
Abstract
BACKGROUND AND OBJECTIVES:
Airway clearance techniques (ACTs) are used by physiotherapists with the purpose of clearing sputum from bronchial airways. They are commonly prescribed for patients experiencing acute exacerbations of chronic obstructive pulmonary disease (AECOPD), however large variability in practice is commonly observed. This study aimed to explore current physiotherapy practice regarding ACTs for people with AECOPD in the Republic of Ireland.
METHOD:
An online survey was distributed to physiotherapy clinicians via direct email and the Irish Society of Chartered Physiotherapists. Main survey themes, identified from previous studies using the same survey tool, included current practice in relation to use of ACTs, perception of their effectiveness, clinical reasoning and awareness of the literature and guidelines. For the purpose of this study, ACTs were defined as techniques used by a physiotherapist for the purpose of clearing sputum from patients’ airways.
RESULTS:
202 surveys were distributed and seventy responses (35%) were received. The majority of respondents (n = 56, 80%) reported prescribing ACTs for more than 60% of patients with AECOPD, the most common techniques being physical activity (n = 65, 93%) and active cycle of breathing techniques (n = 53, 90%). Sputum management (n = 66, 94%) was the most commonly reported indicator for use of ACTs. The majority of physiotherapists (n = 42, 60%) reported being unsure of the literature regarding ACTs in AECOPD.
CONCLUSION:
The response rate to this survey was low, however results show that physiotherapists in the Republic of Ireland regularly prescribe ACTs for patients with AECOPD. Physical activity and active cycle of breathing techniques were the most commonly used ACTs and perceived to be the most effective techniques in AECOPD, with sputum management the most commonly reported indicator for use. Further research is required to explore not only physiotherapists clinical reasoning in relation to the use of ACTs for AECOPD and the perceptions of their effectiveness, but also the lack of awareness of the literature and guidelines.
Keywords
Introduction and background
Chronic obstructive pulmonary disease (COPD) is a progressive, irreversible lung disease typically caused by exposure of the airways to noxious substances [1]. It is defined physiologically by a persistent obstructive airflow defect, and characterised by symptoms of breathlessness, cough and sputum production [1]. COPD is the third leading cause of death in the world and accounts for 6% of deaths internationally [2]. It is estimated that almost 500,000 people (∼10% of the population) in the Republic of Ireland could have COPD [3]. People with COPD may experience flare-ups of their disease called acute exacerbations of COPD (AECOPD). AECOPDs are complex events commonly associated with inflammation of the airways and excess mucus production [2] and characterised by acute deterioration of symptoms such as breathlessness, cough and/or sputum production. AECOPDs are important events due to their negative impact on health status, healthcare utilization and disease progression. [1, 2].
Airway clearance techniques (ACTs) are a treatment option that target problems associated with excessive sputum production or difficulty clearing sputum. ACTs are techniques that aim to clear bronchial secretions via use of gravity, breath holding, forced expiratory techniques (an expiratory breath of varying volume and flow rate used to aid bronchial expectoration [30]) and/or positioning, leveraging on key principles of alveolar interdependence, collateral ventilation and two-phase gas flow [8, 29]. In healthy lungs, bronchial secretions are cleared by cilia, in the lining of the airways, via cephalad transportation [29]. In COPD, however, ciliary dysfunction occurs, resulting in retention of excess sputum and airways secretions - a component of the pathological disease process linked to increased frequency of exacerbations and hospitalisations [5, 29].
The principle of two-phase gas-liquid flow describes the process whereby air flows over the surface of sputum in the airways on inspiration and then exerts an expiratory shear force behind the sputum during expiration to facilitate expectoration [32]. Pressure within the bronchial airways can increase or decrease depending on lung volumes, air flow rate and airways resistance, while pressure on bronchial airways can be influenced by varying the force of exhalation [29]. It is theorized that ACTs can maximize sputum shear forces in the airways at the point at which airway pressure equals intrapleural pressure- called the equal pressure point [31]. In the literature, ACTs have been reported to influence the movement of the equal pressure point further towards the alveoli, improve airflow to collateral channels and influence alveolar interdependence which may be associated with clearance of sputum from peripheral to proximal regions of the lung, thus facilitating sputum expectoration [9, 29].
Evidence of clinical effectiveness regarding ACTs for people with AECOPD has existed for some time now. Despite some ACTs such as positive expiratory pressure devices and active cycle of breathing techniques being recommended for patients with excessive sputum during an AECOPD [4], conclusions regarding ACT effectiveness are highly variable [11]. This is likely due to considerable heterogeneity of review methodologies and highly variable quality of individual clinical trials on people with COPD [7, 13]. A small number of studies have explored physiotherapy practice of ACT prescription for the management of patients with AECOPD [15–19], demonstrating large variability in practice. For example, the most prescribed techniques for AECOPD in Australia were active cycle of breathing techniques (ACBT) and physical exercise [18], while Swedish physiotherapists reported using positive expiratory pressure (PEP) masks most [19]. No data exists relating to the Republic of Ireland.
