
Abstract
PURPOSE:
We evaluated the attitudes of nurses compared to physiotherapy assistants and medical masseurs (PAMs) regarding various treatment modalities used in the treatment of low-back pain (LBP) as their opinions might influence the patients’ attitudes to therapy.
DESIGN:
Cross sectional self-reported questionnaire survey.
METHODS:
175 Hungarian health care providers completed questionnaires evaluating their opinions on the importance of various therapeutic interventions and the need for initiation of LBP treatment. Their personal LBP history and fear-avoidance beliefs (FABQ) were also investigated.
FINDINGS:
The importance of exercise therapy (p = 0.024) and massage (p < 0.01) was evaluated higher by the PAMs, while medication (p = 0.04) was scored higher by the nurses. Those who experienced moderate or severe LBP were more positive about pain medication than to those with mild pain (p = 0.048). Years in health care work had only a weak association with opinions. The nurses reported more fear-avoidance beliefs than the PAMs about both physical activity (p = 0.024) and work (p = 0.021). Those who experienced moderate or severe LBP had higher FABQ scores (p = 0,076), however the difference was significant only for FABQ activity (p = 0.035).
CONCLUSIONS:
Our study confirmed that professional background and years of experience can influence the attitudes towards the importance of certain therapies, although these differences were small. Experiencing moderate or severe LBP increased the fear-avoidance beliefs about work and physical activity independently of the professional background.
CLINICAL RELEVANCE:
Our study draws the attention to the importance of standardization of the information to be passed to the patients and to the need of discussing personal experiences and beliefs during professional training.
Considerations for team work in low-back pain care
Low-back pain (LBP) is one of the most common reasons for medical consultation. In most cases, the symptoms are self-limiting or can be controlled within a short period of time, but in approximately 10% of the cases they persist for a longer term. Pain that persists for at least three months is considered to be chronic [1]. Treatment is ideally administered in accordance with therapeutic guidelines, based on the time course and the intensity of the pain [2]. According to the current LBP guidelines (NICE, APA) [1, 3], the most important goal of treatment is to maintain or restore physical activity and everyday functions. In order to achieve these goals, a biopsychosocial approach can be more effective than a biomedical approach leading to better outcomes regarding pain experience as well as work status and disability, as confirmed by a Cochrane systematic review (Kamper et al., 2014)
This emphasizes that besides providing evidence-based treatments, considering the psychosocial background and communicating effectively with the patients are also important. The US guidelines published in 2017 recommend that “clinicians should also provide patients with evidence-based information regarding their expected course, advise them to remain active as tolerated, and provide information about effective self-care options. Clinicians and patients should use a shared decision-making approach to select the most appropriate treatment based on patient preferences, availability, harms, and costs of the interventions“ [1]. The patients’ self-management activities contribute significantly to the decrease of the pain, to the improvement of the functions and to the overall outcomes [4, 13]. The guidelines also state that both the diagnosis and the treatment of LBP should be multidisciplinary tasks performed through teamwork [5, 6]. Consequently, patients get into contact with various health-care workers over the course of their treatment, and these encounters provide opportunities to deliver various treatment recommendations.
Although the composition of the team may vary depending on local habits and available care options, the leader of the medical team is always the physician who establishes the diagnosis and prescribes the treatments [7]. A number of studies have shown that physicians’ therapeutic decisions might be influenced by several subjective factors such as the physician’s specialty, gender, ethnicity, and professional status [8]. Their own personal beliefs about physical activity influences their recommendations to patients and their adherence to treatment guidelines [9–11]. Typically the patient’s first consultation on their low back pain is with their GP. According to Bishop et al. (2007) only 13,1% of the GPs followed strictly the treatments guidelines about physical activity, with 54,5% broadly following the guidelines; regarding return to work, they adhered strictly in 17,4% and broadly in 54,5%. Their recommendations were influenced by their pain attitudes and beliefs [12]. Further studies have confirmed that the fear-avoidance beliefs of family practitioners [13, 14] or teaching family practitionaires or other specialities [15] have an impact on their therapeutic recommendations, eg. those with high fear of physical acitivity prescribe more imaging exams, and recommend bed rest more often [13]. High FABQ work scores among GPs were associated with prescribing more often sick leave [14].
