
Abstract
BACKGROUND:
A coma is a prolonged unconscious state in which there is no response to various stimuli. In response, sensory stimulation was designed to stimulate brain plasticity and to promote brain regeneration. The effects of sensory stimulation intervention on comatose patients following traumatic brain injury (TBI) remain unclear.
OBJECTIVES:
This study aimed to examine the effects of sensory stimulation on the level of consciousness (LOC) after TBI and to identify the effective treatment dosage.
METHODS:
We searched PubMed, REHABDATA, EMBASE, CINAHL, MEDLINE, PEDro, SCOPUS, and Web of Science from inception to February 2020. Experimental studies investigating the influence of sensory stimulation on the LOC in the comatose patients (Glasgow coma scale < 8) following TBI were selected. The Physiotherapy Evidence Database scale (PEDro) was used to evaluate the methodological quality.
RESULTS:
Eleven studies met the inclusion criteria. Six were randomized controlled trials (RCTs), clinical controlled trials (CCTs) (n = 2), and pilot studies (n = 3). A total of 356 comatose patients (<8 on GCS) post-TBI were included in this study with sample sizes ranging from 5–90 patients. The sample sizes for the selected studies ranged from 5 to 90 patients. The scores on the PEDro scale ranged from three to eight, with a median score of seven. The multimodal sensory stimulation showed beneficial effects on the LOC in the comatose patients following TBI. The evidence for the effects of unimodal stimulation was limited, while the optimal treatment dosage remains unclear.
CONCLUSIONS:
The multimodal sensory stimulation intervention improves the LOC in patients with coma after TBI compared with unimodal stimulation. Further high-quality studies are needed to verify these findings.
Introduction
Traumatic brain injury (TBI) is a leading cause of disability and hospitalisation in intensive care units (ICU) worldwide [1]. About 17% of people who survive TBI have a period of complete unconsciousness or coma with no awareness of themselves or their surroundings [2]. A coma is a prolonged unconsciousness state in which an individual cannot be awakened, fails to respond regularly to painful stimuli, light, or sound, lacks a normal wake-sleep cycle, and does not initiate voluntary actions [3]. Altered loss of conciseness is associated with adverse effects on the normal functioning, long length of altered consciousness, functional dysfunction severity, slow recovery, and poor prognosis [3].
As people recover from TBI, they normally pass through several phases of recovery in which recovery can stop at any phase [4]. The transition between the phases is usually very gradual and highly distinctive depending on many factors, such as type and location of the injury, past medical history, age, and response to the treatment [4]. The long-term impacts of the TBI can influence the ability to participate in activities of daily living (ADLs) [5]. Acoma occurs due to disturbance in the function either of the brainstem reticular activating system (RAS) above the mid pons or of both cerebral hemispheres [6]. They may have a simple reflex in response to touch or pain, but they show no meaningful response to external stimuli [7].
The coma can last from hours to days, depending on the severity of brain damage [7]. Some people remain in a comatose state for months or even years [7]. A person in a coma may experience some improvement and transition to a vegetative state in which lower brain functions (e.g., sleep cycles, heart rate regulation) and some upper brain functions (e.g., eye-opening, sound production) are present [7, 8]. One of the most serious problems among the unconscious individuals is sensory deprivation because their ability to react to internal and external stimuli is altered [8]. It can cause different mental and perceptual problems and life-threatening conditions for patients hospitalised in the intensive care unit (ICU) [9]. The practical implication of the sensory deprivation is that controlled stimulation may meet the higher threshold of the reticular neurons and increase the cortical activity. The undamaged axons may send out collateral connections called the collateral sprouting that assist in reorganizing the brain activity [10].
The sensory stimulation can stimulate the process of post-TBI plasticity, promote brain regeneration, improve neurologic function [11], shorten the length of the ICU stay, and alleviate anxiety [12]. The multimodal stimulation (e.g., tactile and gustatory, auditory, and tactile) has been investigated concerning the wake cycle and purposeful movements [13]. A growing knowledge implies that the recovery processes are activated immediately after TBI [11]. One such recovery process is plasticity [11]. Enhancement of plasticity occurs through both endogenous factors such as the release of nerve growth factor, and the exogenous factors such as environmental or sensory stimulation [14].
