
Abstract
BACKGROUND AND PURPOSE:
Fractures of the proximal humerus are characterised by slow recovery and ongoing disability. We aimed to describe the recovery of patients referred to community physiotherapy after proximal humeral fracture and determine if activity thresholds based on the Shoulder Function Index (SFInX) could inform physiotherapist decision-making.
METHODS:
Using a prospective observational cohort design, patients referred to community rehabilitation for physiotherapy were assessed for activity limitation (SFInX, DASH), quality of life (EQ-5D), pain levels (VAS), global rating of change, and shoulder range of movement at weeks 0, 6, 12 and 26. A focus group explored treating physiotherapists’ perceptions of using the SFInX. Characteristics of participants meeting SFInX clinically meaningful activity thresholds (+Δ17 units, score ≥73 units) were compared to those who did not.
RESULTS:
Participants (n = 38, mean age 78 years, 29 women, 29 conservatively managed) commenced physiotherapy a median of 12 (min 4, max 62) weeks after proximal humeral fracture and received a median of 8 (min 3 max 17) sessions over 8 weeks. N = 18 achieved +ΔSFInX ≥17 units by week 6. N = 15 achieved SFInX ≥73 units by week 26. Shoulder flexion range of 112° predicted +ΔSFInX ≥17 units at week 6 (AUC 0.74, 95% CI 0.58 to 0.90). Physiotherapists reported not basing management decisions on the SFInX.
CONCLUSIONS:
Patients after proximal humeral fracture make clinically meaningful improvements in shoulder activity after referral to physiotherapy. Decision-making based on SFInX activity thresholds or achievement of shoulder flexion of at least 112° may be informative but physiotherapists preferred making decisions based on individual goal-attainment.
Introduction
Proximal humeral fractures are common in people over 50 years [1–3]. Recovery of function is often slow and many patients experience ongoing disability [4–6]. For these reasons, people with proximal humeral fracture are often referred to a physiotherapist in outpatient or community rehabilitation programs.
A key aim of rehabilitation after proximal humeral fracture is to restore shoulder activity, that is the ability to do daily tasks involving the upper limb. However, physiotherapists providing rehabilitation face a number of measurement-related issues. First, the difficulty of selecting an outcome that is suitable to measure activity limitation in this population. Existing scales commonly used such as the Constant score [7] and the American Shoulder Elbow Surgeons (ASES) Shoulder Score [8] are multidimensional, assessing pain, function, range of movement and strength and combine it into a single score, making it difficult to determine activity limitation [9]. Second, because of the slow recovery often observed in these patients [4–6], it may be difficult for physiotherapists to make an informed decision about when to stop active rehabilitation; that is, to decide when patients have restored an acceptable level of shoulder activity after fracture.
The Shoulder Function Index (SFInX), an evi-dence-based outcome measure specifically designed to measure activity limitation in people recovering after proximal humeral fracture, may assist decision-making by physiotherapists. The SFInX is a 13-item clinician-observed, unidimensional outcome measure of shoulder function, as demonstrated using Rasch analysis [10]. It has demonstrated high levels of test-retest reliability and evidence of construct validity [11, 12]. Based on a sample of 92 adults recovering from proximal humeral fracture, an improvement of 17 points in the SFInX scale (0 to 100) equates to a moderate level of clinical improvement. An improvement of 12 points on the SFInX equates to a minimal clinical important difference (MCID) [11, 12]. More than 80% of participants reporting a moderate improvement (based on a moderate clinically important difference) achieved a SFInX score of at least 73 points, meaning they could successfully complete at least 9 of the 13 items on the SFInX. Therefore, monitoring outcomes during rehabilitation after proximal humeral fracture with the SFInX could provide clinicians and patients with a way of determining if they have made a clinically meaningful level of recovery by achieving this activity threshold. A patient achieving this level of shoulder activity could be assumed independent in many daily activities [11, 12]. Since the SFInX is administered by clinicians, another consideration is clinician opinion about using this outcome measure in clinical decision-making.
The aims of this study were to: Describe the characteristics and recovery trajectory of a cohort of people referred for physio-therapy rehabilitation after a proximal humeral fracture. Describe the proportions and differences be-tween those who meet and do not meet the specified activity threshold of 73 points and an improvement of 17 points on the SFInX. Explore physiotherapist opinions about using the SFInX to guide decision-making on discharge planning and patient management.