Added to that, patients have limited time to ask questions during medical interviews, the average length of a doctor-patient encounter being less than 5 minutes based on a review of 67 countries [16]; therefore they will raise questions to other available health care team members, such as nurses, exercise therapists, physiotherapy assistants or masseurs [5]. If the health care providers’ opinion differ from the physician’s, it can modify the patients’ expectations and reactions regarding the treatments received. This might have an important effect on patient outcomes as well. For instance, based on the study of Witt et al., the opinion of the healthcare staff influenced the patients’ pain reduction and the improvement of their physical functions [17]. Houben et al. found that more biomedically oriented paramedical therapists view daily activities as more harmful for the LBP and are more inclined to advise patients to limit daily activity and work compared with biopsychosocial oriented therapists [18]. Other studies on the attitudes of physiotherapists show that having more training on the biopsychosocial approach and working on a team has positive impact on their knowledge and adherence to guidelines [11, 20].
A survey among 170 physiotherapists concluded that their therapeutic advices were in accordance with the guideline recommendations; over 95 % of the respondents adhered strictly or broadly to the guidelines by advising to return to work and to continue physical activities, and 100% would tell their clients to avoid resting in bed [21]. Overall, the knowledge and the attitudes of both the patients and the health care providers are influenced by personal and professional experiences, health concepts, culture and environment [9].
The patients have more and more opportunities to gather information outside the office. Various forms of publication are available for this, such as flyers, booklets, educational videos or websites, the content being provided by health care centers or patient organizations. Publications reflecting the biopsychosocial approach were found to be more effective to improve the patients knowledge about their condition and to influence positively their expectations regarding physical activity [14]. However, the accuracy and the reliability of the information available on the internet is not always satisfactory. A study published in 2012 found that only 3 (13.6%) of 22 English websites followed the guidelines accurately. [22] Ferreira et al. (2019) analysed 79 webpages from 6 different English speaking countries, and evaluated only 43% of all recommendations as accurate. In average 28% (4/14) of the guideline recommendations for acute LBP were correctly covered; the websites for radicular LBP were the least comprehensive, covering only 16% (2.3/14) of the recommendations correctly [23]. These data suggest that although the quality of the content available online is improving, yet they do not follow always the guidelines properly. Patients’ need guidance on which websites are reliable. A qualitative study illustrates that despite the various available sources of information, the physicians’ statements have the greatest long term influence on the patients’ beliefs and self-management [9].
The planning of the treatment is preferably based on shared medical decision making (SMD), which is an interactive, dynamic process that extends beyond informed decision making. A number of factors have an impact on it, including patient related (e.g. preferences, desire for information) and provider related (e.g. attitudes toward shared medical decision, patient-provider relationship) factors [24]. Therefore, it is important to pay attention to the attitudes of the patients and the team members regarding the efficacy of the various relevant treatment modalities.
Most of these previous studies focused on physicians and physiotherapists. We have set the focus of our study on the attitudes of nurses, physiotherapy assistants and medical masseurs (PAMs). They have less qualification but they spend more time with the patients; therefore, they can also have an influence on their attitudes towards treatments and self-management. They can reinforce the patients’ motivation and self-efficacy to engage in regular physical activity and the patients might ask for their advice on the use of as needed medication.
In Hungary nurses during their training acquire a general knowledge regarding musculoskeletal disorders; however, their educational programs devote disproportionately little time and attention to pain management. PAMs acquire special knowledge regarding musculoskeletal disorders, in addition physiotherapy assistants learn about electrotherapy, balneotherapy, thermotherapy, magnetotherapy, and medical masseurs about massage, but none of them have detailed training about pain management. Considering the above, the aim of the present study was to obtain a complex overview of the attitudes of nurses and PAMs regarding LBP treatment and to explore their personal pain experiences, and to evaluate their fear-avoidance beliefs.
Our hypotheses were: There is a difference in the opinions regarding the importance of LBP treatment modalities and the need for initiating pain management based on the professional background. Personal low back pain experience influences the opinions regarding treatment modalities and the need for initiating pain management. Professional background influences fear-avoidance beliefs about work and physical activity. The years spent at work influence the opinions formed regarding the importance of LBP treatment modalities. Personal low back pain experience influences fear-avoidance beliefs about work and physical activity. Fear avoidance beliefs influence the opinions regarding the importance of LBP treatment modalities.
The clinical relevance of this study is that although there have been studies on the attitudes and personal LBP experiences of physicians and physiotherapists, we could find only one study focusing specifically on both attitude and personal low back pain experience among nurses [25] and we found no study among PAMs. Also, to our best knowledge, there was no study yet in the Central-Eastern European region on opinions regarding LBP treatment modalities.
