
Abstract
OBJECTIVES:
Shoulder pain is a common musculoskeletal disorder, which carries a high cost to healthcare systems. Exercise is a common conservative management strategy for a range of shoulder conditions and can reduce shoulder pain and improve function. Exercise classes that integrate education and self-management strategies have been shown to be cost-effective, offer psycho-social benefits and promote self-efficacy. This study aimed to examine the effectiveness of an 8-week educational and exercise-based shoulder rehabilitation programme following the introduction of evidence-based modifications.
METHODS:
A retrospective evaluation of a shoulder rehabilitation programme at X Trust was conducted, comparing existing anonymised Shoulder Pain and Disability Index (SPADI) and Patient-Specific Functional Scale (PSFS) scores from two cohorts of class participants from 2017-18 and 2018-19 that were previously collected by the physiotherapy team. Data from the two cohorts were analysed separately, and in comparison, to assess class efficacy. Descriptive data were also analysed from a patient satisfaction survey from the 2018-19 cohort.
RESULTS:
A total of 47 patients completed the 8-week shoulder rehabilitation programme during the period of data collection (2018-2019). The 2018-19 cohort showed significant improvements in SPADI (p 0.001) and PSFS scores (p 0.001). No significant difference was found between the improvements seen in the 2017-18 cohort and the 2018-19 cohort. 96% of the 31 respondents who completed the patient satisfaction survey felt the class helped to achieve their goals.
CONCLUSION:
A group-based shoulder rehabilitation class, which included loaded exercises and patient education, led to improvements in pain, disability and function for patients with rotator cuff related shoulder pain (RCRSP) in this outpatient setting, but anticipated additional benefits based on evidence were not observed.
Introduction
Shoulder pain is the third most common musculoskeletal disorder in primary care and carries a high cost to healthcare systems [1]. In the UK, costs attributable to shoulder pain are approximately $ 310 million per year [2]. The prevalence of shoulder pain ranges from 6% to almost 70% [3–5], and approximately 1.5% of people visit their general practitioner (GP) annually in the UK for a shoulder problem [6]. The pain and functional disability associated with shoulder disorders can have a significant impact on activities of daily living, and approximately 50% of patients report persistent pain after 12 months [7].
Rotator cuff related shoulder pain (RCRSP) is an umbrella term used to describe pain and loss of function of the shoulder, often during shoulder elevation and external rotation [8]. In patients with RCRSP, an exercise focused approach elicits successful outcomes equivalent to surgical intervention [8], and can reduce pain and improve function in the short-term, with moderate long-term improvements [9, 10].
Specific studies note the beneficial effects of strength training on reducing shoulder symptoms [11–13]. Lombardi et al. found that progressive resistance training significantly reduced shoulder pain and improved function in comparison to a control group receiving no intervention [11]. A 2011 RCT found that as little as two minutes of daily resistance training over a period of 10 weeks can reduce neck and shoulder pain [12]. A further RCT from 2016 compared a self-managed loaded single exercise programme versus usual physiotherapy, at the discretion of the physiotherapist, for patients with rotator cuff tendinopathy [13]. The study showed no significant difference in SPADI scores after three months, concluding that a single-exercise programme is comparable to usual physiotherapy treatment [13]. The number of participants in these studies ranged from 60 to 86 so caution should be applied in generalising findings to the wider population.
Patients with shoulder dysfunction are commonly referred to group exercise classes after an initial consultation with a physiotherapist. Class-based rehabilitation programmes, incorporating advice and education, have been shown to be cost-effective and offer psychosocial benefits, which promote self-efficacy and self-management of pain in a collaborative environment [14–18].
Despite evidence demonstrating the benefits of exercise classes in treating shoulder conditions, there is a lack of comprehensive research into rehabilitation class design and protocol, such as the duration and types of exercise. Many individual studies have methodological limitations, high risk of bias and clinical heterogeneity, resulting in limited generalisability to the wider population [8, 10].