Methods
Design and setting
The study design was a prospective, single-group, observational study of a cohort of people receiving rehabilitation after proximal humeral fracture; and included a qualitative analysis exploring the perceptions of their treating physiotherapists. Ethics approval was obtained from the health service and university ethics committees. All participants completed written informed consent prior to participation. The study is reported with reference to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations [13]. The study was conducted in the community rehabilitation program in a large metropolitan health network in Melbourne, Australia from September 2015 to June 2019. The community rehabilitation program offers short-term goal-directed rehabilitation from a multidisciplinary team. Therapy is delivered either individually and /or in a group setting, in the centre and/or in the home environment depending on the person’s needs.
Participants
Patients were included if they were aged at least 18 years and were referred to the community rehabilitation program for active rehabilitation led by a physiotherapist following a proximal humeral fracture, regardless of the type of orthopaedic fracture management. Active rehabilitation was defined as being permitted to commence active shoulder movement after orthopaedic fracture management. Patients with impaired cognitive functioning were included provided they fulfilled other inclusion criteria. Cognitive functioning was assessed with the Short Portable Mental Status Questionnaire [14], with a score of at least 6 out of 10 indicating intact or mildly impaired cognitive functioning. If a participant had more than a mild level of cognitive impairment, a responsible person was asked to provide written informed consent and the participant invited to provide assent. Participants who did not speak English as their first language were included with use of interpreter services consistent with usual practice at the health service. Patients were excluded if they had confounding medical conditions affecting their ability to participate in an upper limb rehabilitation program (for example, a severe stroke with hemiplegia affecting the arm with the fracture). The physiotherapists who provided treatment for the study participants, and who had used the SFInX were included in the qualitative component of the study.
Intervention
Participants received usual-care physiotherapy management at the community rehabilitation program. Usual care was administered either in the rehabilitation facility (centre-based) or in the participant’s home (home-based). The content and frequency of the physiotherapy interventions was at the discretion of the treating physiotherapist. Physiotherapy was usually weekly, and typically included, but was not restricted to, goal-directed exercise training and education/home advice.
Outcomes
All participants were assessed by their treating physiotherapist at baseline (week 0), week 6, week 12 and week 26. The primary outcome was the SFInX, a 13-item unidimensional measure of shoulder function (activity) for people recovering from proximal humeral fracture [10]. The SFInX typically takes 5 to 7 minutes [12] to complete. Several everyday pieces of equipment are used to make testing functional and to simulate daily activities: a cup, objects of 1.5, 3 and 6 kg, a ball (for example, soccer ball) and a (shopping) bag. A user’s manual and scoring instructions are freely available [10]: https://sfinx.blogs.latrobe.edu.au/
Secondary outcomes
Disabilities of the Arm, Shoulder and Hand (DASH) [15], a multidimensional 30-item patient-reported questionnaire, was used to assess disability in the upper limb. Items relate to daily activities (21 items), symptoms (6 items) and social/role function (3 items), and participants are asked to reflect on ‘the past week’. Total scores range from 0 to 100, where 0 indicates ‘no disability’ and 100 ‘totally disabled’. A DASH score of < 15 can be classified as good (no or minimal problems), 15 to 40 moderate, and > 40 as poor [16]. The scale has demonstrated acceptable levels of convergent validity with other shoulder outcome scales with a MCID of 13 in people with proximal humeral fracture [17].
Global rating of change was assessed using a 15-point ‘overall perception of change’-scale [18]. The scores range from ‘-7 a very great deal worse’ through ‘0 no change’ to ‘+7 a very great deal better’. Interpretation of scores followed recommendations with scores of 0 and±1 considered ‘no change’, scores of±2 and±3 considered a ‘small change’, scores of±4 and±5 considered a ‘moderate change’, and scores of±6 and±7 were considered a ‘large change’.
Pain level was assessed using a 0 (no pain) to 10 (worst possible pain) numeric pain visual analogue scale (VAS) with participants asked to place a mark on the scale that best described their average shoulder pain over the previous week.
Range of movement of elevation (shoulder flexion, shoulder abduction) and shoulder external rotation was assessed using a universal goniometer according to standard instructions [19, 20]. Shoulder external rotation was assessed in standing, with the shoulder in neutral flexion, elbow flexed to 90 degrees with forearm in mid-pronation [20].
Health-related quality of life was assessed using the EuroQoL questionnaire (EQ-5D-3L) and visual analogue scale (EQ-VAS) [21]. The EQ-5D-3L rates five domains of health: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Scores were converted into a utility index score using Australian weights [22]. A change in the EQ-5D utility index score of half a standard deviation was considered clinically important (MCID) [23].
The number of physiotherapy treatment sessions were monitored, as were the number and type of any other interventions (e.g. occupational therapy), and the demographic characteristics of the participants (e.g. age, sex, type of fracture, initial management). To help describe the sample, falls risk at initial assessment was based on the falls risk assessment tool used at the health network, Falls Risk for Older People in the Community (FROP-Com) [24].
