
Abstract
OBJECTIVES:
Injury in Irish dancing (ID) is pervasive and comparable to that in other elite dance genres. There is an absence of formalized education or training for ID teachers to understand and address this issue. This study investigated the injury prevention knowledge and beliefs of registered ID teachers internationally.
METHODS:
An online survey based on an existing questionnaire by the Fédération Internationale de Football Association (FIFA) was adapted to reflect relevant research in ID and other dance genres. It was piloted with seven ID teachers internationally. Participants, who were registered ID teachers were recruited through official ID governing bodies and the networks of the Principal Investigator.
RESULTS:
Two hundred and thirty participants from eleven regions internationally completed the survey. A robust knowledge of the anatomical areas most often injured was displayed, with conflicting opinions on the incidence, location and causes of injuries in males and females. There was a clear appreciation of the vast array of risk factors potentially associated with injury, with warm-up, load management, physical strength, conditioning and flexibility all highly rated. There was lesser insight into important factors such as sleep, nutrition, and general and psychological health. Most teachers rated their injury prevention knowledge and practices as moderate/good but available educational resources as poor/fair.
CONCLUSIONS:
There is a need for education and training in numerous areas of injury prevention by multidisciplinary healthcare practitioners and other professionals, in partnership with the ID community, to ensure a clearer understanding of the biopsychosocial nature of injury prevention and performance optimisation.
Introduction
Irish dancing (ID) is a highly competitive and athletic dance genre, and arguably one of the most recognised traditional dance forms internationally [1]. “An Coimiusiun Le Rinci Gaelacha” (the ID Commission), which is just one of several governing bodies for ID, lists nearly 2,500 active teachers and adjudicators in over 30 countries across five continents [1]. Unlike other forms of dance such as ballet and contemporary dance, ID is distinct in its extensive international competitive calendar, which culminates in the annual World Irish Dancing Championships. This event welcomes approximately 5,000 elite dancers who must qualify for the event at regional and national events, and then compete against dancers in their own age category. Success at the highest competitive level is a potential gateway to a coveted professional career in renowned productions such as “Riverdance” or “Lord of the Dance”. This has led to an exponential increase in the complexity of choreography and physical and psychological demands of ID in recent years.
It is therefore unsurprising that the incidence of injury in elite competitive Irish dancers is substantial [2–4], and comparable to that experienced by elite dancers in other genres [5]. Elite in this context refers to professional Irish dancers, and/or those who participate at the highest competitive level, known colloquially as “open” dancers. In a prospective study of 37 elite adolescent Irish dancers followed up weekly for one year, at least one injury was incurred by 86.5% of participants, with ten participants (27.1%) reporting between five and eleven injuries during the study period [6]. Time-loss as well as non-time-loss (dancing when injured) injuries were explored in this study, to establish anecdotal reports of dancers continuing to train and compete when in pain and/or injured. These studies confirmed that Irish dancers do continue to practice and perform when injured, as indicated by differences in the overall injury incidence (time-loss plus non-time-loss) and time-loss only injury incidence of 9.3 injuries and 4.5 per 1000 hours/dance respectively.
Due to heterogeneity in the definition of injury used within dance medicine, it can often be difficult to compare findings between genres. However, a study exploring injury in a mixed cohort of collegiate contemporary and ID students found similar levels of injury in both groups, with at least one episode of injury reported in the previous year by 83.3% and 92.6% of contemporary and Irish dancers respectively [7]. When these groups were followed prospectively each week for one year [13], an overall incidence of 10.6 injuries per 1000/hours dancing for Irish dancers was recorded, compared to 8.4 injuries per 1000/hours for the contemporary dancers. There is a paucity of evidence in professional ID, but one study of 178 participants has reported that 137(77%) dancers suffered at least one career injury while dancing professionally [8]. Only three dancers (1.7%) reported never dancing in pain, while 60 (34%) dancers often or always danced in pain.
