications for ‘fit for duty’ status of personnel [27]. If work-load is adapted to more administrative work, productivity in desktop-based work will be non-stimulating and non-productive given the low cognitive demands of the tasks. In fact, such work may in fact ‘unmask’ physiological levels of sleepiness resulting in ‘automatic behavior syndrome’ which is is characterised by the ability to perform some aspects of monotonous work, but with an increased risk of error-making secondary to decreased situational awareness or judgement [37].
There are several causes for sleep deprivation in the profession
Professional reasons
Insufficient sleep, in tandem with rumination about work and high work demands in the healthcare system are risk factors which may be contributing to levels of sleep deprivation and subsequently fatigue in the profession –“I find since our hours increased in the public sector, this has impacted on my time outside or work.. I feel like I’m on the back foot for the whole evening, trying to fit in my usual activities”. Burnout is characterised by increased exhaustion, cynicism and inefficacy [38]. It is closely linked to staff resourcing and would indicate that fatigue and sleep loss is intrinsically linked to provision of sufficient personnel and facilities [39]. Overworked and fatigued staff links to greater absenteeism rates [40] which places a greater strain on the system. Sleep deprivation is also likely to have knock on effects for healthcare staff wellbeing and safety. Risk to life including micro-sleep induced car crashes are much higher in healthcare workers [41], as well as higher rates of suicide [42]. Sleep-deprived medical trainees are also more likely to utilise damaging coping strategies such as increasing alcohol intake and increasing medication intake to remain alert [43]. Compassion fatigue and management of work-induced insomnia is prevalent, particularly amongst younger physiotherapists - ““It is very difficult to switch off at night - thinking about patients you had that day and thinking about patients you have the following day”.
Personal reasons
There was a noticeable decline in reporting of sleep deprivation in middle-aged physiotherapists as a result of physiotherapy work. On objective measures however, consistent levels of reduced sleep quality exist in this cohort. As a female dominated profession, parenthood may be the primary reason for sleep deprivation in this age group - –“Family impacts my sleep more than professional reasons, but children are a large role in many professionals lives so needs to be considered”. We do notice that the trend of reporting sleep deprivation from physiotherapy work increases again in 45–54 year old’s before gradually decreasing once again. This may reflect a return to workload responsibilities and managing the transition back into workload responsibilities while balancing parenthood. Additionally, the menstrual cycle, pregnancy, and menopause have been found to impact on sleep quality and quantity in working women and this study may support such evidence [44, 45]. Amongst older physiotherapists, the importance of ‘age’ impacting both sleep quality and professional performance was highest in this age group. Private sector employment was highest in over 65’s (80%) and an ageing musculature, in conjunction with lack of sleep may result in a hypersensitized pain reception [46].
Addressing the issue of sleep deprivation and fatigue in physiotherapy
Effective management of the risk associated with fatigue and performance decrement have proven effective in the aviation industry and similar principles may improve patient outcomes in healthcare [47]. One of the greatest challenges in healthcare is changing the culture towards fatigue. Efforts to emphasise the importance of promoting the necessity of sufficient rest to ensure optimal patient care is needed [48]. Regulatory changes such as the EWTD have brought seismic changes in work-hours in some disciplines such as medicine, with some studies finding that physicians-in-training were working between 80–120 hours pre-mandate [49, 50]. Yet such efforts may have had antipodal impacts for other professions such as nursing and physiotherapy as more responsibility, inclusive of on-call duties is transferred to these disciplines [27]. While operational measures such as work shift alterations stemming from initiatives like the EWTD have been important to create opportunity for greater fatigue management, the first meaningful step to addressing the issue of sleep deprivation in personnel is increasing self-awareness. Behavioural change is routed in an understanding that autonomy of understanding rationale for changes is required in order to accept that change as a personal responsibility [27]. Most healthcare professionals, despite working in an industry which subjects them to 24-hour work, receive no education in sleep science or the importance of sleep in maintaining personal health and occupational performance [51]. A positive output from this survey highlighted by some physiotherapists is that they have become more aware of their sleep patterns and will work to improve them. A robust fatigue management programme within institutions should be implemented, incorporating education on sleep science, the relationship between sleep and performance management, and effective mitigation strategies. In addition, education on sleep hygiene techniques, or provision of psychological therapies such as acceptance and commitment therapy (ACT) or cognitive behavioural therapy (CBT) to tackle insomnia in healthcare workers is likely to be effective in tackling issues which arose in this study such as difficulty falling asleep and rumination.
Addressing the stressors of the workplace and promoting a work-life balance is important, particularly in younger age groups who are entering the workforce. Management should also consider the risk of fatigued personnel on patient outcomes [52] and advocate for enabling effective fatigue mitigating interventions. Rostering, underpinned by biomathematical approaches [53] should be used for those entering and leaving the workforce. For those returning to work, this may include a gradual return to graded responsibilities in the workforce, greater flexibility in working hours and annual leave, and provision of childcare facilities on site. For those near retirement, management should be aware of ageing practitioners, and the potential value in which they play in running efficient healthcare services - while being cognisant and effortful to be non-discriminatory. Practitioners performance, as has been discussed in parallel industries such as surgery, should be assessed on ability and not chronological age [54]. Management should model work-loads to ensure that physiotherapists have appropriate workload demands, with variety to ensure mental stimulation, reduce overcapacity and optimise performance.
Finally, in cases of unavoidable sleep disturbance, such as in physiotherapists who complete on-call work - “when I’m on call and if I get called in late at night, I find it very difficult to unwind and get back to sleep after I get home”, increased breaks should be given in either the preceding day or subsequent day to allow sufficient rest to recover. Alternatively, strategic napping, with an optimal duration of 15–20 minutes to reduce sleep inertia [55] in the workplace may temporarily alleviate the effects of sleep loss [56]. The provision of appropriate rest facilities is likely to have positive effects in this regard. Caffeine consumption should also be strategically taken in times of low alertness to maximise effectiveness but should be limited leading up to times of planned rest [57].
Strengths and limitations
There are some strengths and limitations to this study. The demographics in this survey are representative of the population breakdown in the physio-therapy profession in Ireland. As a female dominated profession, there was opportunities to explore issues which may be context specific to the female worker. The high response rate is greater than surveys conducted by the ISCP, which usually plateau between 300–350 respondents. Nearly half of physiotherapists were working in musculoskeletal medicine and orthopaedics which limits the generalizability of the research to all specialties.
Conclusion
Sleep deprivation is significantly reported in physiotherapy. This is most evidently seen in a poor quality of sleep score in the Pittsburgh Sleep Quality Index. Over half of physiotherapists report that sleep deprivation impacts on their physiotherapy activities while a third of physiotherapists are sleep deprived as a result of their physiotherapy activities. Efforts such as adherence to prescriptive regulations, and a series of fatigue risk management approaches, encompassing personal and professional modifications may be required to facilitate a productive workforce and a safe work environment for workers and patients alike.
Conflict of interest
None.
Ethical considerations
Ethical Approval was given by the School of Medicine Research Ethics Committee at Trinity College, The University of Dublin.