Methods
The X Trust shoulder rehabilitation class has been running for a number of years and is aimed at reducing pain and functional limitations in people with RCRSP. Following an audit of the class in 2017-18, many areas were identified as requiring improvement. The class underwent significant modifications to facilitate greater efficacy, and to align more closely with principles of the ESCAPE (Enabling Self-Management and Coping with Arthritis Knee Pain through Exercise) programme, which has been shown to improve clinical outcomes in a safe and cost-effective way [18–20]. The educational component of the class was increased from five to eight topics, symptom monitoring was conducted using a traffic light system rather than a visual analogue scale, and the exercises were enhanced to ensure greater functionality rather than just focusing on the shoulder complex. A full list of the changes to the class can be found in Appendices 1–3.
In the 2018-19 programme, all patients who met the inclusion criteria were referred by a physiotherapist to the 8-week educational and exercise-based shoulder rehabilitation programme (Appendix 1–3). A Band 6 physiotherapist and therapy assistant or student physiotherapist led the class. The programme consisted of two main components: an educational seminar integrating self-management and coping strategies, and an exercise class in the format of a circuit programme consisting of strength, proprioception and range of movement exercises, carried out at 6 stations for 2 minutes each. Some participants received one-to-one physiotherapy prior to being referred and/or during the 8-week rehabilitation programme, however, these data were not collected.
As data had already been collected in 2017-18, it provided an opportunity to compare the results of participants who attended the 2018-19 class prior and after the change. The aim of this present study was to evaluate the effectiveness of the revised shoulder rehabilitation programme (2018-19), by comparing pre-class and post-class outcome measures. The secondary objective of the study was to evaluate the effectiveness of the revised programme (2018-19) compared to the programme prior to changes (2017–18).
A retrospective evaluation of the shoulder rehabilitation programme at X Trust was carried out in May 2019, using data previously collected by the physiotherapy team leading the shoulder programme. Shoulder Pain and Disability Index (SPADI) and Patient-Specific Functional Scale (PSFS) pre- and post-class scores were collected by the physiotherapy team, as well as demographic data including age, sex and diagnosis. Both outcome measures were considered reliable, reproducible and valid [21–23]. The physiotherapy team also designed a patient satisfaction survey using the Likert Scale, which was completed by patients at the end of their 8-week rehabilitation programme. Existing anonymised SPADI and PSFS data from the previous class audit from 2017-2018 collected over approximately eight months was made available to the research team. Data collection took place between August 2018 and March 2019 to allow for similar data collection periods for the evaluation process.
Data was analysed using SPSS Statistics (25.0 for Windows; SPSS Inc, Chicago, IL). Data was normally distributed. Descriptive data were shown as mean and standard deviation (SD). Differences between groups were shown using a mean with 95% confidence interval. The data analysed were parametric data, where within group analysis was conducted using the two-tailed paired t-test and between group analysis was conducted using independent t-test. Statistical significance was considered at P < 0.05 and Cohen’s effect sizes (pre-mean –post mean/SD) were calculated using an online calculator [24]. The minimal clinically important difference (MCID) for the SPADI was considered 8 points [21] and for the PSFS was 1.16 points [22]. Descriptive statistics were used to analyse the patient satisfaction survey.
Results
Fifty-two patients met the inclusion criteria and were referred to the programme during the period of data collection in 2018-19. A total of 47 patients completed the 8-week programme during this time: five patients were excluded from data analysis due to incomplete data, reason for non-completion was not disclosed by the physiotherapy team conducting the class. Participant flow is shown in Fig. 1. Of the 47 patients included, 43 completed a PSFS pre- and post-class. Baseline characteristics are shown in Table 1. All patients had a diagnosis of RCRSP. More women (n = 31) were referred to the class than men (n = 12).
