
Abstract
BACKGROUND:
The number of rotator cuff repairs performed worldwide is increasing every year. However, there are still controversies regarding when rehabilitation after surgery should start.
OBJECTIVES:
To assess and to compare clinical and biomechanical outcomes of patients who were randomised and allocated to early or conservative rehabilitation after rotator cuff repairs.
METHODS:
Twenty patients were randomised to two treatment groups. The biomechanical assessments were performed before surgery and at three and six months, consisting of 3D kinematics and muscle activity from 5 muscles (upper trapezius, anterior deltoid, middle deltoid, posterior deltoid and biceps brachii) from six movement tasks. In addition, the Oxford Shoulder Score and EQ-5D-5L were also recorded. At 12 months an ultrasound scan was performed to check the repair integrity.
RESULTS:
Overall, both groups had similar results for function and health-related quality of life. However, at six months patients in the early group had better range of motion (ROM) than those in the conservative group, especially for shoulder flexion (Early: median = 152.1° vs Conservative: median = 140.0°). The number of re-tear events was higher in the early group (5 vs 1), and of these only two patients reported symptoms at 12 months.
CONCLUSION:
Early rehabilitation may improve ROM but it does not seem to be superior to a conservative management in improving function and quality of life. In addition, more re-tear events were observed in the early group. However, the results should be interpreted with caution due to the small sample size.
Introduction
Rotator cuff tear is a common disorder affecting approximately 30% of people older than 60 years [1] and it is responsible for almost 450,000 operations per year in the US [2]. Rotator cuff tear can be debilitating and impair patients’ quality of life and function; if initial non-operative treatments fail, surgical repair is often recommended [3]. However, for optimal results, the postoperative rehabilitation must be adequately planned to help patients with their recover and return to daily activities [4].
Following a rotator cuff repair, a period of movement restriction is advised [5]. Using a sling for six weeks is encouraged to protect the tendon and allow adequate soft-tissue healing and possibly avoid a re-tear [6]. In contrast, delaying mobilisation may increase the risk of shoulder stiffness and potentially postpones improvements in function and return to work [7]. Based on the available evidence, it is difficult to make an informed clinical decision on the most favourable postoperative time to start physiotherapy and reduce the use of sling. An overview of systematic reviews with updated meta-analyses demonstrated that, currently, there is almost the same number of systematic reviews compared with randomised controlled trials (RCTs) published on the topic, with reviews and primary studies showing conflicting conclusions [8].
In a clinical setting, it is common to use questionnaires to screen patients’ impairments in activities of daily living (ADL) and goniometers to quantify range of motion (ROM). These tools have the advantage of being easy to use and are relatively inexpensive; however, their simplistic capacity for measurement may not objectively define how patients are affected and how they are recovering. For instance, the deltoid and upper trapezius muscles are activated for longer periods in patients having surgery for rotator cuff related problems but there is a lack of studies investigating if an early postoperative structured exercise program could be more effective than a conservative in readjusting the activity of the shoulder muscles [9, 10]. Considering the uncertainties related to the application of early rehabilitation following rotator cuff repairs, and the lack of information on how different timing of starting physiotherapy affect muscle activation and quality of movement during ADLs after surgery; this study aimed to investigate the effectiveness of a therapist-led early rehabilitation regime compared with a conservative management on clinical and biomechanical outcomes.
Methods
This study was an RCT which followed the CONSORT statement [11]. Ethical approval was gained (16/NW/0143) and it was registered in the clinicaltrials.gov database (NCT02631486). The patients’ recruitment and screening for eligibility were made on the same day that patients attended their scheduled appointments with the consultant regarding their shoulder symptoms and need for surgery. Potential patients were approached and informed about the study, this included what would happen if they agreed to take part and how their rehabilitation would progress. All participants signed an informed consent form after the study details were explained and any questions from the patient were addressed.
Eligibility criteria
The inclusion criteria consisted of 1) males and females aged between 40 and 70 years old (most common age range for rotator cuff tears) [1], 2) on the waiting list for a rotator cuff repair for a chronic tear (symptoms for > 3 months), 3) with no other previous shoulder surgery on the same side, and 4) no other musculoskeletal impairment on the assessed limb or in the cervical and thoracic spine. Patients were excluded if 1) during the surgery a repair was deemed not needed or the tear was too extensive to allow early rehabilitation, 2) they had previous shoulder surgery and/or other musculoskeletal impairment on the assessed limb or in the cervical and thoracic spine, and 3) were unable to follow instructions.
