
Abstract
BACKGROUND:
Posterior shoulder tightness as demonstrated by glenohumeral internal rotation deficit (GIRD) is a common contributor to many shoulder pathologies in overhead throwing athletes.
PURPOSE:
This study aimed to assess immediate effect of combining glenohumeral and scapulothoracic mobilization with stretching on improving internal rotation range of motion (ROM) in overhead athletes with GIRD
METHODS:
This study was a single-blind randomized controlled trial with parallel groups. The participants were 30 asymptomatic male volleyball players who had a loss of shoulder internal rotation ROM of 15 degrees or more on their dominant compared to their nondominant side. They were randomly assigned to 1 of 2 groups: stretching only (n = 15) or stretching plus joint mobilization (n = 15). Participants in the stretching group performed cross-body stretches, and those in stretching plus mobilization group were treated with both cross-body stretching and mobilization techniques for the glenohumeral and scapulothoracic joints. Both groups received the intervention every other day for 1 week. Shoulder internal and external ROM were measured before and after the intervention.
RESULTS:
Before the intervention, dominant-side deficits in internal rotation ROM compared to the nondominant side were 20.11±5.27 degrees in the stretching group and 21.87±8.06 degrees in the stretching plus mobilization group. After the intervention, internal rotation ROM deficit between the dominant and nondominant side decreased to 11.28±5.82 in the stretching group (P < 0.001) and 10.85±9.19 in the stretching plus mobilization group (P < 0.001). However, the between-group difference was not statistically significant (P = 0.389). External rotation ROM remained unchanged in both groups (P > 0.05).
CONCLUSION:
Both interventions (stretching and stretching plus mobilization) can have the same beneficial effect in decreasing GIRD in asymptomatic overhead athletes.
Introduction
Physical examination of the shoulders of overhead sports players consistently demonstrates asymmetric glenohumeral (GH) rotation range of motion (ROM) [1]. Throwing athletes typically have significantly decreased internal rotation in their dominant (throwing) arm compared to their nondominant arm [1, 2]. This loss of GH internal rotation in the throwing shoulder is known as glenohumeral rotation deficit (GIRD) [3]. Studies have reported that GIRD may be a predisposing factor for multiple injuries in overhead athletes [2–4]. Although the reason for this altered ROM is not clear, both bony and soft tissue changes are believed to be associated with GIRD [5].
Several studies have described increased humeral retroversion in association with repetitive overhead throwing in young athletes [5–7]. Increased humeral retroversion is defined as an increase in the angle between the axis of the elbow joint and the axis through the center of the humeral head [6], allowing the arm to externally rotate to a greater extent and internally rotate to a lesser extent in maximum cocking rotation before being constrained by capsuloligamentous restraints [5, 7]. In addition to humeral retroversion, another major contributor to GIRD is posterior shoulder tightness, which can result from muscular stiffness or thickening of the posteroinferior portion of the GH joint capsule, which causes improper shoulder deceleration leading to repetitive microtrauma [3, 8]. Tightness in the posterior structure of the shoulder is currently understood to be a cause of GIRD [9, 10].
Current evidence shows that in overhead athletes, GIRD is associated with shoulder injuries such as rotator cuff injury, superior labral tears, and biceps tendinosis [9–11]. Although it is uncertain what degree of reduction in ROM is associated with a given injury, studies have shown that an internal rotation deficit of up to 15 degrees may be indicative of normal GIRD in overhead athletes [12–14], but an internal rotation deficit of more than 20 degrees is considered pathologic [3, 15]. Prospective studies have demonstrated that the risk of injury is fourfold greater when the internal rotation deficit is greater than 20 degrees [4, 16]. Therefore, finding an effective treatment to reduce posterior shoulder tightness is important and may help prevent impingement-type injuries.
Several studies recommend posterior shoulder stretching exercises to restore internal rotation ROM loss [1, 17–19]. Different stretching methods including towel, sleeper and cross-body stretching have been used for posterior shoulder tightness [3, 17]. Another intervention that has been suggested to increase joint mobility is joint mobilization, which is known to produce greater mobility of soft tissues and capsular joints [20]. Some authors have proposed that loosening posterior shoulder tightness with GH mobilization techniques allows the humeral head to glide in the appropriate direction and thus favors normal GH arthrokinematics [18, 21].