The causes of injury in ID are multifaceted and complex, and include numerous intrinsic and extrinsic risk factors. These include failing to always do a warm-up [2, 9], poorer general health [5, 10], poor sleep [6, 10] and a number of psychological issues including low mood, suboptimal coping and heightened catastrophizing [9, 11].
Additional risk factors identified include a high level of general everyday pain (subjective reports of non-dance related pain experienced by dancers) [10, 12] and severe previous injury [10]. Injury in professional Irish dancers was found to be significantly associated with older age and greater experience [8], with older age, level of competition and increased training load also identified as risk factors in competitive cohorts [3, 4]. Injury in ID overwhelmingly affects the lower limb with the foot/ankle regions accounting for roughly 70% of injuries sustained [3, 13].
To qualify as an ID teacher, one must pass a written exam related to the traditional elements of specific dances and must demonstrate an ability to teach ID and interpret various musical elements. There is no assessment related to any facet of dancer health, wellness or performance. Neither is there any requirement to complete any sort of continuous professional development in this regard. Additionally, there is no centralized information or training regarding the basics of healthy performance and injury management provided by any of the major governing bodies for ID. Anecdotally, teachers feel unprepared to support the prevention and management of injury in their dancers, and rely on trainers and clinicians who are often unfamiliar with the demands and intricacies of the genre.
The aim of this study therefore was to establish the injury knowledge and beliefs of ID teachers to inform future educational strategies to optimise health, injury prevention and performance in these aesthetic athletes.
Materials and methods
Participants
Qualified, actively working ID teachers from any recognised governing organisation for ID were invited to participate. Named representatives of governing bodies internationally were emailed and requested to share study information with their members. Snowball sampling was also employed as the Principal Investigator (PI), who is an ID teacher, shared study details with her networks, and asked colleagues to share further. It is therefore impossible to establish an accurate recruitment rate.
Data collection
An online survey was use to gather data for this study, based on an existing questionnaire used by Fédération Internationale de Football Association (FIFA) to evaluate the injury knowledge and beliefs of coaches in female youth soccer [14]. The questionnaire collects basic demographic data on the age, sex, location, and experience of the teacher as well as specific questions related to the anatomical location, risk factors and causes of injury in ID. Dancing teacher location was categorised according to the ID administrative “region” to which the teacher was affiliated. The FIFA questionnaire was amended to include risk factors commonly associated with dance injury, informed by the literature in this area as discussed previously. It was then piloted with seven ID teachers in diverse geographical locations (Ireland, United Kingdom, Australia, Canada, Mexico) to ensure clarity and appropriateness of the content and language. The questionnaire included an information sheet and contact details for the PI. Informed consent was assumed by completion and submission of the questionnaire. Data were collected during April of 2020.
Statistical analysis
A simple descriptive analysis was used to evaluate participant responses.
Ethics
Ethical approval was granted by the ethics committee of the local University (2020_03_53_EHS (ER)).
Results
Participants
A total of 230 participants completed the questionnaire, of whom 198 (86.1%) were female, and 31 (13.5%) were male. One (0.4%) participant declined to answer this question. The median age of participants was 35–44 years (Fig. 1), and the mean (standard deviation (SD)) years of teaching experience was 15.1 (10.8) years. The United States (n = 113 (49.1%)), Ireland (63 (27.4%)) and Canada (22 (9.6%)) were the regions most represented, with smaller samples from a number of other locations internationally (Fig. 2).