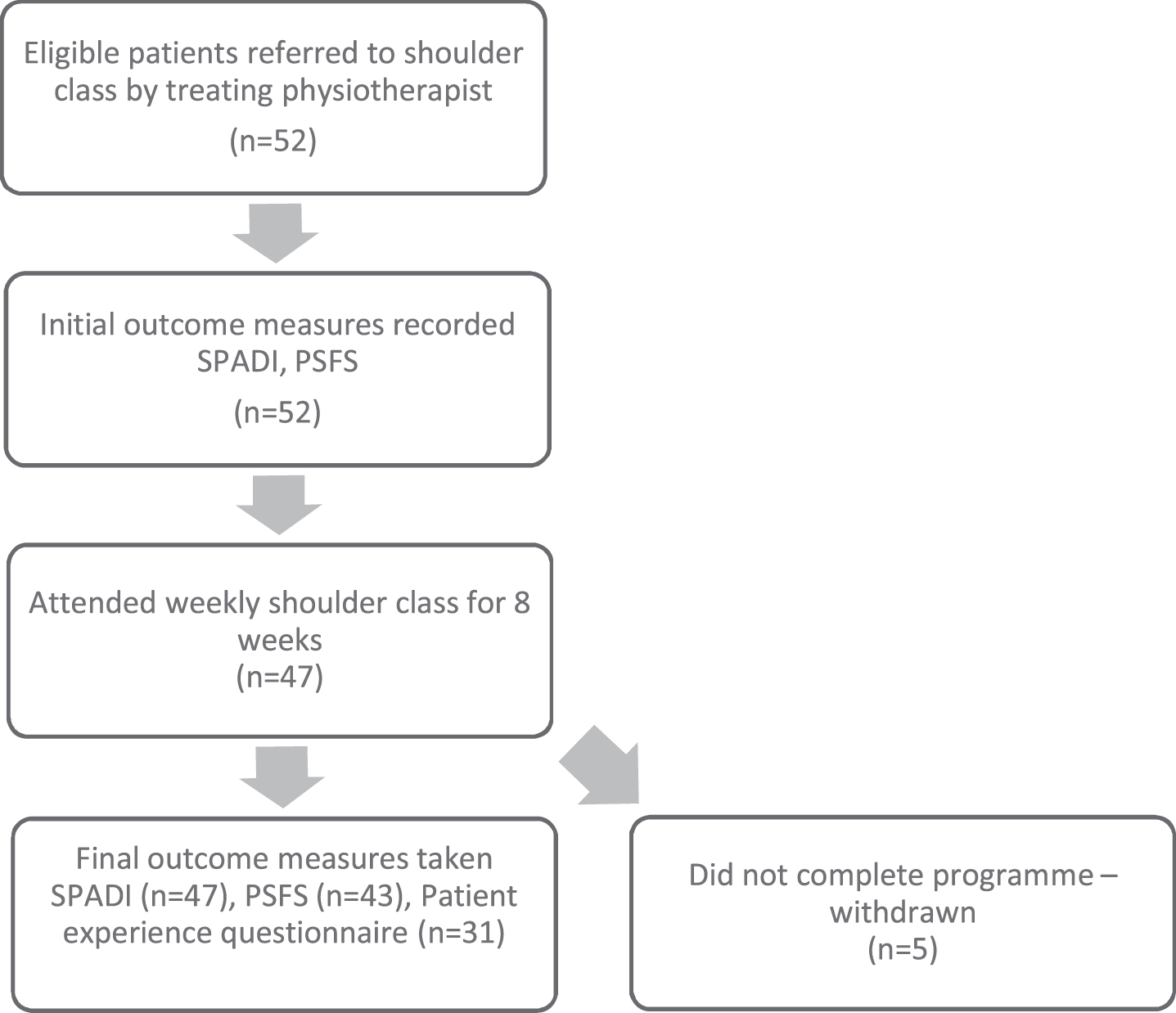
Participant flow for the 2018-19 shoulder class group.
Baseline characteristics of patients who completed the 2018-2019 shoulder class
The 2018-19 group showed significant improvement in SPADI scores as shown in Graph 1. Significant improvement was seen in both subcategory domains. The SPADI pain score reduced from 60.26 (pre-class) to 46.94 (post-class) representing a mean change of 13.32 [6.10–20.54, 95% CI], (p < 0.001, Cohens d = 0.67). Similarly, the SPADI disability domain significantly improved, from 49.49 (pre-class) to 36.12 (post-class), a mean difference of 13.38 [7.76–18.99, 95% CI], (p < 0.001, Cohens d = 0.63). The magnitude of change between domains was not significant.