Moreover, since shoulder girdle mobility requires good coordination between the scapulothoracic (ST) and GH joints [22] and there is evidence that abnormal scapular movements impairs normal shoulder function [23] effect of ST mobilization on shoulder ROM has been investigated in some studies [24, 25]. Aytar et al. (2015) compared the effect of ST mobilization techniques and supervised exercises in patients with subacromial impingement, and found that both methods were beneficial in increasing shoulder ROM [24]. Yang et al. (2012) reported that a combination of ST mobilization and standard physical therapy resulted in greater improvements in ROM in people with frozen shoulder [25].
However, there appear to be no studies to date that focused on ST mobilization in people with GIRD. Therefore this study aimed to assess immediate effect of combining glenohumeral and scapulothoracic mobilization with stretching on improving internal rotation ROM in overhead athletes with GIRD. We hypothesized that adding ST and GH mobilization to stretching would lead to greater improvements in ROM compared to stretching alone.
Methods
Study design
This study was a single-blind randomized controlled trial registered in the Iranian Registry of Clinical Trials (trial registration number IRCT2016050724149N31). The study protocol was approved by the Ethics Committee of Shiraz University of Medical Science (IR.SUMS.REC.1394.169).
Participants
Competitive male volleyball players were recruited as participants for this study. The inclusion criteria were age between 18 and 35 years, right-side dominance, and internal rotation ROM deficit of 15 to 20 degrees on the dominant side compared to the nondominant side measured at 90 degrees of abduction [2]. A 15-degree deficit in internal rotation can be considered a significant amount of GIRD, and this criterion also made it possible to recruit healthy athletes because it is less than the GIRD considered pathologic (20 degrees) [3, 15]. Participants were excluded if they had a history of shoulder pain during the previous 6 months, shoulder and neck surgery, trauma or fracture in the shoulder girdle within the previous year, or radicular pain from the cervical vertebrae. All participants were screened and interviewed by a certified physiotherapist. The study procedures were described to all participants, and they were enrolled after providing their written informed consent. All participants completed a questionnaire with items covering demographic information (age, height, weight) and information on their sport activity (sports experience, number of sports sessions per week, minutes of exercise in each session).
Randomization
The participants were assigned randomly to the stretching group or stretching plus mobilization group by block randomization with a block size of 4. The randomized list was provided by a researcher who was not aware of the treatment process. One physiotherapist with at least 5 years of clinical experience in the field of manual therapy performed all treatments in this study, and two other physiotherapists who were blind to the group allocations performed all measurements. However, it was not possible to blind participants owing to the nature of the interventions. All participants were informed that they would receive one of the two treatment interventions.
Procedure
Intervention
Participants were recruited through advertisement on the sports club bulletin board and referred to the physiotherapy clinic at the School of Rehabilitation Sciences of Shiraz University of Medical Sciences. Participants were allocated randomly to the stretching group (stretching only) or stretching plus mobilization group (stretching and GH and ST mobilization). Both groups received the treatment for 3 sessions every other day during1 week.
Stretching
The sleeper stretch and cross-body stretch are the most common forms of stretching [26]. Meclure et al. compared stretching techniques in individuals with limited shoulder internal rotation, and found the cross-body stretch to be the most effective technique [17]. We therefore used this technique to stretch the posterior shoulder. The participants were given a standardized intervention and visual demonstration of the cross-body stretch. All stretches were performed in the standing position on the dominant side, and participants were asked to pull their humerus into horizontal adduction with their opposite hand placed beneath their stretched arm. They were instructed to perform the stretching exercise to the point of mild discomfort. The stretch was held for 30 seconds and repeated 5 times with a 30-second rest between each movement [17]. Stretching exercises were performed in front of a mirror with supervision by the physiotherapist.
Mobilization
Mobilizations were performed by the physiotherapist. Glenohumeral joint mobilization in the dorsal glide direction was performed with the participant in supine position with his shoulder flexed and horizontally adducted, and his elbow flexed. A wedge was placed under the dorsal scapula [27]. For ST mobilization, the participant was in side-lying position with the involved limb accessible to the physiotherapist. The physiotherapist stood in the front of the patient and placed her index finger under the medial scapular border, with the inferior angle of the scapula in the web space. With her other hand the physiotherapist grasped the superior border of the scapula and moved the scapula superiorly and inferiorly for superior and inferior glide, and medially and laterally for medial and lateral glide. Then the scapula was rotated upward and downward for scapular rotation. All techniques were applied and maintained at grade 4 [28]. Three sets of 10 repetitions were used for each technique, with a 30-second rest period between sets [24]. The end position in each technique was held for 5 seconds, and there was a 3-second rest between each technique in each set.