Intervention
Rehabilitation consisted of two groups who received physiotherapy post-surgery with a planned frequency of once every two weeks, lasting for approximately 3–4 months. In the first stage (discharge to 4 weeks), patients in the Early group used the sling for comfort only, which could be discarded when the patient felt comfortable and confident in doing so; whereas the Conservative group was asked to remain in the sling until the 6th week and remove it only to perform the prescribed exercises. The full protocols are available in the Supplementary file A. Treatment compliance and adherence were checked at the follow-up assessment sessions and were based on patients self-report on sling usage and attendance to physiotherapy.
Randomization and allocation concealment
A sequence of random numbers (www.randomization.com) was generated by an independent research team member (JR) who was also responsible for the allocation concealment. The opaque sealed envelopes were opened after surgery by one of the treating physiotherapists who was not involved with the study design or data analysis.
Procedures
Four assessment sessions were undertaken in the outpatient setting at baseline (before surgery), three, six and 12 months follow-up. The first three assessment sessions consisted of completing the Oxford Shoulder Score (OSS) for function, the EQ-5D-5L for health-related quality of life and a biomechanical assessment. The OSS is a 12 item questionnaire about pain and function commonly used in randomised controlled trials. It is valid, reliable and showed good responsiveness [12, 13]. The EQ-5D is a generic questionnaire about quality of life which has been extensively used and researched and validated [14, 15]. The assessments were led by an assessor (BM) who was blinded to patients’ allocation until the final data analysis. The last assessment session at 12 months consisted of an ultrasound scan only. The scans were performed by a single Fellowship-trained Musculoskeletal Radiologist (SB), blinded to patient’s group allocation, using a GE Logiq S8 ultrasound scanner (General Electric Healthcare; Chicago, United States of America).
Biomechanical assessment
The biomechanical assessment used two different systems that were synchronized; the Xsens MVN system (Xsens Tech®, Enschede, Netherlands) motion capture system which recorded upper body kinematics at 120 Hz, and the Trigno (Delsys®, Boston, USA) wireless EMG system which recorded muscle activity at 2000 Hz. Every participant performed six shoulder movements and repeated each of them five times at a comfortable self-selected speed. The decision about using the tasks described in Table 1 was based on what is generally used during routine clinical assessments and common tasks used in everyday life that were assessed in similar studies [16–18]. After determining the ROM (humerus in relation to the thorax) in degrees for each repetition, an average was calculated. For the EMG analysis, the muscles chosen were the anterior (AD), middle (MD) and posterior (PD) deltoids, upper trapezius (UT) and biceps brachii (BC). These muscles are easy to access and are sensitive to changes to the rotator cuff muscles activation [19]. The integral was calculated and expressed as a percentage of the peak value [20]. All sensors were placed on each participant by the same assessor at every assessment session.
Range of motion tasks
Range of motion tasks
The primary outcome was shoulder ROM during flexion at 6 months. Based on a similar study [4], 14 patients would be needed in each group to detect a minimal clinically important difference (MCID) of 25° of flexion ROM, with a standard deviation of 23.6° at the 5% significance level, with 80% power. Adding 20% for eventual follow-up loss, the final total sample needed was 34 participants.
Statistical analysis
Considering the number of patients recruited in each group and the number of patients that were reassessed at the follow-up points, descriptive statistics were preferred [21]. We followed the intention-to-treat principle to report all outcomes.
Results
Ninety-nine patients were assessed for eligibility between May 2016 and January 2017; 57 were excluded as they did not agree to take part in the study. From the remaining 42, a further 22 were excluded: 17 did not need a rotator cuff repair and 5 had a massive tear, which were considered inappropriate for the early mobilisation protocol. Therefore, 20 patients were randomised, 10 per group (Fig. 1).