Recently, one systematic review by Padilla and Domina (2016) examined the effectiveness of sensory stimulation on the arousal and alertness of individuals in a coma or vegetative state [14]. It was limited by the number of studies that were published between 2008 to 2013. Their results were not definitive because of the selected studies in their review had a small sample size and short intervention period [14]. Recently, there is an increase in the number of studies that investigate the influence of sensory stimulation in comatose patients following TBI. This review aimed to investigate the effect of sensory stimulation approaches on the LOC in comatose individuals after TB and, if possible, to identify the effective treatment dosage by studying and analyzing the existing evidence.
Methods
Search strategy and study selection
An electronic search was conducted in PubMed, REHABDATA, EMBASE, CINAHL, MEDLINE, PEDro, SCOPUS, and Web of Science from inception to February 2020. The keywords were (sensory stimulation OR stimulation OR acoustic stimulation OR physical stimulation) AND (brain injury OR trauma OR traumatic brain injury OR traumatic) AND (coma OR comatose) AND (level of consciousness OR consciousness OR Glasgow coma scale OR arousal) (Fig. 1).
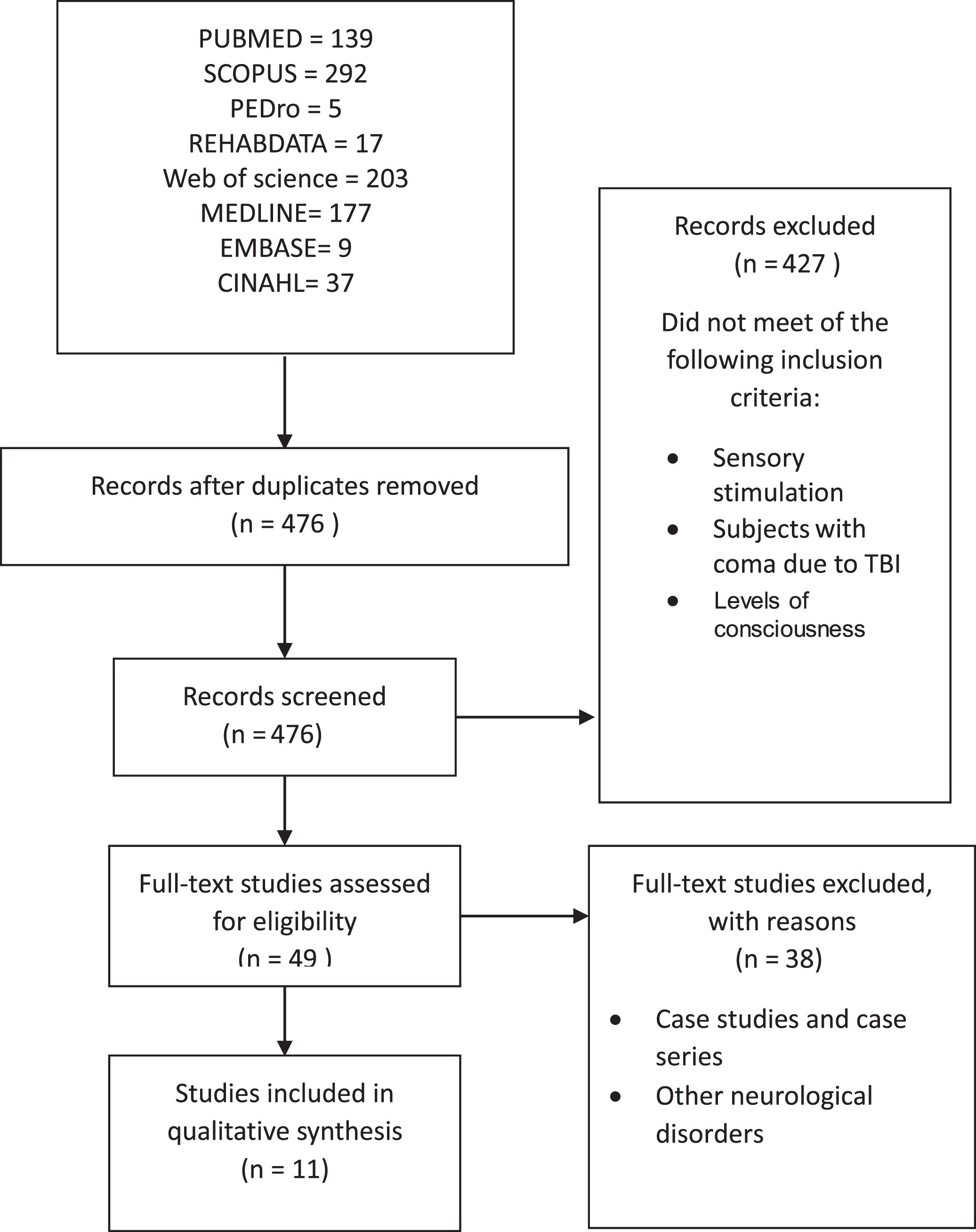
Summary of literature review process.