Outcome measures
The outcome measures were internal rotation and external rotation ROM, recorded in both groups at baseline and after treatment was completed. At baseline, internal and external humeral rotation were measured in both the dominant and nondominant limbs, and after treatment rotation was measured only on the dominant side in both groups.
2.4.4.1. Shoulder internal and external rotation range of motion: Internal and external rotation were measured by digital photography. Antonietti et al. (2014) showed that photography is more reliable than goniometery for assessing shoulder internal and external rotation [29]. The participant lay supine on a treatment table with his hip and knee flexed at 90 degrees. The shoulder to be examined was kept in 90-degree abduction and the elbow in 90-degree flexion. In the starting position, the participant’s arm was placed in position with the forearm perpendicular to ground. Two adhesive reflective marker were placed on the ulnar styloid process and the olecranon process. To assess internal rotation, the examiner passively rotated the shoulder internally with one hand and fixed the scapula by pushing the anterior aspect of the shoulder joint toward the table with the other hand. The end range of internal rotation was defined as no further rotation or when the coracoid process started to move anteriorly [1] (Fig. 1).

Measurement of passive internal rotation.
At the end of internal rotation, a second investigator took a photograph with a digital camera (Kodak, M5350). The camera lens was positioned opposite the olecranon at a distance of 3 feet from the table and at the same height as the table. Images were analyzed with the IMAGEJ computer program (1.44 p). This public-domain image processing and analysis program, developed at the US National Institute of Health (NIH), was used to calculate the angles between anatomical landmarks [30]. Three trials of passive internal rotation were conducted, and the mean of all 3 trails was calculated. External rotation was measured with techniques similar to those for internal rotation (Fig. 2).

Measurement of passive external rotation.
The study sample size was calculated with the G* Power program 3.1.9.2 (G power program Version 3.1, Heinrich-Heine-University Düsseldorf, Düsseldorf, Germany). Sample size calculation was based on a previous study in which there was a 32% difference in internal rotation improvement between the stretching and control groups [17]. The estimated sample size to achieve a statistical power of at least 80% at an α level of 0.05 was 24 participants (12 in each group). Accordingly, 30 participants were recruited to account for a potential dropout rate of 25%.
Statistical analysis
All statistical analyses were done with the Statistical Package for the Social Sciences version 23 (SPSS, Inc., Chicago, IL, USA). Data normality was checked with the Shapiro–Wilk test. Some data did not meet the criteria for normal distribution. Thus, nonparametric tests were used. Baseline variables were compared between the stretching group and stretching plus mobilization group with Mann–Whitney U tests. In each group, differences between pre-intervention and post-intervention values were analyzed with the Wilcoxon signed rank test. The Mann–Whitney U test was used to evaluate between-group differences. The significance level for all statistical tests was set at P < 0.05.
Results
Sixty-eight athletes were recruited and screened for group assignment (Fig. 3).