After completion of the clinical study, a focus group was conducted with the physiotherapists who were involved with treatment and assessment of the patient participants. The use of a focus group was appropriate as we aimed to understand interpretations of a select group of people, in this case physiotherapists, on a specific issue, the use of the SFInX in the management of people recovering from proximal humeral fracture [25]. Physiotherapists who had treated at least two participants in the study were invited to participate in the focus group by their manager. An experienced moderator facilitated the focus group with assistance from a member of the research team. A series of questions were used to guide and generate discussion about the SFInX and how useful it was as a decision-making tool to guide clinician practice. The key questions were: 1. How do you use the SFInX to guide your treatment? 2. What’s difficult about using the SFInX when managing your patients with shoulder conditions? 3. What do you like about using the SFInX when managing your patients with shoulder conditions? 4. Would you continue to use the SFInX? Explain why; 5. How has the SFInX been useful in discharge planning? The focus group was audiotaped and transcribed verbatim. In addition, field notes were taken by the member of the research team.
Analysis
A descriptive analysis was completed of participants who achieved the activity thresholds, their health-related quality of life and of the number and duration of treatment sessions they received. Based on inspection of the scatterplots, skewed distributions were described as medians and ranges in the descriptive tables. Other continuous distributions were described as means and standard deviations. Changes from week 0 to each of the other time points (i.e. weeks 6, 12 and 26) were quantified as mean differences and 95% confidence intervals derived from paired t-tests. The difference between participants who achieved the SFInX thresholds of a 17-point improvement and/or a score of 73 points and those who do not were compared using independent t-tests. If assumptions were not fulfilled then degrees of freedom were adjusted. T-tests are robust for violation of assumptions [26] and allow for easier comparison with other studies. Consistent with recommendations, adjustments for multiplicity were not made as the study was exploratory and there was no universal hypothesis [27]. Receiver operating curve analysis of the variable that best discriminated those achieving activity thresholds was completed with discriminative ability expressed as the area under the curve (AUC) [28]. Optimal cutoffs were determined using the Youden index [29]. Assuming a large effect size (d = 1.0), and twice as many participants achieving the activity threshold as not (allocation ratio = 2), a total of 38 participants were estimated to be required for power of 0.80 at an alpha level of 0.05. Consistent with intention to treat principles, all available data were used for analyses. Quantitative data were analysed with IBM SPSS version 25 [30].
Qualitative analysis of the focus group data commenced with two researchers independently reading and re-reading the transcript along with session notes. The transcription text was subsequently coded manually and the codes were organised into themes, using an inductive approach. An interpretive description framework was used to gain an understanding of the views of physiotherapists and to generate knowledge that could be applied in clinical practice [31]. The two researchers discussed the codes and came to a consensus on the overall themes and related subthemes. A third researcher provided feedback on the interpretation of the data and the themes derived from the data.
Results
Patient characteristics
Of 54 potentially eligible patients, 38 participants were recruited (Fig. 1). The most common reasons why patients were excluded were concurrent medical conditions (e.g. stroke) affecting the same side as the side of the proximal humeral fracture. Of the 38 participants, 4 were lost to follow up by week 26. Of these 4 participants 2 fell out of contact, 1 was waiting for placement due to a general decline in health, and 1 was diagnosed with an un-united fracture at week 20.