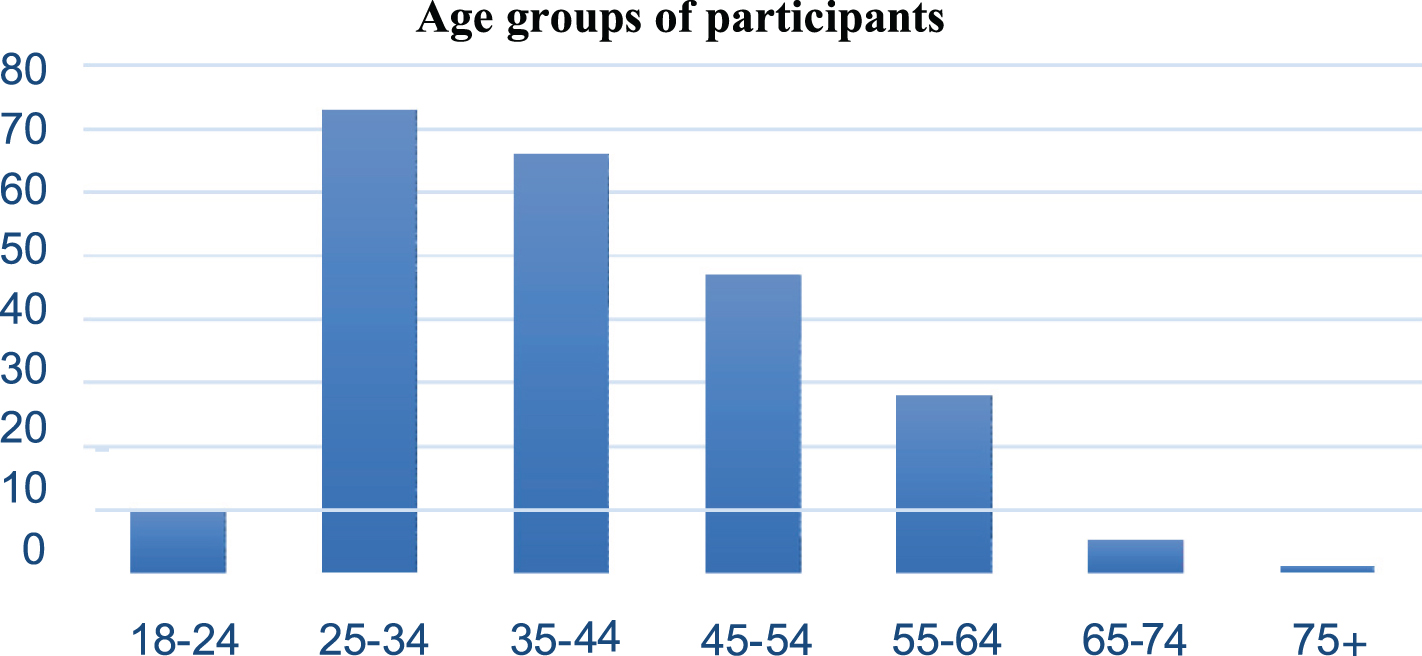
Distribution of participants by age group.
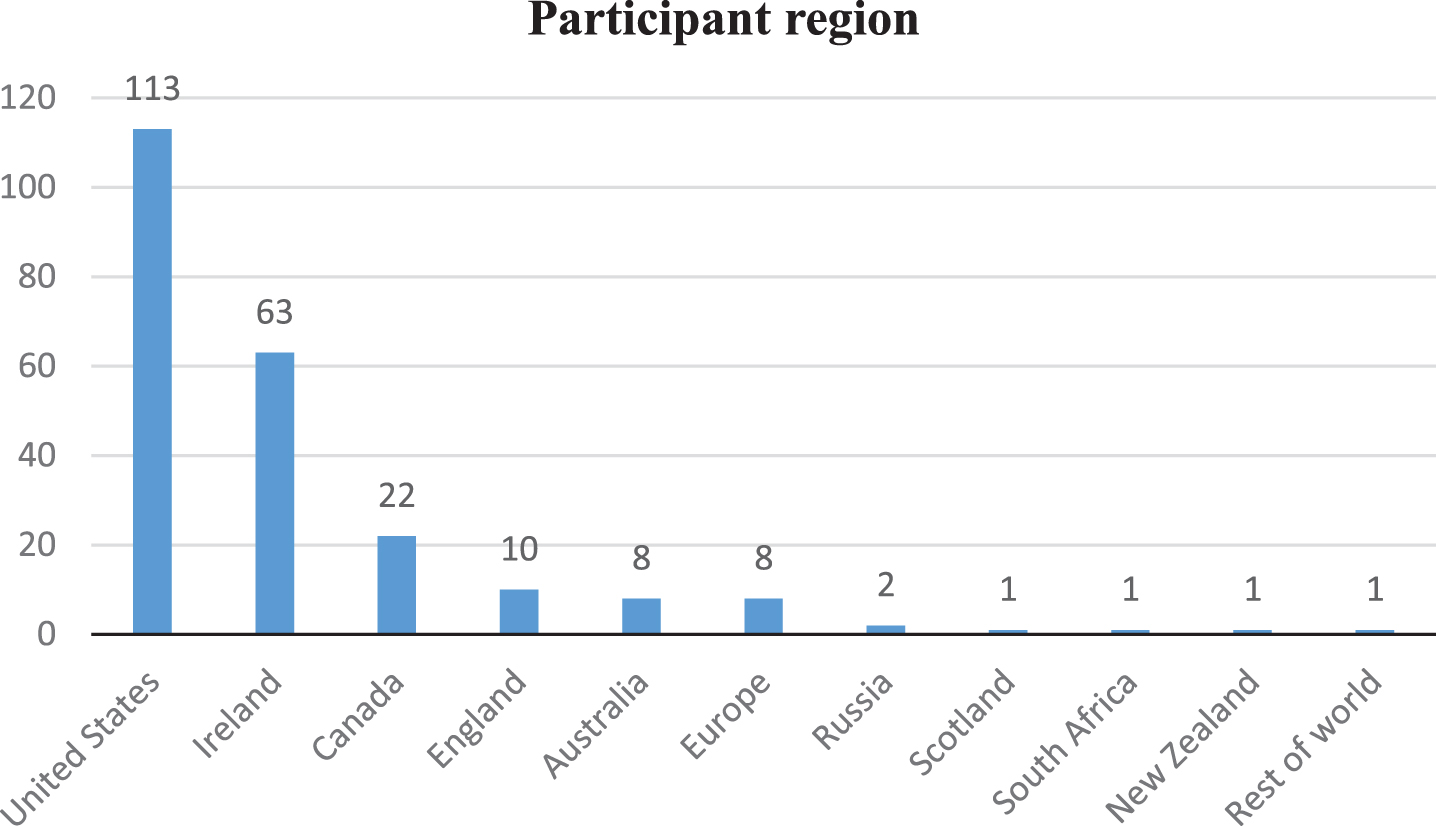
Location of participants by region.
Participants were asked to name the three anatomical regions they believed were most often injured in ID. The foot/ankle was the most commonly named region, identified by 216(93.9%) participants, followed by the knee (132(57.4%)), groin/hip (121(52.6%)) and shin/calf regions (118(51.3%)). Hamstring/quadriceps and lower back/pelvis were mentioned by 82 (35.7%) and 23 (10%) participants respectively. Mid/upper back, shoulder/arm, head/face and wrist/hand collectively were mentioned by just five (2.2%) participants (Fig. 3).