Methods
We conducted a cross-sectional questionnaire survey among nurses, physiotherapy assistants and medical masseurs, attending various postgraduate courses in Hungary, Budapest between November 2016 and November 2017. The courses were accredited for any health care professional; participants could come from all over the country. We did not collect data on their regional distribution. The topics of these courses were diverse: “New therapeutic methods in physiotherapy” (on 2 occasions), “Management of chronic pain” (on 2 occasions), “New knowledge on hygiene” (once).
Participants received a hard copy of the questionnaire on site, and the lecturer asked them to complete it before the start of the course, so that the new knowledge would not affect their responses. Completion of the questionnaire took 15–20 minutes. Participation in the survey was voluntary, and the participants did not receive any reimbursement or incentive for their cooperation. Individuals who returned the completed anonymous questionnaire were considered to have given their consent to participate. As attendance at the course was linked to specific professional qualifications, there were no further exclusion criteria.
The completion rate was 89% (188 out 211) however thirteen participants did not provide data on their professional background (qualification), that was a key data. Thus overall, 175 questionnaires were included in the analysis, representing 110 nurses, 35 physiotherapy assistants and 30 medical masseurs. Further missing answers are marked analysis by analysis in the results section. Based on their similar professional training, we grouped the physiotherapy assistants and the medical masseurs together and we refer to this group as “PAMs”. While nurses have secondary nursing school education, the prerequisite for the training of physiotherapy assistants and of medical masseur is high school graduation. They learn the same basic subjects such as basic care, clinical science, basic health knowledge, and then they acquire specific practical knowledge of either massage techniques or physical treatments. The proportion of theory and practice during their training is 50–50%.
The questionnaire comprised two main parts
Part 1. was developed by the authors, and included questions about three main topics: Work experience. These concerned participants’ years of experience and professional background (nurse, physiotherapy assistant or medical masseur). Personal LBP. These aimed at detecting whether the respondents had previously experienced LBP. For those who responded “yes,” information regarding the number of times they had experienced LBP, the intensity of the strongest pain they had ever experienced, and the intensity at the time of completion of the questionnaire was also obtained. Pain intensity was rated from zero to 10 points. For the analysis, pain intensity categories were defined): 1–4: mild; 5–7: moderate; 8–10: severe pain [26] Attitudes towards LBP therapeutic procedures. Rate the importance of the listed therapeutic methods in the treatment of LBP on a 5 point Likert scale (1: useless, pointless, 2: little bit important, 3: important, 4: very important, 5: essential): exercise therapy, medication, electrotherapy, massage, homeopathy, acupuncture, surgery, psychotherapy. What level of pain, in terms of intensity on the VAS scale, requires treatment? Any pain mentioned by the patient should be treated Pain levels of 1 and higher should be treated Pain levels of 4 and higher should be treated Only pain of level 8 and higher should be treated
Part 2. comprised the Hungarian version of the Fear and Avoidance Beliefs Questionnaire (FABQ) [27]. This was to be completed only by respondents who experienced LBP. The FABQ was initially published by Waddel [28], and has been translated and validated in many languages. The scale helps to quantify the fear of physical activity and work and can be used in clinical and research settings. The FABQ comprises 16 statements (e.g., “the cause of my pain is physical activity”) that are scored using a seven-point Likert scale ranging from 0 (“do not agree at all”) to 6 (“completely agree”). Consequently, the total score can range from 0 to 96, a higher score indicating a higher level of fear and avoidance. In addition, scores for two subscales can also be calculated: 1) work-related fear score (FABQ-W), which comprises seven items (total range: 0–42); and 2) physical-activity-related fear score (FABQ-A) which comprises four items (total range: 0–24). The cut off point determined as indicator of elevated risk for developing chronic pain are 14 for FABQ-A and 29 for the FABQ-W [29]. The internal consistency of the Hungarian version of the FABQ questionnaire was 0.8 for the total score; the Cronbach-alpha for the physical activity subscale was 0.66 and for the work-related fear subscale was 0.86 [18].
This study was approved by the Regional Ethical Council (no: 44009-1/2015/EKU).
Statistical analysis
We used the SPSS 15.0 program for analysis. The data were summarized using descriptive statistics and correlations were performed using Pearson’s correlation analysis. For the comparison of groups the chi square test and ANOVA were used. Level of significance was 0.05.