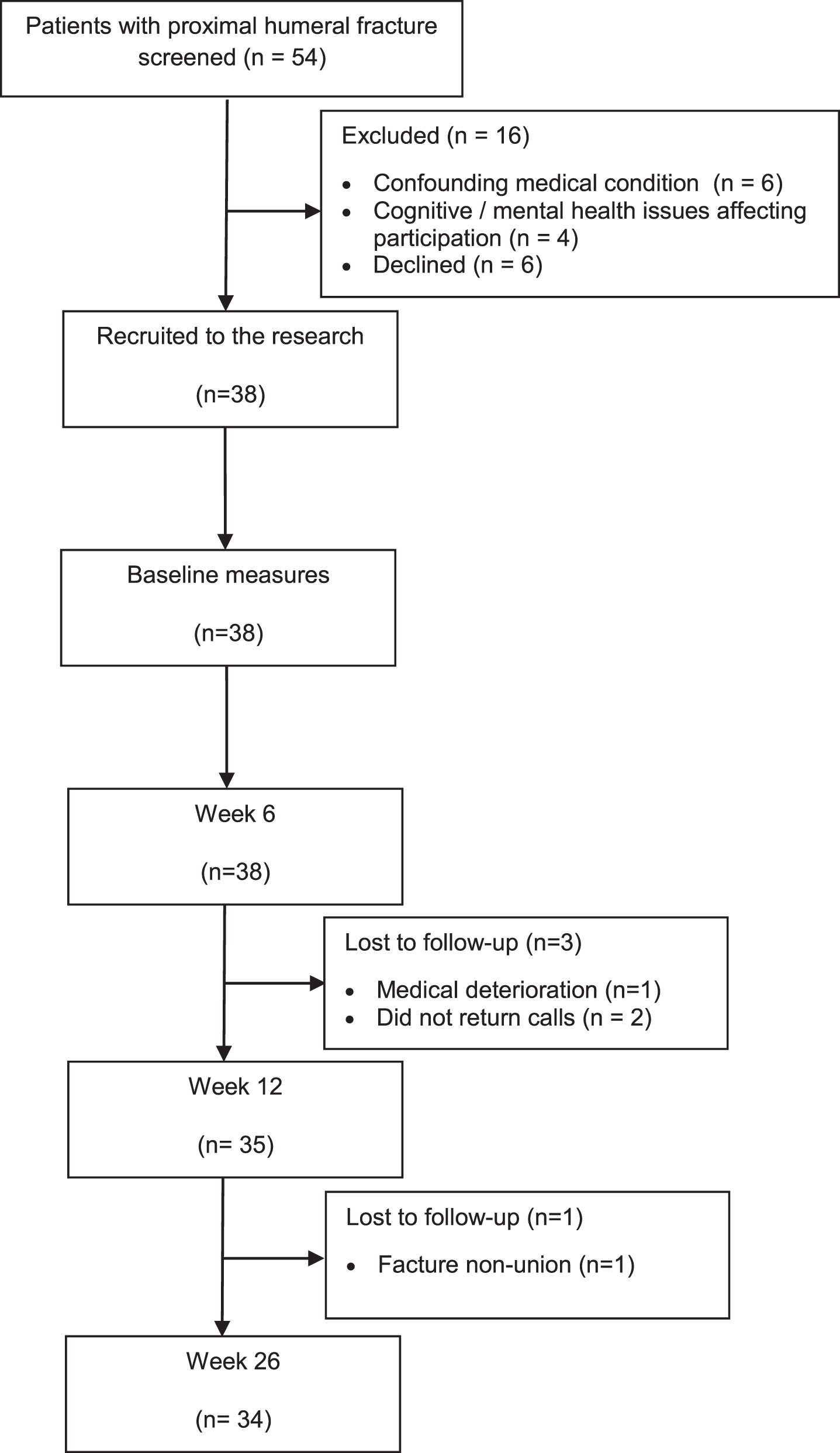
Flow of participants through study.
The 38 participants (9 men and 29 women) lived independently in the community and had a mean (standard deviation (SD)) age of 78 (SD 10) years (Table 1). Ninety-two per cent (35 of 38) occurred as a result of a fall and 76% (29 of 38) were managed conservatively. Ninety-two per cent of participants (35 of 38; 92%) presented with multiple comorbidities; hypertension (n = 24), cardiac comorbidities (n = 13) and osteoarthritis (n = 12) being the most common. Twelve participants were assessed as having a high falls risk on the FROP-Com tool. One participant had more than a mild impairment in cognitive function on screening, thus requiring a responsible adult to consent on their behalf. No participant required the use of a language interpreter.
Baseline characteristics of n = 38 participants
Participants commenced active shoulder rehabilitation with a physiotherapist at a median of 12 (min 4, max 62) weeks after fracture (Table 1), and had a median of 8 (min 3, max 17) sessions with a physiotherapist at home or in the rehabilitation centre over the following 8 weeks (Table 2). Eighty-nine per cent (34 of 38) were discharged from physiotherapy by 12 weeks and all were discharged by 26 weeks. Fifty-five per cent of participants (21 of 38) received other therapy services; of these, 39% (15 of 38) received occupational therapy.
Therapy details during community rehabilitation
There were large improvements in shoulder acti-vity from week 0 to week 6, with smaller improvements observed at week 12 and week 26 (Table 3, Fig. 2). The lower band of the 95% confidence interval of the change in SFInX exceeded the MCID at week 6 indicating clinically important changes. There were also large increases in the range of shoulder movement from week 0 to week 6 with smaller improvements observed until week 26. At week 6, the average change in health-related quality of life exceeded the MCID (>0.5 baseline SD), and global rating of change (mean 3.6 units, SD 2.4) was consistent with a perception of moderate improvement. Mean DASH scores improved from poor to moderate from week 0 to week 6, with a smaller improvement observed at week 12 and little improvement between week 12 and week 26. The average change in DASH scores was less than the MCID at week 6; the lower band of the 95% confidence interval exceeded the MCID at week 12 indicating clinically important changes in shoulder disability at that time.