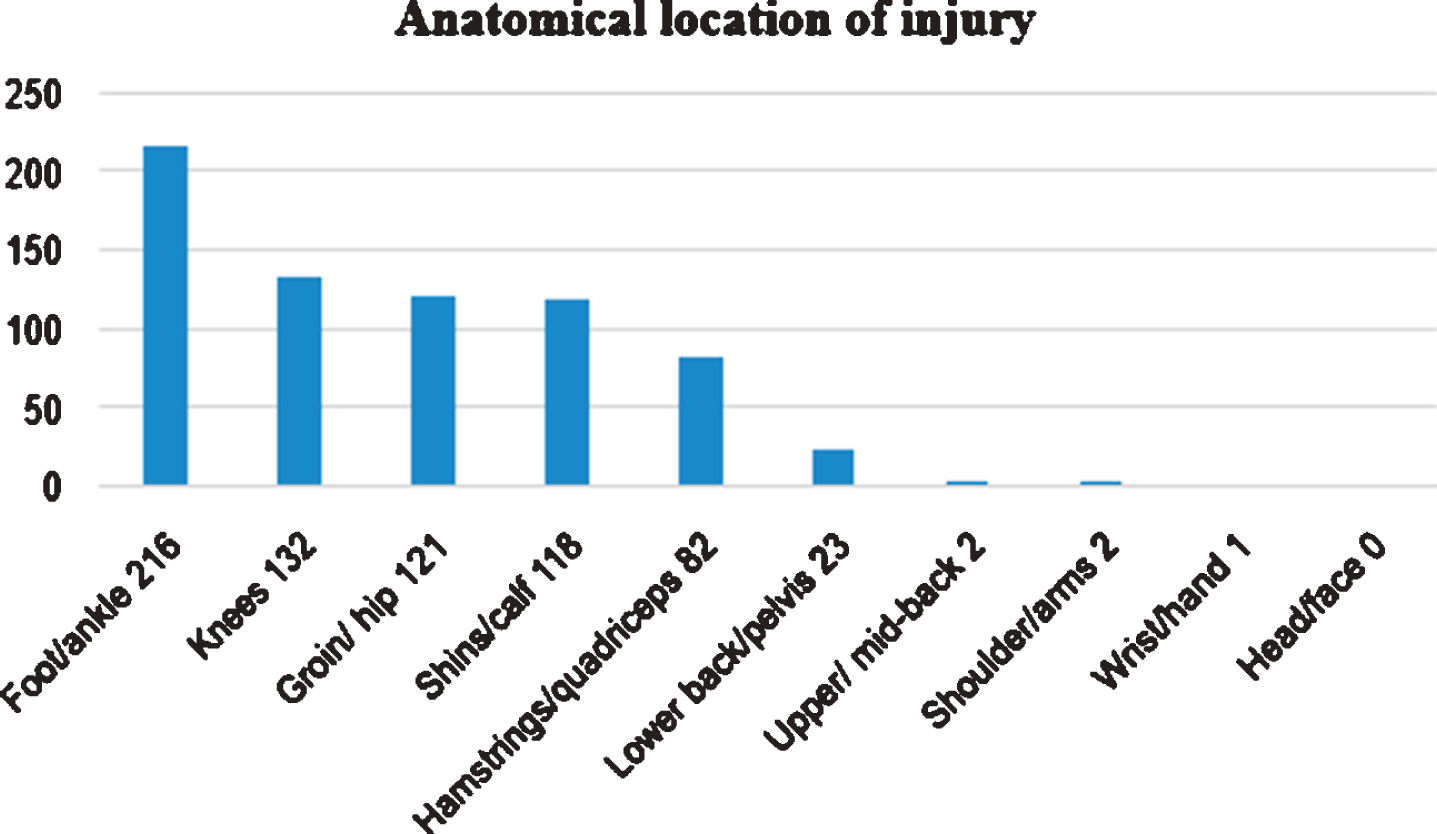
Anatomical location of injury–participant beliefs.
When asked whether they believed if male and female Irish dancers had the same risk of injury, approximately half (116 (50.4%)) of the participants answered yes, while 73 (31.7%) participants answered no. The remaining 40 (17.4%) participants did not know. Forty-five participants who thought that the sexes had the same injury risk provided further comments to support this opinion. These included the homogeneity of dance movements in males and females, using the same muscle groups and undertaking similar training loads. Conversely, of the participants who answered no, 47 provided further comments including differences in biomechanics and dance movements, greater inherent strength in males, and challenges posed by the differing footwear worn by the sexes. Of these 47 participants, 32 clearly identified which sex was at greater risk of injury with 30 (93.8%) participants stating that females were more vulnerable to injury.
Participants were then asked whether they believed males and females sustained injuries to similar body parts. In this case, 146 (63.5%) participants said yes, 41 (17.8%) said no, and 43 (18.7%) were unsure. Reasons similar to those provided in relation to the risk of injury were given. In the main, females were identified as more likely to injure feet, ankles and hips, with males more vulnerable to knee and groin injury. These comments were offered by a smaller group of 36 participants and were not completely consistent (e.g. females occasionally identified as having more knee problems.)