Results
Professional experience
The nurses (N = 110) had an average 22.3±10.1 years of experience in patient care; the PAMs (N = 65) had an average of 17.9±14.4 years.
Previous low-back pain experience
The prevalence of self-reported low-back pain among health-care professionals
The prevalence of self-reported low-back pain among health-care professionals
PAMs = physiotherapy assistants including licensed massage therapists.
To the question “What level of pain, in terms of intensity on the VAS scale, requires treatment?” 38.3% (N = 67) responded that “in all cases when pain is mentioned by the patient”, that is the answer most in accordance with the guidelines. However, we considered the answer stating “when pain intensity is 1–4 on the VAS scale” also conform to the guidelines (20.6%, N = 36). We did not find any significant difference between the answers of the nurses and the PAMs. (see Table 2)
Opinions on level of pain requiring treatment in terms of professional background
Opinions on level of pain requiring treatment in terms of professional background
PAMs: Physiotherapy assistants and medical masseurs. Khi square = 2,065 p = 0,560 (ns).
Personal pain experience and own pain intensity had no significant connection with the opinions on when pain management should be initiated. (see Table 3)
Opinions on level of pain requiring treatment in terms of own low back pain experience
chi square = 2.257 p = 0.894 (ns).
We asked the nurses and the PAMs to score the importance of treatment modalities for low-back pain from 1 to 5 (1: useless, pointless –5: essential). Results are presented on Fig. 1. Overall, the respondents scored exercise therapy as the most useful (4.06, SD = 0.90), followed by electrotherapy (3.58, SD = 0.82) and massage (3.42, SD = 0.93); meanwhile, the importance of medication was scored (3.09, SD = 0.87) and psychotherapy was scored 2.58 (SD = 1.13). Complementary methods such as acupuncture (2.24, SD = 1.01) and homeopathy (1.81 SD = 0.95) reached low scores.
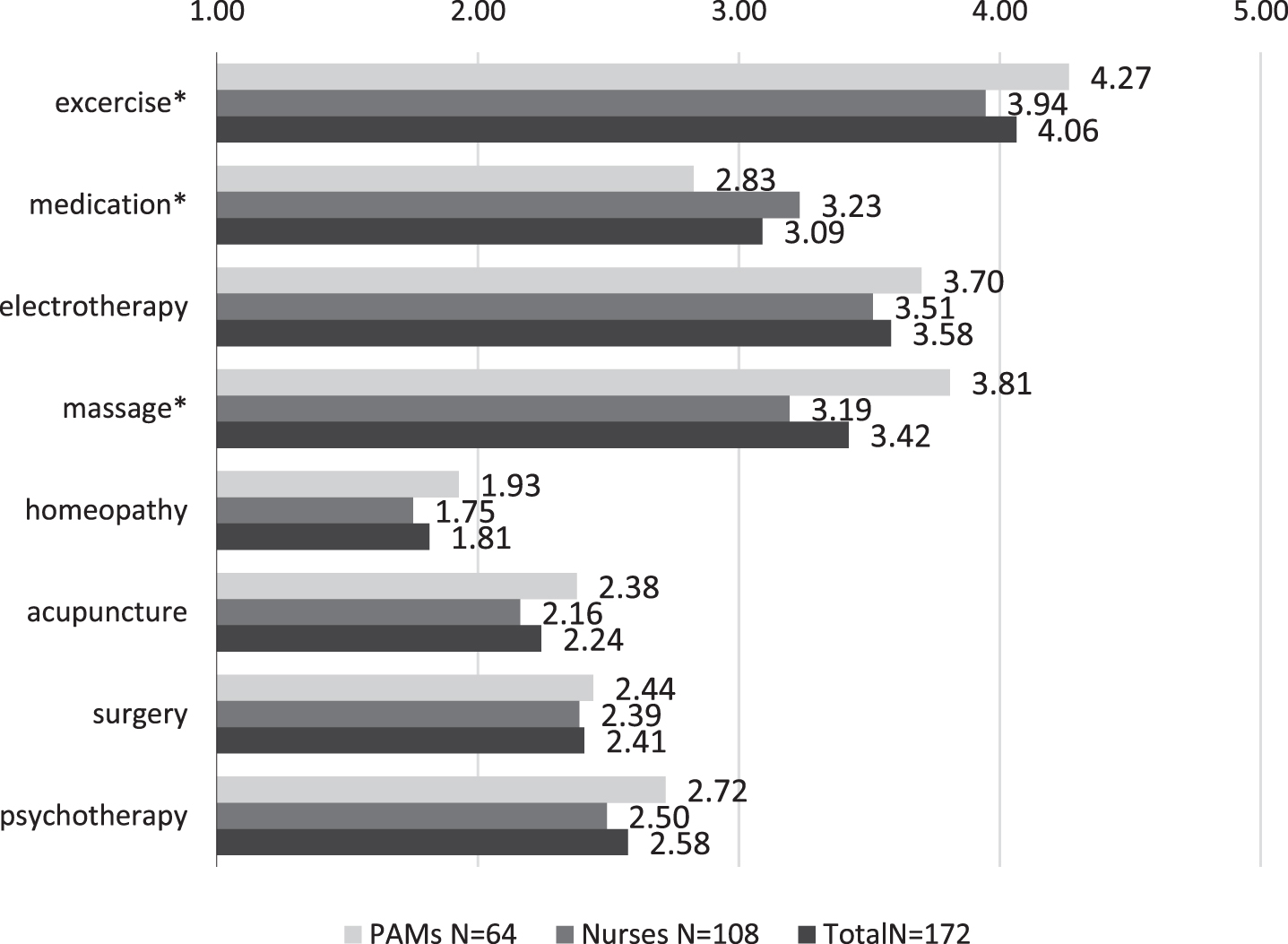
Opinions regarding the importance of treatment modalities for low-back pain in terms of professional background (answer options: 5 very important –1 useless, pointless;). The bars represent mean scores; SD-s ranged from 0.8–1.00. Significant differences are marked as: *p < 0.05.