Mean (SD) of shoulder function, quality of life, pain level and range of motion at each time, and mean difference (95% CI) across time
Mean (SD) of shoulder function, quality of life, pain level and range of motion at each time, and mean difference (95% CI) across time
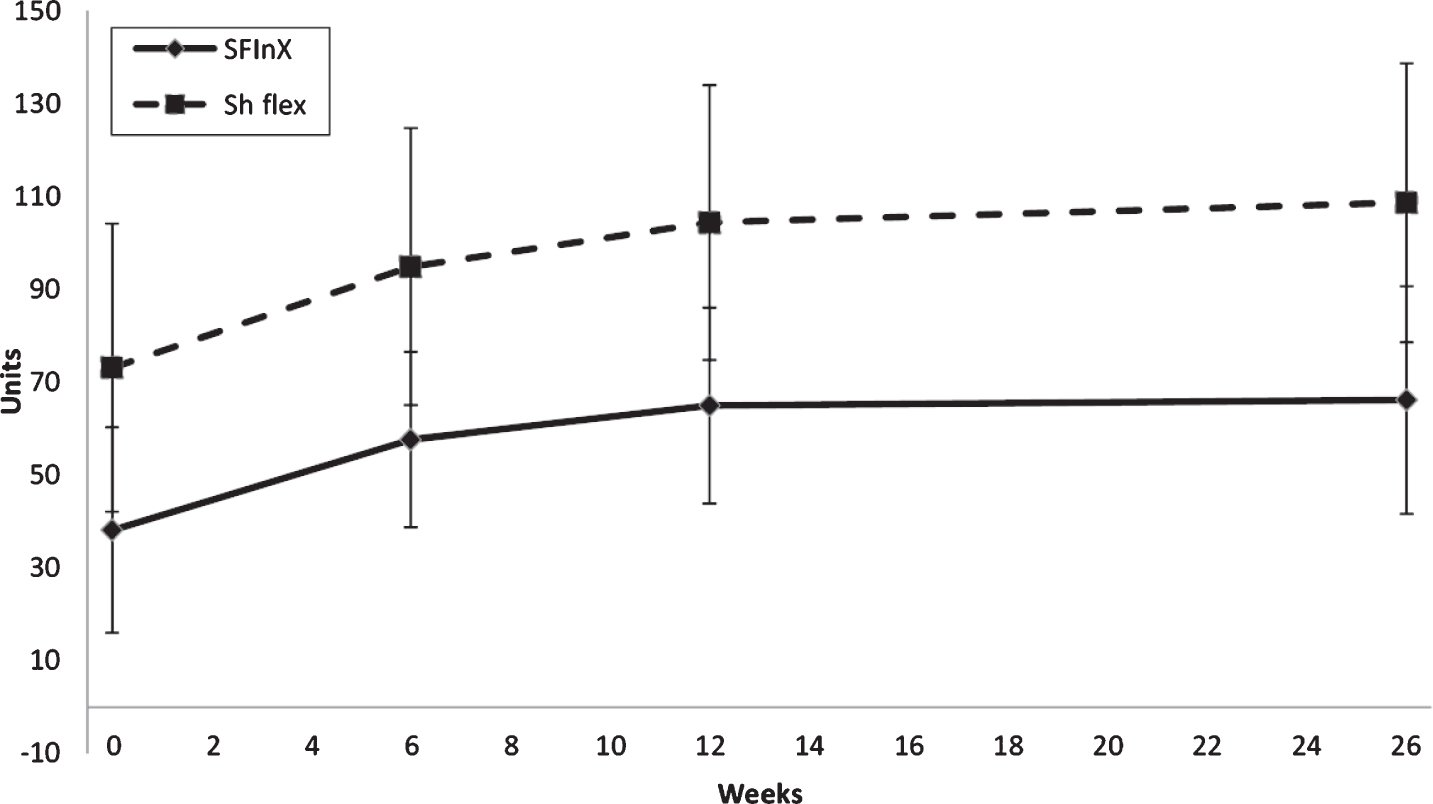
Recovery trajectory of activity (SFInX units 1 to 100) and range of shoulder flexion (degrees) from baseline (week 0) to week 26 after commencement of physiotherapy in community rehabilitation for patients with proximal humeral fracture.
Three percent of participants (1 of 38) achieved the threshold score of 73 units on the SFInX at week 0, 21% (8 of 38) at week 6, 37% (13 of 35) at week 12 and 44% (15 of 34) at week 26 (Table 4, Fig. 3). Forty-seven percent of participants (18 of 38) demonstrated a moderate clinical improvement in their SFInX score (+Δ17 units) by week 6, increasing to 69% (24 of 35) by week 12 (Table 5, Fig. 2).