Finally, participants were asked whether males and females sustained injuries due to the same causes. Here, 170 (73.9%) participants said yes, 22 (9.6%) said no, and 38 (16.5%) did not know. Ninety-nine participants, who felt the causes of injury were the same in both sexes provided further comments pointing to similar dance movements, shared intensity in training and common physiological weaknesses. Of the 21 additional comments provided by participants who felt the causes were different between the sexes, themes included the higher level of competition in females, female specific moves such as toe-walks, and greater inherent strength in male bodies.
Participants were then presented with a list of potential risk factors and asked to rank them on a Likert scale according to their association with injury (1 = Not at all, 5 = Very strongly). Factors included a range of intrinsic (modifiable and non-modifiable) and extrinsic risk factors. Factors most strongly identified as associated with injury included previous injury, an inadequate warm-up, dance-training load, and poor stretching and flexibility. Factors identified as least strongly associated with injury, included sex of the dancer, passion for dance, and menstruation in females (Table 1).
Participant belief regarding association between risk factor and injury
Participants were asked to identify the three main causes of injury in their opinion. A total of 737 responses across 40 causes were provided, of which inadequate warm-up/cool-down and suboptimal muscle strengthening were most commonly cited (both = 93 (12.6%)). Overuse was listed 77 (10.5%) times, with related themes of inappropriate training (wrong amount/type) (n = 16 (2.2%)), insufficient cross-training (n = 13 (1.8%) and poor load management (n = 5 (0.7%)) also identified. Poor technique was cited 77 (10.5%) times, with inadequate stretching/flexibility (n = 54 (7.3%)), and poor fitness/conditioning (n = 37 (5.0%)), also frequently mentioned. Genre-specific causes such as unsuitable flooring (n = 33 (4.5%)), complex choreography (n = 30 (4.1%)), dance footwear (n = 20 (2.7%)), movement repetition (n = 19 (2.6%)), and over-dancing (exaggerated performance of steps) (n = 14(1.9%)) were identified. Fatigue (n = 27 (3.7%)) and insufficient rest between competitions or when injured (n = 11 (1.5%)), accidents (n = 18 (2.4%)), poor biomechanics (n = 14 (1.9%)), and a lack of appropriate education (n = 12 (1.6%) were also mentioned. An additional 21 potential causes of injury mentioned ten or less times included inadequate sleep, poor nutrition and diet, previous injury, an arduous competitive calendar and poor general health (Appendix 1).
When asked who was chiefly responsible for injury prevention, 217 (94.4%) participants said both the teacher and the dancer themselves. This was followed by parent/guardian n = 167 (72.6%)), governing bodies (n = 37 (16.1%)), physiotherapists (n = 28 (12.2%)), and other healthcare practitioners (n = 20 (8.7%)). Participants were finally asked to rate their own injury prevention knowledge, practice, and the quality of educational resources available to inform injury prevention in ID (Table 2). In the case of injury knowledge and practices, the majority of participants felt that they were in the moderate or good category (combined 72.6% and 80% for knowledge and practice respectively). However, 143 (62.2%) participants felt that available injury prevention educational resources were either poor or fair.
Participant opinion on injury prevention knowledge, practice, and standard of educational resource.
This is the first study investigating the injury knowledge and beliefs of ID teachers internationally. Given the substantial rate of injury in the genre as already established [2–11], and the lack of any related formalised educational or professional development requirements, an in-depth understanding of the perspectives of teachers is vital. This is particularly important as this research would suggest that teachers perceive that they act as key gatekeepers in the injury management of these dancers. This study has found that teachers possess generally good insight into the plethora of biopsychosocial risk factors associated with injury in ID, with varying degrees of awareness about the importance of each. There is much capacity to improve both the injury knowledge and practices of teachers, as well as the resources available to support teacher development in this regard. This is particularly important as teachers, along with their dancers and parents are identified as the stakeholders with most responsibility for injury prevention.