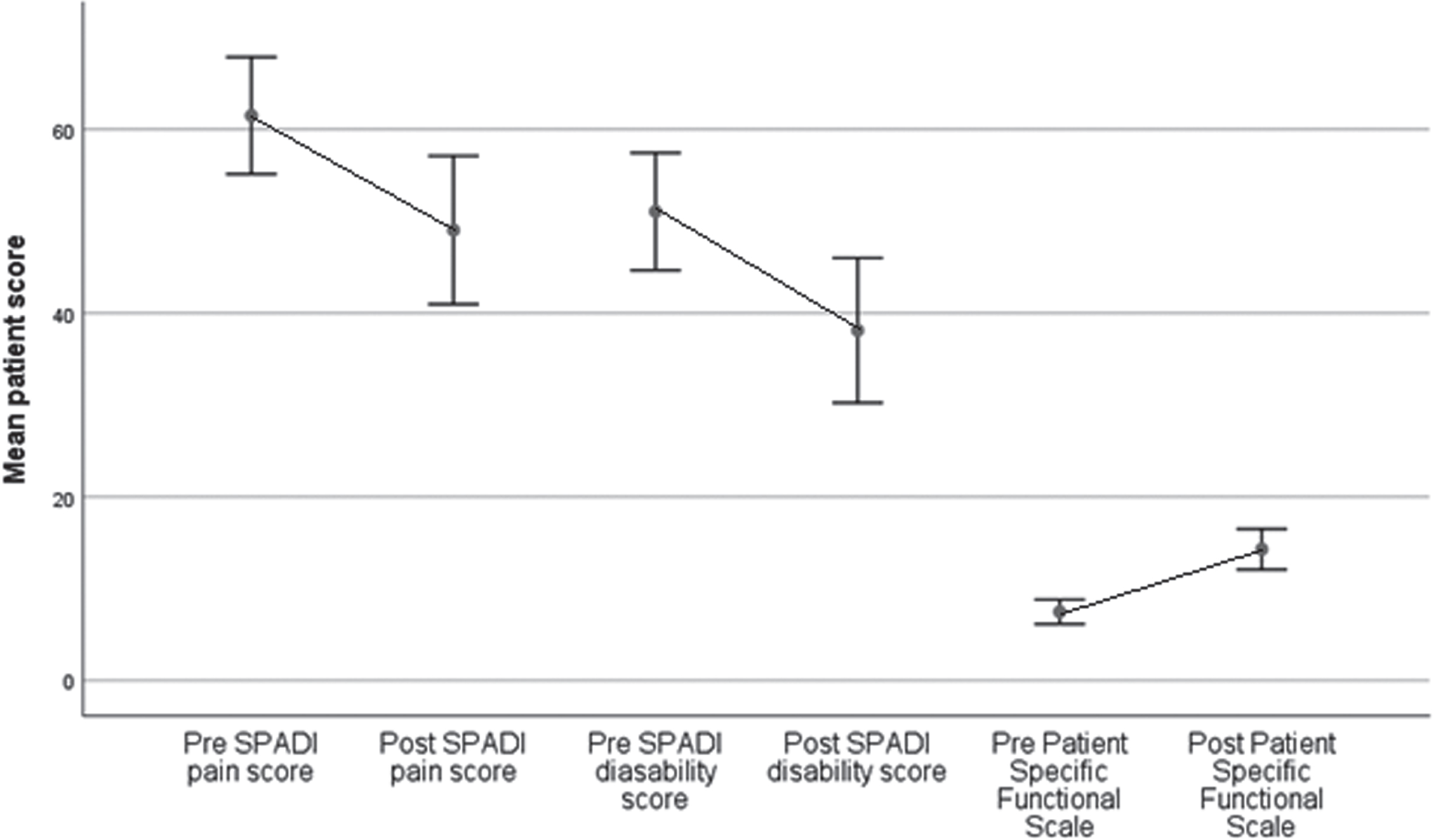
Mean SPADI and PSFS scores pre and post shoulder class. Error bars indicate 95% confidence interval of score mean. SPADI pain is calculated as: score/50*100, SPADI disability is calculated as: score/80*100.