There were some significant differences between the opinions of the nurses and the PAMs (see Fig. 1). PAMs evaluated exercise therapy (4.27 vs. 3.97; p = 0.024) and massage (3.81 vs 3.19 p < 0.01) as more important, while the nurses were more positive about drug efficacy (3.23 vs 2.83; p = 0.04). We did not find significant difference between the professions regarding the other treatment modalities.
We tested whether pain experience influenced the opinions regarding the importance of the therapies. We found that acceptance of drug therapy was higher among those experiencing moderate (3.12 SD = 0.76) or severe (3.11 SD = 0.99) pain compared to mild pain (2.85 SD = 0.76), however, this difference did not reach significance. No difference was found for the other therapies. (Fig. 2.)

Opinions regarding the importance of treatment modalities for low-back pain in terms of own pain experience (answer options 5: very important, –1 useless, pointless; The bar represents mean scores; SD-s ranged from 0.8–1.00). missing: N = 5 did not answer the question for pain, N = 6 did not answer the question for therapy Significant differences are marked as: *p < 0.05.
Years in health care work had only a weak association with the opinions regarding the treatment modalities surveyed. Based on Pearson’s correlation controlled for professional background, the importance attributed to medication significantly increased (r = 0.165 p = 0.029) and the importance of massage significantly decreased (r = –0.164 p = 0.027) with years of experience. No significant correlation was found for the other therapeutic procedures: exercise physiotherapy r = 0.014; electrotherapy r = 0.073; homeopathy r = 0.048, acupuncture r = 0.010 surgery r = –0.091; psychotherapy r = –0.087.
The nurses scored higher on FABQ total (43.7 vs. 36.1; p = 0.016), on FABQ_A (13.0 vs. 11.5; p = 0.024) and on FABQ-W (20.0 vs. 16.2; p = 0.021) than the PAMs. (see Table 4) 49.09 % (N = 72) of the nurses and 27.69 % (N = 18) of the PAMs met the criteria for high FABQ-A score (≥14) and 23.63% of the nurses N = 26 and 4.61% of the PAMs N = 3 had high FABQ-W score (≥29).
Fear Avoidance Beliefs Questionnaire (FABQ) scores according to professional background
Fear Avoidance Beliefs Questionnaire (FABQ) scores according to professional background
*N = 16 missing (8 nurses and 8 PAMs did not answer the FABQ questionnaire) FABQ-A = FABQ Activity; FABQ-W = FABQ Work; FABQ sum = all items. PAMs = physiotherapy assistants and medical masseurs.