This study has revealed an accurate understanding of the anatomical location of injuries in ID, with some incongruence regarding the role of dancer sex in other aspects of injury. The perceived role of dancer sex in this study produced some interesting results. A large majority of participants identified no differences between the sexes in relation to the incidence, location or causes of injury. A number of studies in ID have investigated the association between dancer sex and injury [7, 9–12] with just two studies identifying an association between female sex and injury [9, 12]. This is however tempered by the comparatively small number of male Irish dancers, particularly at the elite level. This was referred to by a number of participants who stated that they had an insufficient number of male pupils to inform an answer to these questions. It was noteworthy that dance movements/ choreography were cited as a reason that the sexes would be both the same and different as each other in various facets of injury. In ID, there are many consistencies between the sexes in terms of the length and types of dances performed, the fundamentals of step execution and posture, and competitive events. However, females perform more steps on the top of their toes, in a position similar to the “en-pointe” movement in ballet, and wear different footwear than males for some dances. These shoes, called “light shoes” or “ghillies”, are flimsy leather laced pumps, with no shock absorption or foot support. The implication of these factors would seem to indicate greater challenges to females in terms of control and proprioception needed at the ankle, as well as increased ground reaction forces absorbed through the female lower limb. This is yet to be fully substantiated by empirical research and is an important area for further study.
When asked to rank the importance of various risk factors, participants favoured intuitive factors such as warm-up, strength, conditioning and flexibility, load management, and previous injury (Appendix 1). Warm-up has consistently been identified as an important measure in injury prevention and the research supports that it is widely practiced in ID [15]. However, evidence is lacking as to the nature and content of these warm-up sessions, and it is unknown how effective they may be. Research indicates that the warm-up performed by collegiate Irish dancers is markedly shorter than that performed by contemporary dance peers, but the impact of this is unknown [5].
Several studies have failed to establish any link between physical characteristics such as muscle strength, fitness or flexibility and injury in ID [9, 16]. This of course is not to say that these elements are not important for the wellbeing of the dancer, but may simply be less pertinent than some other factors. In particular, the overemphasis on flexibility is a potentially concerning finding, given the adverse nature of generalized hypermobility which is common in dancers, in the absence of appropriate neuromuscular control [17]. Interestingly, although previous injury was the risk factor that participants rated highest across combined strong/very strong categories (Table 1), it was only mentioned as one of the top three risk factors for injury by nine participants (Appendix 1). Previous injury is widely established across numerous dance genres as a key risk factor [10, 18] but this study may suggest that it is given less consideration than the training/physical characteristics of the dancer once the injury is resolved.
Overuse and suboptimal load management have been established as risk factors for injury in dance [19]. A pilot study in elite adolescent Irish dancers has shown an association between spikes in load and subsequent injury [6]. The same study also showed training patterns lacking appropriate periodization and load management. The ID competitive calendar is a year-round event of prestigious competitions, with no distinct downtime or rest period. Existing evidence in elite youth-sport points to an increased risk of injury and burnout in elite adolescent athletes who compete yearlong with inadequate rest and recuperation [20]. This is exacerbated in the case of uni-disciplinary athletes, as is the case with most elite Irish dancers, due to an inherent lack of cross-training and overload of the same muscle groups [21]. ID teachers are the main gatekeepers for the training load management of their students, and an educational intervention from an appropriately qualified professional who is familiar with the genre seems warranted.
A number of established risk factors for injury in dance more broadly were not ranked as important by participants (Table 1). These include social support, psychological health, and passion and motivation for dance. Research has shown that dancers with better social support from family, friends and dance peers possess superior coping strategies to overcome injury, and those lacking a robust social support network are less resilient to the impact of injury [22, 23]. These findings have been reinforced in recent qualitative work with Irish dancers, which emphasized the value of social support in managing adverse events including injury [24]. Relatedly, psychological distress has been associated with injury in a number of ID cohorts including professional Irish dancers [8] and collegiate students of ID [9].