The present review followed the PRISMA guidelines. And the PICOS approach (P: participants; I: intervention; C: comparison; O: Outcomes; S: study design) [15]. Studies were included if they (a) assessed comatose patients (<8 on Glasgow coma scale [GCS]) following TBI, (b) used sensory stimulation intervention, (c) classified as an experimental study published in English, (d) assessed level of consciousness, and (e) compared with active/passive control group or no control. Articles were excluded if they (a) assessed patients in coma or vegetative caused by non-traumatic disorders, (b) lack of outcome data, (c) descriptive studies, and (d) animal models.
Methodological quality
Two authors assessed the methodological quality for the included studies using the Physiotherapy Evidence Database scale (PEDro) scale. The PEDro scale provides an overview of a study of the internal and external validity. Furthermore, it assesses the capability of statistical analysis [16]. Four grades of the PEDro scale have been validated, while other grades have face validity [17]. Lastly, inter-rater reliability has been confirmed [16, 18]. The non-randomization, non-blinding of evaluators, no intention to examination, and no measurement of compliance were central threats to the biasing [19]. The methodological quality scores for the selected studies are presented in Table 1.
Methodological quality scores
Methodological quality scores
Y: low risk of bias; N: high risk of bias; ?: not clear.
The data were extracted by two authors. The data were extracted: (1) study design and participants, (2) treatment protocol, (3) experimental intervention, and (4) control group intervention (Table 2).
Study characteristics
Study characteristics
Table 3 presents the outcome measures details (GCS). The effect sizes were established by dividing the difference between the means of both groups by the pooled SD [20]. The effect size (ES) was determined using Cohen’s d >0.8 was large, 0.5 moderate, and <0.2 small [21].
Outcome measures
GCS: Glassgow Coma Scale;+: Significant improvement in the experimental group.++: improvement in both groups/conditions without significant difference=: No significant difference between groups.
Strong evidence indicates consistent results from at least two RCTs. Moderate evidence is made based on one RCT, two or more studies with lower levels of evidence. Limited evidence is based on few studies, flaws in available studies, or some inconsistency in the findings across individual studies [21]. After reviewing the results of the included studies, the meta-analysis was not appropriate because of the significant heterogeneity of the treatment protocols.
Study selection
A systematic search of databases produced a total of 879 articles. After eliminating the duplicates, 476 articles were reviewed. Out of those, 427 articles were excluded based on their abstracts Forty-nine full text studies were reviewedThirty-eight studies were removed for the following reasons: case studies/case series and include other neurological disorders. A total of 11 studies were included in the current review (Fig. 1).
Methodological quality
Six of the selected studies were RCTs [22–27], CCTs (n = 2) [11, 28], and pilot studies (n = 3) [29–31]. Five studies [11, 28–31] did not perform to random allocation, whereas nine studies [11, 26–31] failed to concealed allocation. Five studies failed to blind the assessors [11, 28–31]. Three studies failed to initiation to treat analysis [11, 30]. Finally, four studies failed to report between-group analysis [11, 29–31]. Six studies were of high methodological quality (>6/10) [22–27]. Whereas five were of low methodological quality (<6/10) [11, 28–31]. (Table 1).