Participants meeting shoulder activity threshold of SFinX ≥73 units. Mean (SD) of groups at each time, and mean difference (95% CI) between groups
Participants meeting shoulder activity threshold of SFinX ≥73 units. Mean (SD) of groups at each time, and mean difference (95% CI) between groups
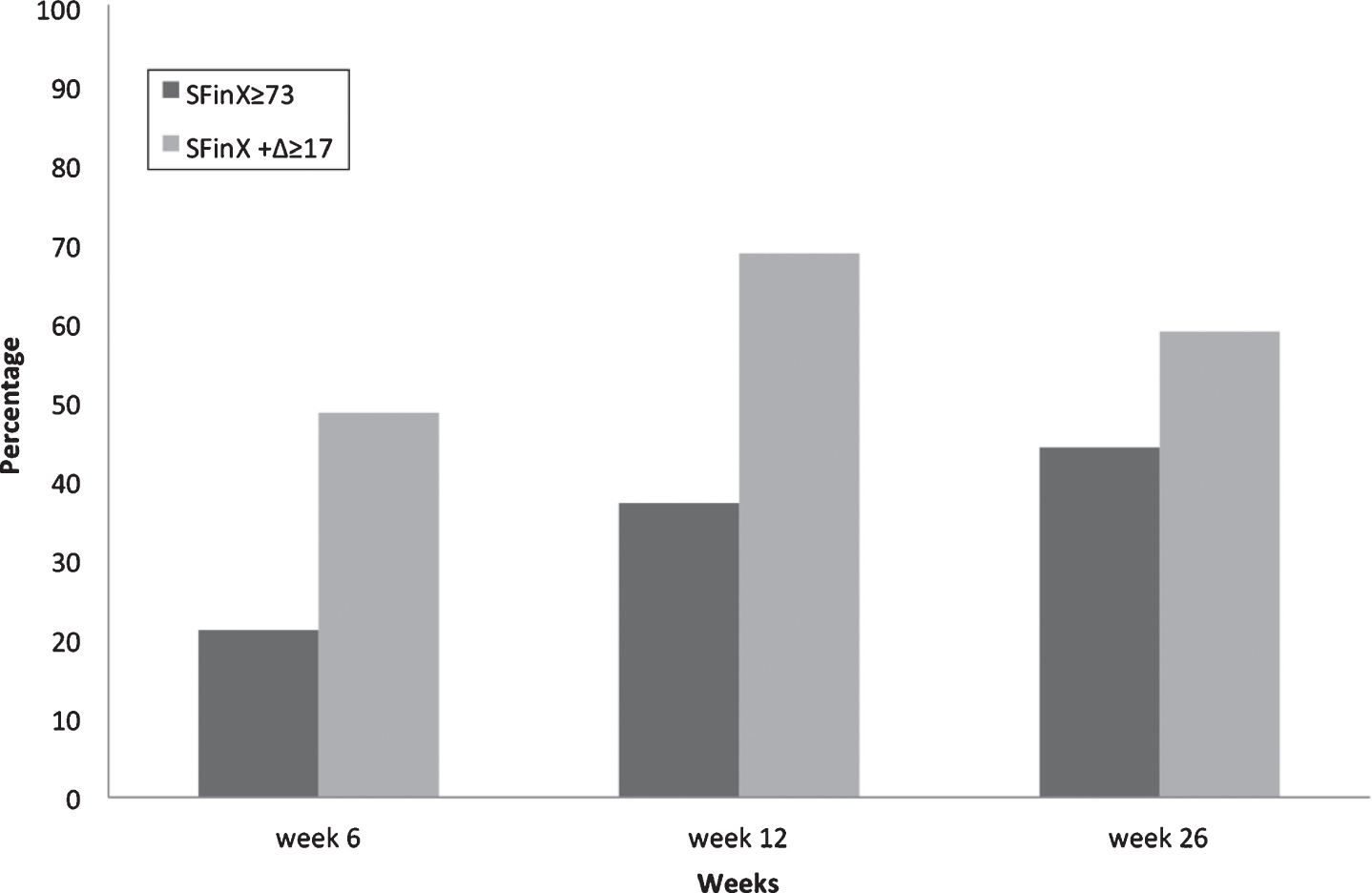
Proportion (percentage) of patients with proximal humeral fracture meeting activity thresholds of a score of at 73 units or an improvement of at least 17 units on the SFInX weeks 6, 12 and 26 after commencement of physiotherapy in community rehabilitation.