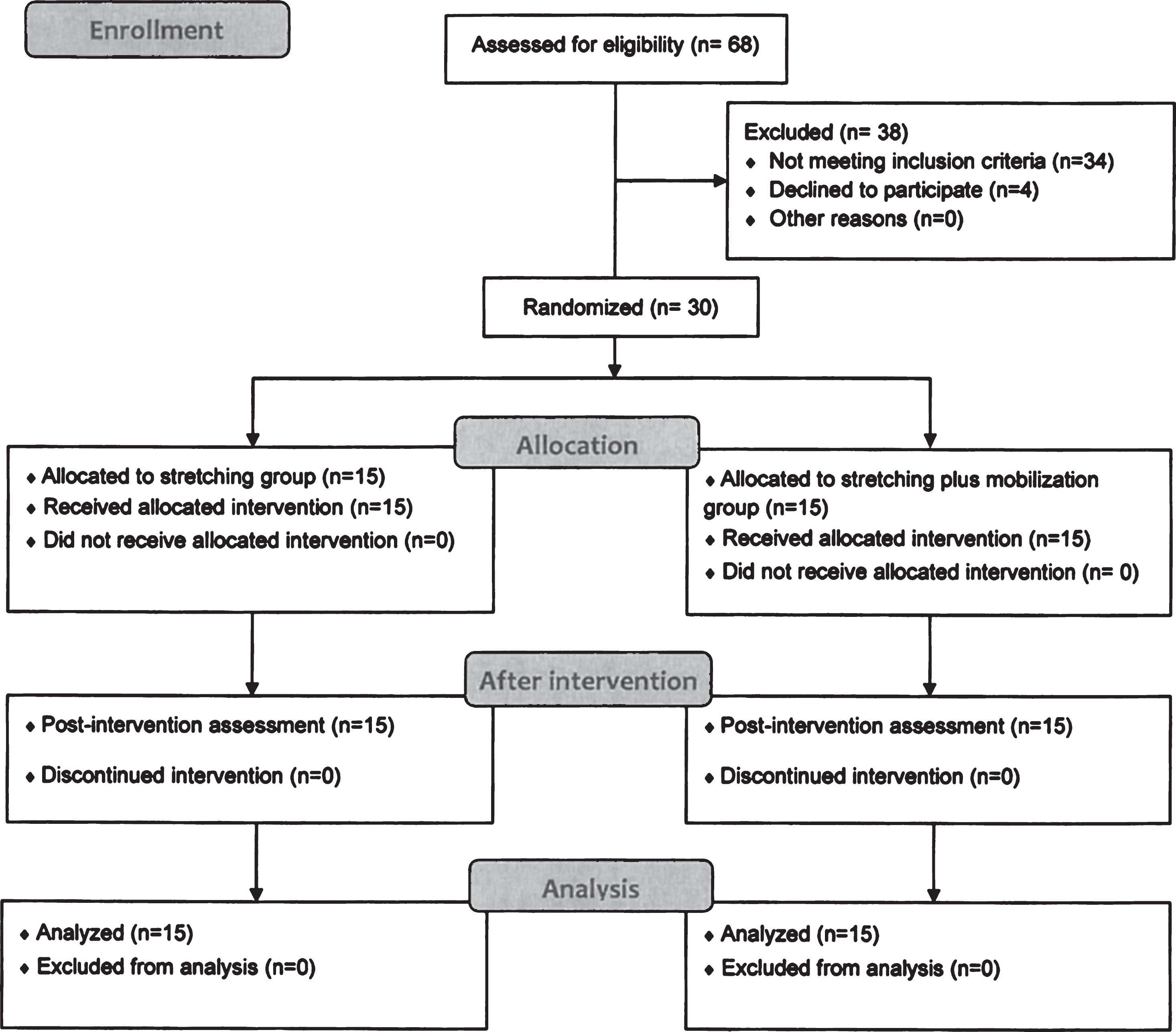
Flow diagram of the study.
The athletes’ demographic data and information on their sports activity are shown in Table 1. There were no significant differences between groups at baseline in age, weight, height, number of sports session per week, duration of exercise in each session, or the number of years of sports experience.
Comparison of demographic and sport activity information of participants in both groups at baseline
Values are given as the mean±standard deviation.
Descriptive statistics for internal and external rotation ROM in the dominant and nondominant limbs, and for GIRD and external rotation gain in both groups, are presented in Table 2. GIRD and external rotation gain were computed by subtracting internal and external rotation ROM on dominant side from the nondominant side. GIRD shows the amount of loss of internal rotation ROM on dominant side compared to the nondominant side, and external rotation gain shows amount of increase in external rotation ROM on the dominant side compared to the nondominant side. No significant differences in these variables were observed between groups at baseline (Table 2).
Comparison of glenohumeral rotation in the dominant and nondominant limb in both groups at baseline
Values are given as the mean±standard deviation. GIRD, glenohumral internal rotation deficit; ERG, external rotation gain.
After the intervention, internal rotation ROM on the dominant side was significantly greater in both the stretching group (P < 0.001) and stretching plus mobilization group (P < 0.001), but the difference between groups was not significant (P = 0.436) (Table 3). Decreases in GIRD were seen in both the stretching group (P < 0.001) and the stretching plus mobilization group (P < 0.001); however, there was no significant difference between groups (P = 0.389) (Table 3).
Within-group and between-group differences in the changes in glenohumeral rotation in the dominant limb after the intervention
Values are given as the mean±standard deviation. GIRD, glenohumral internal rotation deficit; ERG, external rotation gain.
No significant difference was observed in external rotation ROM on the dominant side or external rotation gain between pre-intervention and post-intervention values in either group (P > 0.05) (Table 3).