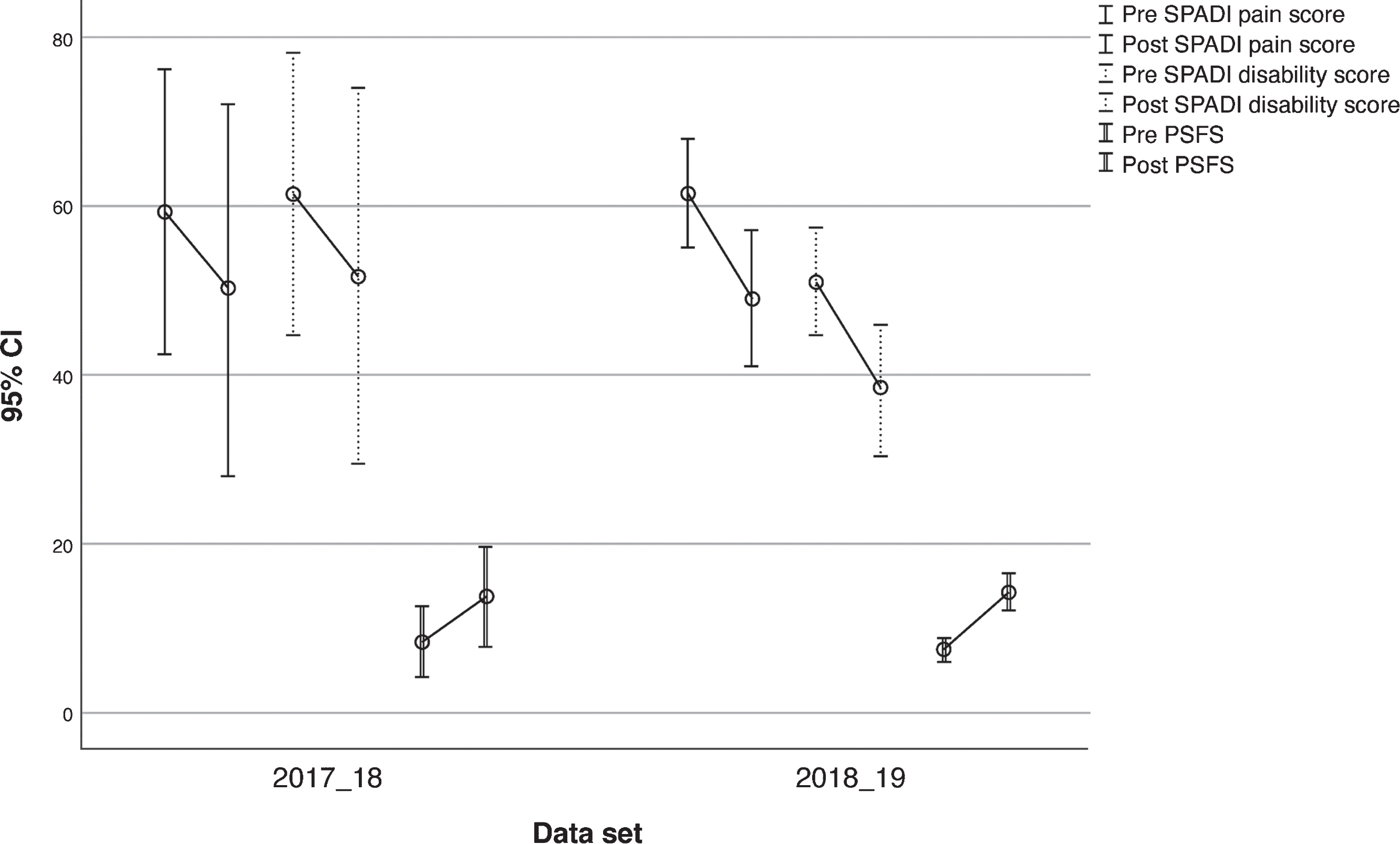
Comparison of SPADI and PSFS data by programme year.
Significant change was recorded for PSFS scores indicating improvement in activity limitation and functional outcomes, with a mean increase of 5.66 [5.07–8.55, CI 95%], (p < 0.001, Cohens d = 0.98).