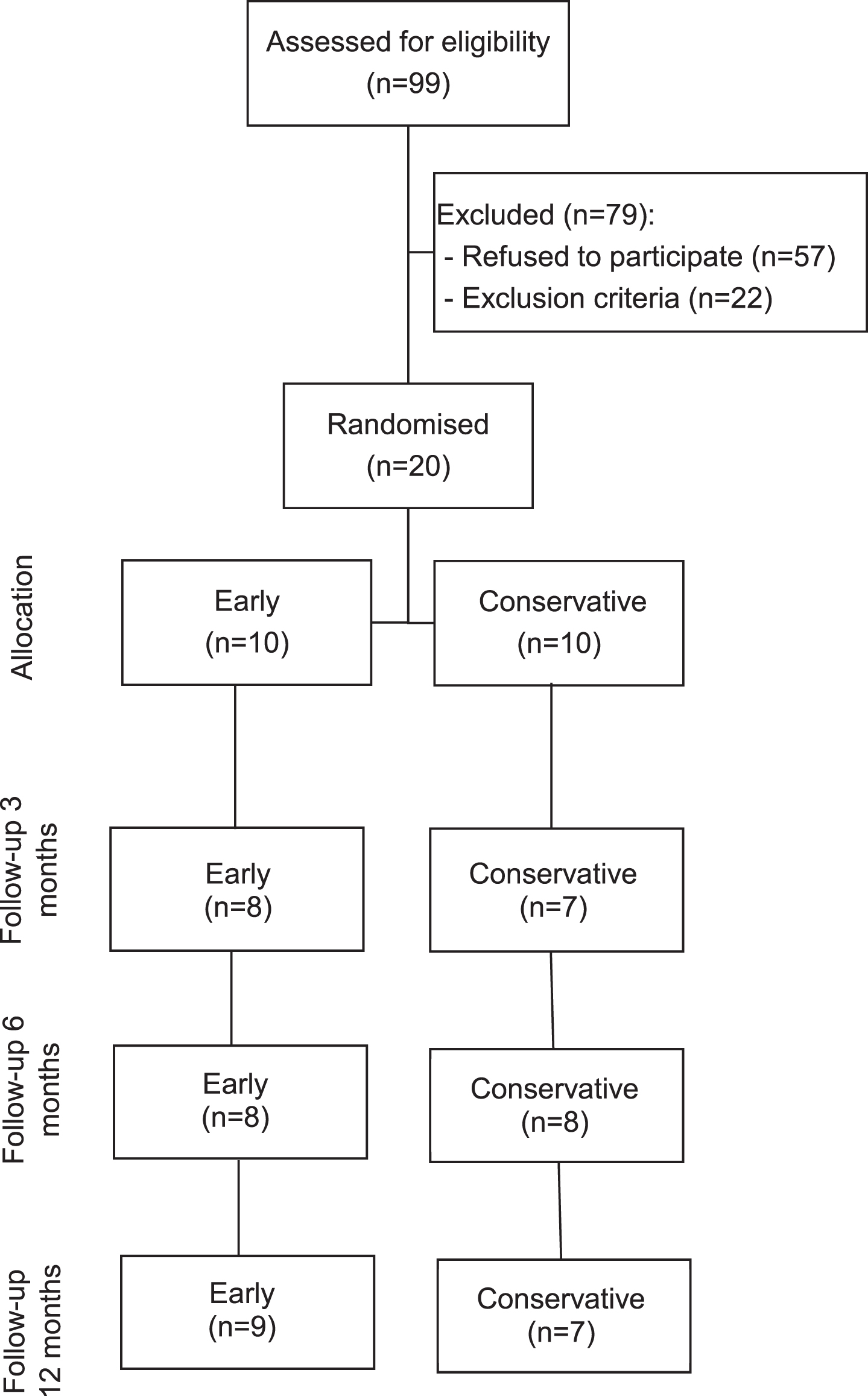
Flow diagram of patient recruitment, allocation and analyses.
Table 2 shows the demographic details at baseline. Most of the variables were similar between groups; there was a substantial difference in the length of time from first symptoms until the date of surgery and the Early group had more smokers than the Conservative group. Based on the surgeons’ reports for the repairs, the most common lesions were found in the supraspinatus combined with the infraspinatus (Table 3).
Baseline characteristics
Baseline characteristics
SD: standard deviation.
Surgery characteristics
SAD: subacromial decompression.