This study demonstrated improvements in GH internal rotation on the dominant side in both the stretching and stretching plus mobilization groups, but the difference between groups was not statistically significant. The dominant side in participants in this study had a GIRD of 20.98±6.7 degrees, a deficit very close to the 20-degree value proposed by Burkhat et al. (2003) [3]. Improvements in internal rotation after the intervention were seen in both groups, which is in agreement with previous research showing that internal rotation deficit is responsive to conservative treatments [18, 31].
The amount of external rotation gain in this study was small at only 2 degrees, and there was no change in shoulder external rotation in either group, a finding consistent with results reported by McClure et al. (2007) who found no change in external rotation [17]. When a loss of internal rotation results in a concomitant gain in external rotation, function of the throwing shoulder is not affected [32, 33], However, when the amount of internal rotation loss exceeds any gain in external rotation, this condition can become problematic in the throwing shoulder and result from thickening of the posterior GH joint capsule [3]. Regarding the small pre-intervention gain in external rotation and lack of post-intervention change in external rotation ROM, the improvement in internal rotation in both groups studied here can be attributed to changes in the posterior GH joint capsule.
We found no advantage of combined ST and GH mobilization over stretching alone in increasing internal rotation ROM. After the intervention, GIRD in both the stretching and stretching plus mobilization groups decreased to 11.28±5.82 and 10.85±9.19 degrees, respectively. This means that the athletes responded well to both interventions, and their internal rotation deficit was lowered to an acceptable level. A difference in motion loss of less than 15 degrees between the shoulders is considered an acceptable outcome Manske et al. (2010) compared the effects of stretching plus mobilization with stretching alone, and as in the present study, found no additional effect of GH joint mobilization combined with cross-body stretching in improving internal rotation ROM in asymptomatic persons with GIRD [18]. We hypothesized that combining ST and GH mobilization techniques would result in more improvement in internal rotation compared to stretching alone. Joint mobilization techniques are assumed to induce various beneficial effects such as breaking up adhesions, releasing collagen, and increasing fiber glide [34]. However, our hypothesis was not supported. In contrast to our results, Bailey et al. reported that the added use of manual therapy with stretching produced a greater increase in internal rotation ROM compared to stretching alone [31]. Methodological differences between these two studies may account for the difference in findings. In the present study we assessed internal rotation ROM after a 1-week intervention with stretching and mobilization, whereas Bailey et al. (2017) assessed the immediate effect of stretching and instrumented manual therapy on internal rotation ROM. Moreover, the dominant-side deficit in internal rotation ROM was 20 degrees in the present study, but was 26 degrees in the study by Bailey et al (2017). A study by Cools et al. (2012) compared the effect of stretching and mobilization techniques on improvements in internal rotation in symptomatic and asymptomatic athletes. These authors found that both techniques significantly increased internal rotation ROM, although the improvement in internal rotation ROM in symptomatic athletes was smaller compared to asymptomatic athletes [21]. They concluded that symptomatic athletes were less responsive to the treatment or dose of treatment provided [21]. Thus, we speculate that a combination of these interventions may be more beneficial in restoring internal rotation ROM in symptomatic patients or athletes with greater internal rotation deficits. However, further studies are needed to clarify this issue.
Limitation
This study had some limitations. Our participants were asymptomatic male volleyball athletes between 18 and 35 years old; thus we cannot be certain that our results are generalizable to the whole population. Also, in this study only immediate effect of mobilization and stretching was investigated, future studies with follow up period are needed to determine both short term and long term effects of these interventions on improving ROM. Finally, we did not measure posterior capsule tightness or scapular mobility, thus future studies are needed to investigate the direct effect of GH and ST techniques on these factors.
Conclusion
The results of this study show that both stretching alone and stretching plus joint mobilization can significantly increase shoulder internal rotation after 1 week of intervention in a group of asymptomatic overhead athletes. Our results also suggest that joint mobilization techniques do not have an additive effect on improvements in shoulder internal rotation.
Footnotes
Acknowledgments
This work was based on the MSc Dissertation prepared by Narjes Ghasempour, and was financially supported by Shiraz University of Medical Sciences (Grant No. 94-01-06-9719). We thank K. Shashok (AuthorAID in the Eastern Mediterranean) for improving the use of English in the manuscript.
Conflict of interest
The authors have no conflicts of interest to declare.