Complete pre-post data was available from 48 participants in the 2017-18 class. The 2017-18 data showed SPADI pain reduction from 66.00 (pre-class) to 51.80 (post-class) representing a mean change of 14.15 [5.20–23.10, 95% CI], (p < 0.01, Cohens d = 0.67). Similarly, the SPADI disability improved from 50.42 (pre-class) to 39.81 (post-class), a mean difference of 11.61 [0.84–22.37, 95% CI], (p < 0.05, Cohens d = 0.63). The combined data set (2017–2019) (n = 95) showed significant improvements in both domains: SPADI pain mean change of 14.32 [10.03 –18.61, 95% CI], (p < 0.001, Cohens d = 0.67), and SPADI disability of 15.53 [11.14–19.93, 95% CI], (p < 0.001, Cohens d = 0.59). No significant difference was seen between pre- and post-SPADI scores comparing 2017-18 and 2018-19 programmes (p = 0.335). The magnitude of change was also not found to be significant comparing 2017-18 and 2018-19, so neither protocol can be said to be superior (mean change in SPADI pain score between groups (p = 0.799), mean change in SPADI disability score between groups (p = 0.544)). No significance was found in PSFS in 2017-18 pre-post scores (8.33 (pre)- 13.66 (post), p = 0.55). Neither was there a significant difference between the mean change of PSFS 2017-18 to 2018-19 (p = 0.498). Demographic data was not collected with the 2017-18 data, so it is not possible to compare mean age and any differences in the sex of participants between groups.
Tertiary objective–Patient satisfaction survey
Thirty-one participants completed the patient satisfaction survey post class; questions and responses can be seen in Fig. 2. 96.7% of responders to the patient satisfaction survey either agreed or strongly agreed that the class helped achieve their goals (Q.1). 93.5% agreed/strongly agreed that the class had improved activities of daily living. Questions 6 and 12 looked at self-management, 93.6% agreed/strongly agreed that they have increased their level of exercise and 87.1% agreed/strongly agreed that they had the information and skills to carry on independent of the class. Fewer participants completed questions 7–12 as the survey was printed on double-sided paper, and some participants did not turn over the page. The lowest response was seen for question 13, which looked at likelihood of recommending the class to other participants. All responding participants (n = 13) stated ‘agree’ or ‘strongly agree’. This question was not included in an earlier iteration of the document given to patients by physiotherapy staff post-class.
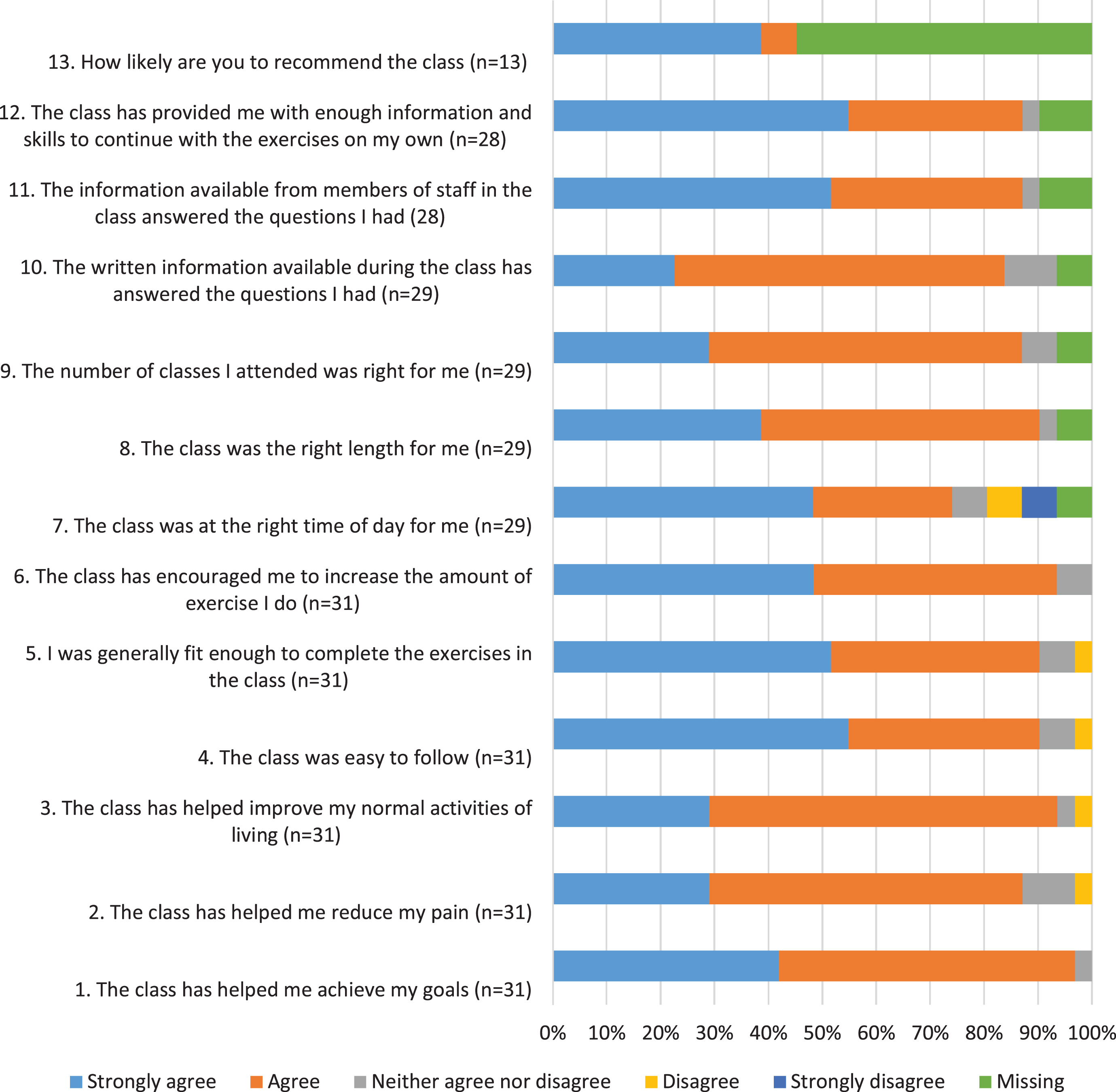