Passion for dance is a common theme in dance literature and has previously been classified as either harmonious or obsessive [25]. In a study of Irish and contemporary dancers, participants mainly displayed a harmonious passion for dance [7]. However, a small minority from both genres exhibited an obsessive passion for dance, which has been associated with increased risk-taking behaviours, a reticence to engage with healthcare professionals when injured, and a tendency to continue to dance even when seriously hurt [25]. Chronic, persistent injury and compromised dance careers may result. Teachers must be educated to identify such individuals and take appropriate action if required. A related area is motivation for dance, which is dichotomized into ego-driven or task-driven motivation [26]. For the dancer motivated by ego, competition results and success are crucially important, and perceived failure may result in shame and compromised self-esteem [27]. In competitive ID, disappointment at some stage is largely unavoidable, and therefore, teachers again need to be mindful of the affect such an event may have on ego-driven individuals.
The importance of sleep [5] and general health [6, 10], both established risk factors for injury in ID, enjoyed only moderate recognition among these participants (Table 1). The association between nutrition and injury in ID has not been investigated, but research from other genres supports the importance of good dietary practices to prevent injury [28]. There is existing evidence to show that Irish dancers have very poor nutrition knowledge and practices, which is of concern when combined with a lack of teacher focus on diet [29]. Again, education from an appropriately trained professional would be welcome in this area.
It is evident from the responses in this survey that the quality of existing educational resources is perceived as suboptimal, and yet many participants felt that their injury prevention practices were good even though their knowledge was only moderate or fair. It is unclear whether there is any relationship between participants’ confidence in their knowledge and their criticism of resources, as this study did not collect information on the specifics of any training undertaken. However, it is reasonable to suggest that appropriate, high quality injury prevention guidance which considers the broad plethora of potential risk factors is likely lacking in ID, and is an area that requires input and focus from all stakeholders.
Generic programmes to improve teacher training such as the “Healthy Dance Practitioner” certificates from Safe in Dance International are available but it is unknown whether the ID community engages in these educational programs or not. Ideally, given the overwhelming number of teachers who subscribe to the main governing bodies for ID, these organisations are best placed to lead on teacher education via their existing social networks and information dissemination systems. Any such educational programmes would require input from a broad range of experts addressing the important role of the aforementioned risk factors in the overall biopsychosocial wellbeing of the dancer. This may involve a range of health professionals including physiotherapists, medics, dieticians, psychologists, podiatrists etc. as well as other professionals in the areas of sports, strength and conditioning training.
Limitations
Participants overwhelmingly came from regions where ID is long established; therefore, it is unknown if the same findings apply in places where ID is less commonly practiced. Selection bias is likely as those more interested in the topic area were more likely to participate. In terms of data gathered, warm-up and cool-down should have been presented as separate entities, as they appear to be viewed quite separately by participants in terms of importance. Additionally, no definitions were provided for the majority of risk factors presented in the questionnaires which may have led to varying interpretations of what these risk factors actually meant. A concise and detailed description of risk factors is recommended for future studies. More information about the type of injury prevention/management education or training undertaken by participants would have added valuable insight into if, what, how and where teachers are accessing information.
Conclusion/summary
ID teachers are well aware of the impact and extent of injury in ID, with an appreciation of the wide array of potential risk factors involved. It is encouraging that overuse and improper training are recognised as serious issues in ID, and suggests a role for clinicians and trainers in guiding appropriate load management, periodization and training. There appears to be an overemphasis on the physical traits of the dancer (strength, flexibility, fitness) with lesser attention given to important factors including sleep, previous injury, nutrition, and general and psychological wellbeing. This is despite the fact that teachers appear to recognise the strong association with injury represented by a number of these risk factors. Education and training from multidisciplinary healthcare practitioners and other professionals from the world of sport and athletic training is recommended to instill a deeper understanding of the holistic nature of injury prevention and performance optimization.