Participants who achieved the SFInX threshold score of 73 units had a lower DASH score, a higher health-related quality of life index, and increased range of shoulder flexion, abduction and external rotation at all three times compared to those participants who did not achieve a SFInX score of 73 (Table 4). Participants who improved by at least 17 units on the SFInX at weeks 6, 12 and 26 had an increased range of shoulder flexion compared to those who did not. There was no association between the number of sessions with a physiotherapist or duration of rehabilitation and achievement of activity thresholds (Tables 4 and 5).
Participants increasing shoulder activity by at least a moderate amount of SFinX ≥17 units from baseline. Mean (SD) of groups at each time, and mean difference (95% CI) between groups
Participants increasing shoulder activity by at least a moderate amount of SFinX ≥17 units from baseline. Mean (SD) of groups at each time, and mean difference (95% CI) between groups
Range of shoulder flexion was the variable that best differentiated those achieving activity thresholds as it was the only variable to demonstrate significant differences for both activity thresholds at all three times. Receiver operating curve analysis of range of shoulder flexion demonstrated excellent diagnostic accuracy for achieving SFInX ≥73 at week 6 (AUC 0.93, 95% CI 0.85 to 1.0) and fair diagnostic accuracy for achieving+ΔSFInX ≥17 at week 6 (AUC 0.74, 95% CI 0.58 to 0.90). Optimal shoulder flexion cut-offs to achieve activity thresholds were achieved when shoulder flexion exceeded 112°.
Of the eight eligible treating physiotherapists, five participated in the focus group. The treating physiotherapists (4 women, 1 man) had worked in the community rehabilitation program at the health service for between 2.0 and 5.5 years and could be described as being early to mid-career physiotherapists. The primary theme to emerge was that, although they viewed the SFInX as an objective and standardised measure of shoulder activity/function, they believed it was not useful in informing their decision making:
I think ultimately for me in terms of treatment direction, you kind of go from your conversation about goal setting on where you’re going to direct treatment ultimately. But the SFInX was a good, I suppose, objective measure at that point of functional task potentially but I don’t know how much influence it had on treatment per se. (Physiotherapist #3)
Physiotherapists were consistent in using attainment of specific patient goals to inform discharge planning rather than the SFInX:
From your impairment-based assessment as well as your goals I think you can tell whether or not someone’s plateauing and planning from there, so it [the SFInX) didn’t really aid us in that way. (Physiotherapist #5)
The second theme to emerge was that physiotherapists discussed the practical challenges of using the SFInX in the home environment, where equipment, such as standard weights and a soccer ball, was perceived to be cumbersome to take with them for home visits:
I found that most of my clients tended to be home based, so it did require you to take out quite a lot of equipment. It was challenging at times to find appropriate height shelves and things to make it really standardised. (Physiotherapist #1)
Discussion
Patients referred to physiotherapists in a community rehabilitation program after proximal humeral fracture demonstrated minimal clinically important improvements in shoulder activity as measured by the SFInX within the first 6 weeks of therapy. Fewer than half of participants achieved designated activity thresholds on the SFInX by week 6, but more than half had made moderate clinical improvements in shoulder activity by week 12. A range of shoulder flexion of at least 112° was the variable that best discriminated between those who were able and unable to achieve activity thresholds. Physiotherapists reported they did not use the SFInX to inform their decisions about patient management and discharge planning.
Approximately 8 sessions of physiotherapy comprising goal-directed exercise training and advice over 8 weeks were sufficient to lead to clinically important increases in shoulder activity, improved health-related quality of life and shoulder range of movement with benefits maintained at 6 months. The median time for commencement of active physiotherapy after fracture was 12 weeks; in contrast to recommendations that proximal humeral fractures benefit from early mobilisation [5, 33]. The high levels of disability at week 0 (mean DASH score 50.0 units), suggests participants may have received little physiotherapy prior to referral to community rehabilitation. These results appear to suggest patients benefitted from referral to a physiotherapist although, without a non-treatment control group, other explanations such as natural recovery have to be considered. The few controlled trials of exercise interventions after proximal humeral fracture have reported uncertainty about the outcomes, perhaps due to small sample sizes [34].
Despite clinically significant improvements, the findings of impairments and activity limitation at week 26 (approximately 9 months after fracture) are consistent with reports of ongoing disability after proximal humeral fracture in older persons [6, 36]. Many of the participants in our study were unable to elevate their shoulder above 90° at the final assessment approximately 9 months after fracture, DASH scores were indicative of a moderate level of functional disability and health-related quality of life remained significantly less than their age-matched peers without proximal humeral fracture [6]. Mean health-related quality of life EQ-5D index scores (index score 0.72) and VAS pain levels (2.6 units) in our study at 6 months were the same as those reported at a mean of 4 to 5 years after fracture [35]. Others also report similar mean DASH scores and EQ-5D index scores after 2 years [6]. This could suggest participants in our study may have achieved their optimum outcome by 6 months, approaching a ceiling level of recovery, supporting the decision of physiotherapists to discharge most participants by 12 weeks.