Seventy percent of patients in the Early group used the sling for less than 4 weeks and 88% of patients in the Conservative group used for at least 6 weeks (Table 4). Patients in the Early group reported a usage of 8.7 (SD = 10.6) hours per day (h/d) in comparison to 22.1 h/d (SD = 3.5) in the Conservative group. The Early group had an average of 6.5 (SD = 2.9) sessions with a physiotherapist and the Conservative group had an average of 8.7 (SD = 4.3).
Self-reported sling usage
Self-reported sling usage
A large improvement from baseline was observed for both groups on both follow-ups for the OSS. Both groups had better scores for the EQ-5D-5L compared to baseline with equivalent values at 6 months (Table 5).
Questionnaires and ROM results
Questionnaires and ROM results
IQR: interquartile range, OSS: Oxford Shoulder Score.
Combing
At three months, the Conservative group showed slightly better ROM and higher muscle activity for the PD. At six months, the Early group had better ROM (6.7° between groups difference) and similar muscle activity apart from the BC, which showed 18% higher activity in the Conservative group (Supplementary file B).
Abduction
Similar to the results of the Combing task, the Conservative group had better ROM at three months (7.6° between groups difference) and the Early group at six months, (14° between groups difference). At three months, the Conservative group showed higher muscle activity for all muscles. At six months, the Early group showed higher activity of the AD, MD and BC, with between groups differences of 15%, 9.6% and 25.8%, respectively.
Carrying
For the Carrying task, the Conservative group showed higher ROM and EMG activity at three and six months, although the between groups differences for ROM were small; 0.2° and 1.9°, respectively. The largest difference between groups for muscle activity was 18.8% for the MD at six months in favour of the Conservative group.
Reaching
The Early group had better ROM and muscle activity for the PD at three months (4.9° and 11.7% between groups difference) and the Conservative at six months (2° and 9.3% between groups difference).
Flexion
Comparing the follow-up values with baseline, the Early group improved 25° at three months and over 45° at six months. In contrast, the Conservative group had a reduction of approximately 6° at three months and an improvement of 9° at six months. The main between groups differences for muscle activity was for the MD (13.9% in favour of the Conservative group) at three months and for the AD (20.1 % in favour of the Early group) and the PD (13.4% in favour of the Conservative group) at six months.
Lifting
Comparing follow-up values with baseline, the Early group improved 40.7° at three months and 68.9° at six months, while the Conservative group got worse at three months by 9.5° and improved by 9.6° at six months. The main between groups differences for muscle activity was observed for MD (19.8%) in favour of the Conservative group, and PD (12.1%) in favour of the Early group at 3 months. At six months, the Early group showed greater activity for AD, MD and BC (28.4%, 14.2% and 20.4%, respectively).
Repair integrity
Sixteen patients (Early n = 9; Conservative n = 7) had an ultrasound scan and six re-tears were found (Early n = 5, Conservative n = 1). Based on patients self-report, only 2 patients, both from the Early group, reported any symptoms; all the others confirmed that they were satisfied and had no pain or difficulties with activities involving the shoulder.
Discussion
The study aimed to assess and to compare outcomes of patients who had a rotator cuff repair and were randomised to either early or conservative rehabilitation. We found that the majority of patients reported adhering to the use of the sling as per instructions, which corroborates with the study of Mazzocca, Arciero [22]. In their study, the authors reported that the majority of patients in the trial comparing early with conservative rehabilitation following rotator cuff repairs also used the sling as requested. Although the information on sling usage from our study is important, it relies on patients’ self-reported information, which may be prone to inaccuracies.
Overall, both groups improved self-reported function at both follow-ups with similar results at six months. However, it could be observed that the Early group continued to improve over time, while the Conservative group did not improve further at six months. Both groups improved above the OSS MCID of six points from baseline to six months [23, 24]. Previous studies that have evaluated the effectiveness of rotator cuff repairs only have shown that the surgery is effective in improving function and quality of life of patients [25–27]. Other RCTs on the topic have used different questionnaires, which limit direct comparisons. However, based on the MCID of each scale some estimations are possible. For example, the MCID for the Constant-Murley Score (0–100), is 11 and for the Simple Shoulder Test (0–12) is 2.2 points [23, 24]. Using this approach, it is possible to observe the same trend on the RCTs reported by Kim, Chung [28] and Koh, Lim [29]. These authors did not find statistically significant differences between groups at follow-ups, but both groups in both studies improved more than the MCID after 6 months.