Results of the patient satisfaction survey.
The first aim of this evaluation was to compare patient SPADI and PSFS scores before and after the 8-week intervention. The cohort of 2018-19 showed significant improvements in pain, disability and function upon completion of the last class; total SPADI scores improved by an average of 13.3 points with a moderate effect size [24] and notably 29 of the 42 participants achieving more than reported MCID [21]. The changes in PSFS (5.66) had a large effect size [24] and 22 of the 43 participant exceeded the MCID [22]. The findings of this evaluation were similar to those of a study by Littlewood and colleagues [13] where an improvement of 12.4 points in total SPADI score was achieved with a single loaded exercise to treat RCRSP. Significant results from this evaluation and a mixed methods study in 2012 [25] help to support the use of loaded exercises in shoulder treatment.
The second aim of the evaluation was to compare outcomes from the 2017-18 class and the 2018-19 class to determine whether the modifications outlined in Appendix 1 led to greater improvements. No significant difference in the effectiveness of the 2017-18 class versus the 2018-19 class was found; both iterations of the class were as effective in improving function, pain and disability in patients with RCRSP. Thus it can be concluded that group exercise classes are beneficial for people with RCRSP, independent of the type of exercise and education.
Systematic reviews investigating exercise-focused interventions for this patient population lack consensus on the frequency, dosage i.e. sets/repetitions, nature of the exercises, exercise intensity and appropriate levels of activity outside the class [26]. This evaluation suggests that an exercise circuit of 2-minute intervals can improve patient outcomes, and the use of a traffic light system to monitor symptoms may allow for an individualised and patient-centred approach. However, further research is required to explore these benefits fully.
A major strength of this evaluation, comparable to that of Hurley and colleagues’ ESCAPE study relating to knee pain, [18] was the inclusion of loaded exercises and education in a real-life, pragmatic setting of the outpatient department. Variables such as staff turnover and clinical experience, departmental budgets, location and class timings, mean that whilst the results of this evaluation only provide meaningful conclusions within this local context, other settings may draw parallels to inform practice within their own specific clinical environments.