Outcome measures
The selected studies used the Glasgow Coma Scale (GCS) to assess the level of consciousness (LOC). The GCS is a reliable, objective way of recording the individuals’ consciousness level, derived from the eye-opening, verbal response, and motor response [32]. The lowest possible GCS (the sum) is 3 for the deep coma or death, while the highest is 15 for a fully awake person. The inter-rater reliability of the GCS has been reported to be in an acceptable data [33].
Description of included studies
Participants
A total of 356 comatose patients (<8 on GCS) post-TBI were included in this analysis. Sample sizes ranged considerably from 5 to 90 patients. The majority of patients in the included studies were male (82%), with the mean age (36.45 years old). Regarding the length of coma before the beginning of the intervention, seven studies included patient with <1-month coma status history [11, 27–29]. The remaining studies did not provide details about the length of coma status [26, 31].
Intervention
Unimodal stimulation: Three studies used unimodal stimulation (i.e., auditory stimulation) to stimulate the LOC in comatose patients post-TBI [11, 31] compared with usual care [11] and natural voices of environment [23] control groups.
Multimodal stimulation: Eight studies [23–30] used multimodal stimulation to stimulate the LOC in the comatose patients post-TBI compared with no intervention [22, 28], conventional physiotherapy [24], and usual care [25–27] control groups.
Effects of sensory stimulation on the level of consciousness in comatose patients after TBI
Unimodal stimulation
No significant change in the GCS scale scores was reported in the comatose patients following auditory stimulation intervention compared with usual care [11] and the natural voices of the environment [23] control groups. The study by Park and Davis (2016) reported an increase in the GCS scores after the direct and non-direct auditory stimulation conditions with no significant difference [31].
Multimodal stimulation
Eight studies [22, 24–30] reported a significant increase in the GCS scores following multimodal auditory stimulation intervention compared with no intervention [22, 28], conventional physiotherapy [24], and usual care [25–27] control groups. Two studies did not include control groups [29, 30]. The results were presented in Table 3.
Adverse effects or side effects
No adverse effects, side effects, or serious complications were reported after the sensory stimulation intervention in the included studies.
Discussion
The present systematic review aimed to examine the influences of sensory stimulation intervention on the LOC in the comatose patients following TBI and to define the optimal treatment dosage. The main finding showed strong evidence for the positive effects of multimodal sensory stimulation on the level of consciousness in comatose individuals post-TBI. We were unable to establish any benefits attributable to unimodal stimulation. Thus, the effects of unimodal stimulation are still limited. Padilla and Domina (2016) showed strong evidence of the impacts of multimodal stimulation on arousal and alertness of individuals in a coma or vegetative state after TBI [14]. As well, Karma and Rawat (2006) found that sensory stimulation is an effective intervention in improving the LOC in the comatose patients following non-traumatic brain injury [34]. Any effective stimulation affects the brain can activate the reticular activating system [34]. This results in increased sympathetic activity in different parts of the body, increased norepinephrine release in nerve terminals, and greater consciousness and arousal [35]. Moreover, it stimulates the nervous system development [36]. The human brain responds to kindly stimulation and behaviors by releasing hormones from the frontal cortex. These hormones increase the overall activity of the brain and improve the LOC [36]. Our results are consistent with the findings of Mitchell et al. (1990) [28], Kater (1989) [37], and Oh and Seo (2003) [30]. According to Kater (1989), the recovery can be explained by alteration such as axonal sprouting, rerouting, and anomalous connections to various regions of the brain and by the compensation mechanisms of the brain [37]. Although the GCS is a reliable outcome measure for recording individuals’ consciousness levels [32]; however, it can lead to misdiagnosing vegetative and minimal consciousness states. This misdiagnosis can lead to significant clinical, therapeutic, and ethical consequences [38].