Trying to compare the biomechanics results of the ADLs from this RCT to other studies is challenging due to the lack of similar design and hypotheses tested. Most studies with a similar method of assessment compared differences between healthy groups with patients who had the injury but were still untreated or compared patients after surgery versus healthy groups. For example, Vidt, Santago [30] assessed 7 functional activities comparing patients with rotator cuff tears to a healthy control group, which included two similar tasks (combing and upward reach) to those used in our study. Their results showed that for upward reaching, which was similar to the Flexion and Lifting tasks, patients with rotator cuff tears had approximately a 60° range of motion in the sagittal plane. Another study, from Fritz, Inawat [31], measured 3D kinematics and EMG at 9–12 weeks post-surgery for 10 patients who had rotator cuff repairs compared to 10 healthy subjects. The authors assessed 10 activities which included Combing and Reaching, with patients showing a lower ROM for Combing, Reaching and for all the other tasks included in their study. From the six tasks proposed in our study, a clear pattern was observed where the Early group continually improved their ROM at every follow-up time point for all tasks excepting for Reaching. Whereas the Conservative group showed a slight deterioration at 3 months for the tasks Carrying, Flexion and Lifting, and at 6 months for Combing; Abduction was the only task to improve in the Conservative group at both follow-up time points.
At three months, the differences in ROM between groups were generally small. Nevertheless, at six months, substantial differences of 14° for Abduction, 12.1° for Flexion and 13.8° for Lifting were observed. The MCID for shoulder flexion reported by Muir, Corea [32] is 14° when measured with a goniometer. Considering that the glenohumeral relative angle was defined as the humerus in relation to the thorax, it could be possible that the difference between groups for ROM are clinically important; however, such analysis is beyond the scope of our study and the instrument used to measure ROM was not a goniometer. Despite the difference in ROM for some of the tasks favouring the Early group, the narrow margin for other tasks may explain why the OSS score was similar. Patients may not see a substantial increase in range of motion being the same as an indicator of a better outcome; as long as they reach a functional range that permits the return to some of their basic activities. Therefore, even though the Early group had greater improvements in ROM, both groups were functionally equivalent and consequently, one rehabilitation regime does not seem to be superior to the other on meeting patients’ expectations. Moreover, at this stage, patients may consider that a better improvement in pain intensity and quality of sleep is more relevant than having a greater ROM of their shoulders [33, 34].
In our study, muscle recruitment was assessed with EMG. Overall, the integral of the 5 muscles showed some changes between groups but with high variability, which indicates that the amount of work done by each muscle was similar between groups and time points. However, as mentioned previously, the Conservative group generally showed a reduction in ROM over the tasks. Therefore, although groups may have equivalent muscle recruitment, Early rehabilitation may facilitate an earlier return to activities. The similar amount of work done and EMG amplitude, but with better ROM for the Early group, indicates that their shoulder muscles may be more efficient than the Conservative group, i.e. patients in the Early group needed equivalent muscle activity to perform greater joint excursions [35]. This rationale is supported by other studies showing that the amount of power generated by muscles is not associated with an increase in EMG activity [36].
We found that the Early group had a higher number of re-tear events. However, three patients from the Conservative group did not attend their scan appointment compared to one from the Early group, thus, additional events in the Conservative group may have been missed. Moreover, the Early group had a greater number of smokers; smoking has been linked to worse outcomes and is considered a risk factor for rotator cuff tears [37]. Although a higher number of re-tear events was found for the Early group only two patients were symptomatic. This finding corroborates with other studies reporting that even if a re-tear occurs patients may present significant improvement of their pain and strength [38–40].
Limitations
The sample size planned was not achieved and considerable lost to follow-up was observed, therefore, descriptive statistics was preferred as the study would have limited power to determine whether possible non-significant statistical differences between groups were not truly different [41]. These limitations may limit the applicability of our findings, it is possible that due to missing values the treatment effects have been underestimated or overestimated [42, 43].
Conclusion
This study suggests that early rehabilitation is not superior to conservative rehabilitation in improving function and quality of life. There is some indication that an early regime may be beneficial to improve ROM and muscle efficiency; however, the number of re-tears, although mostly asymptomatic (no pain or difficulties with daily activities), were higher for this group.