The inclusion of an educational component, similar to the ESCAPE class [18], was designed to provide reassurance, introduce coping strategies, prevent fear avoidance and improve self-management. There is mounting evidence that identifies not only the physical but also the psychological, cognitive and social aspects of treating shoulder pain [6, 28].
The patient satisfaction surveys were designed to provide insight into patient’s perceptions of self-management, class structure and class scheduling. Overall, responses to the survey were generally positive, the majority of respondents felt that the class helped to achieve their goals, improve their activities of daily living and encouraged them to exercise more. Due to inconsistent data collection, it was not possible to analyse the relationship between patient satisfaction and SPADI and PSFS scores, making it difficult to draw any further conclusions.
The class may have facilitated changes in health beliefs and improvements in self-management, as well as offering a supportive environment to foster motivation and learning from peers [14]. However, caution must be taken when claiming clinical significance without further studies specifically designed to investigate the mechanisms involved. It is important to note that the act of an intervention, regardless of the mechanism, may lead to improved outcomes, i.e. the placebo effect [29]. Shoulder pain can also resolve with the natural progression of healing. Positive outcomes may therefore be a result of both or either of these phenomena.
More women than men were referred into the 2018-19 cohort. Rotator cuff pathology is more prevalent in women compared to men and this may be due to biological distinctions in anatomy, hormones, neuromuscular control, strength and aerobic capacity, which make women more vulnerable to certain musculoskeletal disorders [30]. Further research is required to explore the role of sex and gender differences regarding RCRSP.
Limitations and recommendations for future research
This evaluation was limited by a lack of consistency in the data collection. Although the findings were strengthened by a between-group comparison, baseline characteristics and sociodemographic data relating to participant age, gender and pathology were not captured in the 2017-18 data set; it is therefore not possible to determine whether the patients in the 2017-18 class and the 2018-19 class were similar at baseline, which exposes the findings to confounding factors. There is strong evidence to suggest that body mass index (BMI), chronicity of pain, level of physical activity, self-efficacy, anxiety and depression at baseline are linked to poor adherence and treatment outcomes within musculoskeletal outpatient settings [31]. Future evaluations will benefit from including this data to better understand the mechanisms influencing improvements in function, pain and disability in patients with RCRSP.
Fewer participants completed the PSFS compared to the SPADI outcome measure. This was due to time constraints within the class, as the PSFS required a physiotherapist to help the patient to list the activities that were impacted by their RCRSP [32], whereas the SPADI was self-administered. Additional time allocated at the end of the class would have ensured more comprehensive data collection.
Class attendance and outcome measures were not linked to participants and adherence to exercise outside of the class was not monitored, making it difficult to draw generalisable conclusions. The evaluation was also limited by lack of long-term follow-up with participants after completion of the 8-week programme. Future research will benefit by conducting a qualitative analysis of patient perspectives to identify potential barriers to treatment and to determine their effects on long-term self-management.
Although the hospital services a diverse population of 1.3 million people, data collection focused on one clinical site and thus limited generalisability. It is recommended that future audits collect data from multiple sites to ensure greater representation of the wider population.
It was also difficult to identify whether improvements were derived from the education component alone or the supervised exercises. Most participants will have received one-to-one physiotherapy prior to being referred and/or during the 8-week rehabilitation programme; this individual treatment may have influenced the results. An adequately powered randomised control trial is required to compare the benefits of group exercise classes and/or group education versus usual one-to-one physiotherapy for people with RCRSP.
Conclusion
This evaluation investigated the efficacy of a shoulder rehabilitation programme and compared the results to patient outcomes from the previous cohort. Despite modifications to the class, both rehabilitation programmes were shown to be equally effective with improvements in pain, disability and function. The findings support the continued use of group-based exercises combined with patient education for the treatment of RCRSP in this outpatient setting. Future investigations should include multiple site evaluations, long-term patient follow-up and further analysis of patient experience.
Conflict of interest
The authors declared no competing interests.
Ethical considerations
An application for ethical approval was made to the Faculty of Health and Social Care Research Ethics Committee (Kingston University and St George’s University of London) and it was deemed that ethical approval was not required for this evaluation.
Funding
This evaluation has no financial support.