Regarding the relationship between fear avoidance beliefs and personal pain experience, we found higher FABQ total scores among those who experienced severe or moderate pain compared to those who had mild pain (p = 0.076). This difference was significant for FABQ physical activity (p = 0.035) but not for FABQ work scores (p = 0.226) (see Table 5).
Fear Avoidance Beliefs Questionnaire scores in terms of strongest personal pain experience
*N = 25 missing (8 nurses and 8 PAMs did not answer the FABQ questionnaire; 8 nurses and 1 PAM did not answer the own pain intensity question).
We also tested the relationship between fear-avoidance beliefs and opinions on the importance of the treatment modalities. After controlling for professional background, we found significant positive correlation between the importance attributed to medication and all FABQ scores (r = 0.27; p < 0.001). The same tendency was also observed for surgery (r = 0.30; p < 0.001); no significant correlation was found for the other therapies (see Table 6).
Partial correlations, controlled for professional background, between FABQ subscales and opinions about the importance of the various therapies
N = 19 missing (8 nurses and 8 PAMs did not answer the FABQ questionnaire; 3 nurses and 1 PAM did not answer the therapies opinion) *p < 0.005.
Previous studies have shown that health care providers’ attitudes have an influence on their adherence to the guidelines and on the recommendations they give to their patients. In the present study, we investigated attitudes and beliefs regarding the management of LBP in a Hungarian sample of physiotherapy assistants and medical masseurs (together PAMs) and nurses, in the context of their professional and personal experiences with LBP. The participants came from various departments (internal medicine, emergency, rehabilitation, rheumatology, surgery, orthopaedics, primary healthcare etc.) across the country to attend postgraduate courses; therefore, this heterogeneous group might reflect general attitudes in these professional groups in Hungary.
Previous studies focused mostly on physicians and physiotherapists, while we found very limited data focusing on nurses and PAMs, although they might also influence the patients’ attitudes and self-management behaviours during their encounters.
Nurses and PAMs differ from physicians and exercise therapists regarding their training (secondary education compared to university degree) and their role in patient care (more time spent with the patients, less decision making power). The knowledge and tasks of these two groups also differ from each other. The nursing school gives a general knowledge of pathology and physiology, and limited knowledge on musculoskeletal disorders and pain management. PAMs training provides more specific knowledge about musculoskeletal disorders, while they learn less about drug therapies and general care. Nurses are more often confronted with the limitations experienced by the patients in their everyday lives (e.g., difficulties in mobility, dressing, bathing).
Our results partly confirmed our hypothesis regarding the influence of the professional background on attitudes. As expected, each professional group attributed greater importance to the therapeutic modalities they were providing: the PAMs group considered exercise therapy, massage and electrotherapy more important, while nurses had a more positive attitude to medication. Their opinions did not differ regarding surgery, psychotherapy or complementary and alternative medicine (CAM) interventions such as acupuncture or homeopathy, to which they attributed small importance. Those who had more years in practice attributed higher importance to medication and lower to massage. Although our study does not allow to make any assumption on causality, we hypothesize that older HCPs had less training with biopsychosocial approach. These findings are in accordance with the results of other studies. According to Fullen et al.’s review (2008) doctors’ specialty, demographic factors, personal beliefs and education influenced their attitudes towards acute LBP treatment. Petit et al.’s study found that the biopsychosocial approach (as compared to the biomechanical approach) was positively influenced by shorter length of practice, the collaboration with a multidisciplinary team and recent LBP-specific training [11].
We found only very small effects of personal pain experience on the attitudes and beliefs regarding LBP and its treatment. Medication was evaluated more important when the pain experience was more intense, while we did not find such correlation with exercise therapy despite our hypothesis (see Fig. 2). Those who experienced moderate or severe pain scored higher on the Fear Avoidance Beliefs Questionnaire (FABQ) compared to those with mild pain (Table 5). Higher FABQ scores were associated with a more biomedically oriented approach, attributing higher importance to medications and to surgery, however we found no correlation between FABQ scores and opinions about exercise therapy or the other treatments (Table 6). Neither we found significant association between FABQ scores and opinions about the need to start pain management (Table 3).
Nurses had higher FABQ scores than the physiotherapy assistants or masseurs (Table 4). Part of this can be that nursing is among the highest risk professions for LBP. This high risk can be explained by ergonomic factors such as the physical efforts required during their daily work, e.g. lifting of the patients, but also by psychosocial stress e.g. time pressure and emotional demands. The PAMs lower FABQ scores might be explained by their lower exposure to such requirements during their work.