The SFInX provided quantitative data supporting its use as a useful outcome measure to monitor progress and inform decision making after proximal humeral fracture. The measure was responsive, demonstrating clinically important improvements in shoulder activity from week 0 to week 6. The ability to meet activity thresholds may be a useful target for informing discharge planning, especially the moderate clinically important increase of 17 units on the SFInX. The target of achieving a threshold SFInX score of 73 may be too difficult for a proportion of this older population with multiple morbidities. A threshold of less than 73 units on the SFInX may be a more suitable target for this population, who on average were older than the cohort with proximal humeral fracture on which psychometric testing was completed [12].
Despite the ability of the SFInX to show changes in shoulder activity, physiotherapists in the study did not use it to inform their decision-making. Physiotherapists reported they focused their management and discharge planning on person-centered goal setting, a collaborative process towards finding goals that are meaningful to the patient [37, 38]. The physiotherapists, however, did not seem to consider the hierarchy of tasks in the SFInX could be used as a basis for exploring goals that might be meaningful to their patient. Furthermore, the tasks in the SFInX were included after careful selection and analysis of meaningful activities based on focus group input from people with a proximal humeral fracture and their treating clinicians [10]. Indeed, the most common activities chosen for person-centred goal setting after proximal humeral fracture are included in the SFInX: combing hair, reaching for objects above shoulder height and putting on clothes [39]. One explanation for these results is that the physiotherapists were obliged to use the SFInX for the study; they did not choose to use it and perhaps saw it as an addition to their normal practice. Another explanation is that physiotherapistsmay be reluctant to change practice, including assessment, even when that change of practice is based on evidence. This explanation is consistent with reports that 43% of physiotherapists may not follow evidence-based guidelines when treating common musculoskeletal conditions [40]. However, the physiotherapists raised important concerns about incorporating the SFInX into their practice, such as the practical difficulty of taking equipment with them on home visits; and the priority they placed on patient-centered practice, basing assessments on what was considered to be most meaningful to their patient. While acknowledging that the SFInX could be used as an objective outcome measure, the concerns of the physiotherapists question the extent to which the SFInX might be incorporated into usual care of patients recovering from proximal humeral fracture.
Range of shoulder flexion emerged as the measure that was best able to discriminate ability to achieve shoulder activity thresholds derived from the SFInX. The ability to elevate the shoulder to at least 112° was associated with being able to complete most shoulder tasks required for activities of daily living and to achieve moderate clinically important improvements in doing those tasks. Although association between impairment and activity limitation cannot be assumed, similar associations have been demonstrated for other fractures of the upper limb [41]. Therefore, a quick and easy measure of impairment was able to indicate activity limitation. Based on these findings assessment of shoulder flexion is indicated for physiotherapists to monitor progress after proximal humeral fracture. This association may be explained by the importance of having sufficient range of movement to place the hand for upper limb function. Despite its use, assessment of shoulder flexion alone does not provide information about specific tasks that the patient may find difficult to complete; assessment with the SFInX can provide this information.
A limitation of this study was the relatively small sample size. However, 145 full assessments were completed over 6 months providing comprehensive data on rehabilitation and recovery after proximal humeral fracture. The small sample size did not allow for exploration of other factors such as operative versus conservative management. However, anecdotally, physiotherapy management at the stage of referral to a physiotherapist in this study (a median of 12 weeks after fracture) would be expected to be similar regardless of orthopaedic management. The specific content of the physiotherapy sessions was not recorded as part of the study which may have provided more detailed insights in used type of interventions and dose. The observational design does not allow conclusions about the effect of interventions, but can provide data for hypothesis generation that could be tested in future randomised controlled trials. The study was completed in a publicly funded community rehabilitation program which may not be generalizable to other health care settings. However, the age and gender ratio suggests our sample was typical of those reported in other studies [6, 34]. Patient focus groups informed item generation in the development of the SFInX [10], but qualitative analysis could have been strengthened by exploring the perceptions of patients who had to complete the SFInX tasks in the current study.
In conclusion, older people after proximal humeral fracture make clinically important improvements in shoulder activity after receiving physiotherapy as part of a community rehabilitation program. The SFInX is a tool with excellent psychometric properties that along with range of shoulder flexion may be a useful option to inform physiotherapist decision-making during rehabilitation.
Conflict of interest
The authors have no financial conflict of interest to declare. Authors van de Water, Taylor and Shields developed the measurement scale evaluated in this study.