The efficacy of multimodal sensory stimulation can be explained based on the concept of Perrin et al. (2006). He reported that although the resting metabolism of the comatose individuals is reduced, the auditory cortices (Brodman’s areas numbers 41 and 42) are still responding to the tone [39]. Similarly, Sullivan et al. (1998) showed that the olfactory stimulation raised blood flow to the frontal lobes and the orbitofrontal cortex. Thus, activating the brain regions vital for planning and judgment [40]. Keller et al. (2007) also confirmed that the various kinds of stimulation increase the autonomic nervous system (ANS) activity, which confirms the fact that they have an impact on the Reticular activating system [41].
The selected studies failed to blind the participants and therapists, leading to potential bias. While it is difficult to blind the participants and therapists to the intervention, it is possible to blind the assessor. Therefore, this is important to reduce the bias correlated with measurement based on outcomes [39]. In a total, six studies were of high methodological quality (>6/10) [22–27]. Whereas five were of low methodological quality (<6/10) [11, 28–31].
Three studies investigated the effects of unimodal stimulation (i.e., auditory) on the LOC in the comatose patients post-TBI [11, 31]. Only one study by Park & Davis (2016) demonstrated an improvement in the LOC after both direct and non-direct auditory simulation conditions. This study was of low methodological quality (3/10) and had a small sample size (n = 9) [31]. So the meaningful effects cannot be established. As well, Gorji et al. (2014) and Davis & Gimenez (2003) explained that the lack of support for using the sensory stimulation is related to the small sample size [11, 23].
Eight studies demonstrated improvements in the LOC in the comatose patients post-TBI after multimodal stimulation intervention [22, 24–30]. Three studies were of low quality on the PEDro scale (High risk of bias) (<6/10) and had a small sample size (<25) [28–30]. The significant differences are not allowed to calculate with a small sample size [42]. So it is not possible to establish the clinical importance of the reported effects. The remaining five studies were of high methodological quality on the PEDro scale (>6/10) and had a large sample size [22, 24–27]. The effect sizes were small to large (0.00–2.53). So the meaningful effects can be established.
Three studies administrated multimodal sensory intervention within several days post-coma [22, 25], while two studies did not provide information about the time of beginning the intervention [26, 27]. As the most neurological recovery occurs early after brain injury [42]; thus, it seems that earlier intervention could provide more efficient improvement in the LOC in the comatose patients after TBI. In agreement with Padilla and Domina (2016), the multimodal sensory stimulation should be administrated early after the coma [14]. The recovery processes in the TBI are activated immediately following the injury [43, 44]. The plasticity recovery permits the brain to modify its organization and function [45]. Improvement of plasticity occurs through exogenous factors, such as environmental or sensory stimulation [14].
Because of the heterogeneity treatment protocols, identifying the optimal treatment dosages remain unclear. Moreover, to date, the long-term effects of the sensory stimulation on the LOC remain unclear. The effects of multimodal sensory stimulation on the LOC in comatose patients with non-traumatic injuries remain ambiguous. Moreover, many studies had small sample sizes and were of poor methodological quality. High-quality studies with large sample sizes and long-term follow-ups are warranted to determine the most effective treatment parameters. Established studies investigated the effects of sensory stimulation on the LOC on the non-traumatic comatose patients strongly needed.
There are several limitations to this systematic review. The search process was limited by studies published in the English language. This leading to bias since the research papers with significant findings are also more likely to be published in the English language [46]. Thus, reviewing only studies published in English could lead to an overestimation of treatment impacts [47]. The meta-analysis was not performed because of the heterogeneity of the treatment interventions between the selected studies. However, the effect sizes were calculated. Lastly, the effect size for some of the selected studies was not calculated because data were presented as a median instead of mean and standard deviation. This limited our ability to perform a meta-analysis.
Conclusion
The multimodal sensory stimulation intervention may improve the LOC in the comatose patients following TBI. The unimodal sensory stimulation appeared ineffective relative to multimodal stimulation. The optimal treatment dosage remains unclear. Further high quality and adequately powered randomized controlled trials are needed to verify our findings and hypothesis.