In our sample the lifetime prevalence of LBP was 90%, and 46% reported current or recurrent low back pain (Table 1). This high prevalence is in accordance with international studies [30], and also with a recent study by Ofori-Attah and Németh among Hungarian nurses finding that 35.1% of those working day shifts and 27.1% of those working night shifts reported current musculoskeletal pain [31].
When we compared the results of the present study with a previous study among Hungarian LBP patients [16], we found that the FABQ work scores of the nurses were nearly as high as those of chronic LBP patients (FABQ-W LBP patients: 23,4; nurses: 20,0; PAMs: 16,2). The fear of physical activity scores were significantly lower in both HCPs groups than in chronic low-back patients (FABQ-A LBP patients: 19,1; nurses: 13,7; PAMs: 11,5).
Other studies on FABQ among nurses found similar results. In a Chinese sample of nurses FABQ-W was 20,15 in case of high LBP disability and 15,2 in case of low disability [14] French nurses reported even higher FABQ-W scores [24, 27], their FABQ-A score 15,85 was similar to ours [32] In a French sample of physicians the FABQ scores were lower than in the previous sample of nurses, the FABQ-W was 17,5 and FABQ-A was 9,6 [14]. An older survey that is still worth mentioning found the FABQ-W 18,4 and FABQ-A 14,6 in a sample of 1206 Belgian and Dutch nurses [33].
There are contradictory result regarding the influence of personal pain experience on fear avoidance beliefs. Some have found a connection [25], while other studies did not support this hypothesis [14]; in our study we found a weak relationship between FABQ scores and own pain intensity.
Overall, the opinions of our respondents were broadly in line with the current scientific evidence, as the respondents gave the highest importance to exercise therapy and did not consider CAM therapies to be very important in the treatment of low back pain. However less than half of them knew the exact criteria for initiating pain management. Our study confirmed in accordance with other studies that professional training has an influence on attitudes: health care providers are inclined to attribute higher importance to the treatment modalities that they are providing themselves, or to therapies with which they have more positive personal experience. The clinical relevance of our results is that own beliefs and fears might influence the encouragement of the patients to regain their physical activity as soon as possible, as recommended in the guidelines.
There are positive examples that fear avoidance beliefs of the HCPs might be modified by providing continuous education [13, 16]. The change in knowledge and attitudes of the therapists could influence the patient outcomes, decreasing the risk of developing long-term disability in more severe LBP cases [34]. Our research also brings on the need that in order to change attitudes, the discussion of personal experiences might be useful besides teaching the protocols during continuous education and training. These trainings could include the first step of a 5-step approach proposed by Nijs et al. that is self-reflection: The self-assessment and discussion of therapists own attitudes and beliefs regarding chronic pain could not only support a more evidence based thinking, but can also prepare therapists to assess their patients’ attitudes and beliefs [10]. Team discussions also could provide an opportunity to discuss the opinions about therapies delivered by the different professional groups.
Limitations
In our questionnaire we did not differentiate between acute and chronic pain, this might have some minor impact on the opinions regarding the usefulness of the various treatment modalities. We could not make a separate analysis for respondents working at different areas of health care because the sample size was too small.
This was a cross sectional study focusing only on the opinions so we can’t just assume that their attitudes have an impact on the HCP’s communication with the patients.
Strengths of the study
This study is the first study in Hungary (and as far as we could find information in the Eastern European region) examining the attitudes and personal LBP experiences in a general sample of nurses and PAMs working in various health care settings. Another strength of this research is that a combination of a standardized questionnaire on fear avoidance beliefs and original questions regarding attitudes were used to explore various aspects of personal experiences and opinions that might affect health-care professionals during their work with LBP patients.
Conclusion
In accordance with previous international studies, we found that professional background, work experience as well as personal experiences had small, but consistent influence on the attitudes of nurses, physiotherapy assistants and medical masseurs. These differences in opinions and beliefs regarding low back pain treatment modalities should be taken in consideration when working in a team. Our study draws attention to the importance of standardizing the information to be passed to the patients and to the need of discussing personal experiences and attitudes during continuous professional training, with special focus on the fear avoidance beliefs that are very common among the health care providers and might interfere with the encouragement of LBP patients to become physically active.
Conflict of interest
The authors declare that there are no conflicts of interest.