In the Republic of Ireland, use of ACTs by physiotherapists for COPD is outlined by the Health Services Executive (HSE) “End to End COPD Model of Care” clinical guidelines, which are based on the Global Initiative for Obstructive Lung Disease (GOLD) Guidelines [2, 3]. The HSE recommends use of ACTs by physiotherapists treating patients with COPD in the integrated care, acute hospital and COPD outreach settings but does not specify which ACTs are the most effective nor how or when to prescribe them. The extent to which physiotherapists employ ACTs in their management of AECOPD in the Republic of Ireland has not been examined, and thus no comparisons can be made with international practice. In addition, examining local practice may help to identify trends in the use of ACTs in the Republic of Ireland, and inform future service improvements in this important area of clinical practice.
The primary aim of the study was to determine current practice of physiotherapists with respect to ACTs and AECOPD in the Republic of Ireland. Secondary aims were to i) explore perceptions regarding the importance of ACTs for clinical practice and effectiveness of ACTs to clear sputum; ii) identify factors influencing the prescription of ACTs; and iii) examine physiotherapists’ awareness of evidence regarding ACTs in their management of patients with AECOPD.
Methods
Ethical approval for this study was granted by Ulster University Ethics Board in December 2019 #RG3_2019-12-3.4.
Procedures
A cross-sectional survey of physiotherapists treating patients with AECOPD in the Republic of Ireland was implemented during January and February of 2020. The survey was conducted electronically via Survey Monkey. Physiotherapists working in the Republic of Ireland in the public or private health system were eligible for inclusion if they were registered with (or pending registration with) the national professional body CORU and had treated patients with AECOPD within the last 10 years. For the purpose of this study an AECOPD was defined as an acute deterioration of a patients’ respiratory symptoms requiring additional therapy [2], either in the community or following hospital admission. ACTs were defined as techniques used by a physiotherapist for the purpose of clearing sputum from patients’ airways [18].
The survey comprised multiple-choice questions and Likert scales, based upon a previously used instrument where the survey was first evaluated for face validity via pilot testing on a representative sample [18]. The authors of the survey used Likert scales to ensure brevity of the survey, for example “How easy is it for patients with AECOPD to master the following techniques?” and multiple-choice questions were also used to allow for answers pertaining to clinical reasoning, for example “What do you consider to be important indications for ACTs in patients with AECOPD?”. With alteration of one question and addition of one other, as per original authors recommendations (Appendix 1), the amended survey was further reviewed by a respiratory clinical nurse specialist, a senior physiotherapist and a consultant respiratory physician in the Republic of Ireland to verify the questions were appropriate for target respondents and targeted to the specific aims of the present study. Permission was granted to use the survey by the original authors [18] and was distributed via email link to members of the Chartered Physiotherapists in Respiratory Care group (90 physiotherapists) and Chartered Physiotherapists Manager group (88 physiotherapy managers) of the Irish Society of Chartered Physiotherapists (professional body of the Republic of Ireland). The survey was also emailed to physiotherapists throughout the Republic of Ireland working in COPD outreach and respiratory integrated care services (approximately 24 physiotherapists), with all recipients encouraged to share the survey with colleagues experienced in respiratory care. In total, the approximate number of survey distributions was 202. To facilitate survey engagement, potential participants were emailed one week prior to initial survey distribution and reminders sent one, two and three weeks afterwards. Survey responses were also anonymised and data pertaining to work location and education history were not recorded. Sample size calculation was not performed for this study due its cross-sectional nature of distribution (i.e. targeting all participants in the Republic of Ireland who treat patients with AECOPD).
Data analysis
Data were presented descriptively using frequencies and percentages. Some data were pooled into fewer categories in order to explore relationships between variables. For example, work experience in the cardiorespiratory field was subdivided as ≤5 vs 5 or more years, and similar approaches used for perceived effectiveness and awareness of the evidence regarding ACTs. This allowed for comparisons to be made between questions via Chi square tests. Statistical significance was set at p≤0.05. Analyses were conducted using IBM SPSS statistical package version 26 and results presented as column graphs via Microsoft Excel.
Results
Participants
Responses were received from 70/202 (35% response rate) physiotherapists who self-reported meeting study inclusion criteria. All returned surveys (n = 70) were fully completed. The majority of respondents (n = 59, 84%) reported greater than 5 years physiotherapy experience (0–5 years, n = 11; 5–10 years, n = 16; 10–15 years, n = 19; 15–20 years, n = 11; 20+ years, n = 13), with 63% (n = 44) working specifically in cardio-respiratory physiotherapy for at least 10 years. Survey responses were anonymised, and data pertaining to workplace (public, private, community or hospital based) were not collected.
Current practice
The majority of respondents (n = 56, 80%) reported prescribing ACTs for more than 60% of patients with AECOPD with only 7% (n = 5) doing so rarely or never. The frequency of prescription of ACTs for patients with AECOPD did not differ between physiotherapists with less or more than 5 years cardiorespiratory experience (p = 0.65). The majority of respondents (n = 65, 92%) spent between 5–20 minutes on ACT treatment, with 3% (n = 2) spending 0–5 minutes, 40% (n = 28) spending 5–10 minutes, 31% (n = 22) spending 10–15 minutes and 21% (n = 15) spending 15–20 minutes. 96% (n = 69) of respondents perceived ACTs to be important (very important, fairly important or moderately important). The most commonly prescribed individual ACTs (combined “very often/always” or “often”) were physical activity 93% (n = 65), ACBT 90% (n = 63) and deep breathing exercises 90% (n = 63). A detailed overview of all ACTs is presented in Fig. 1.
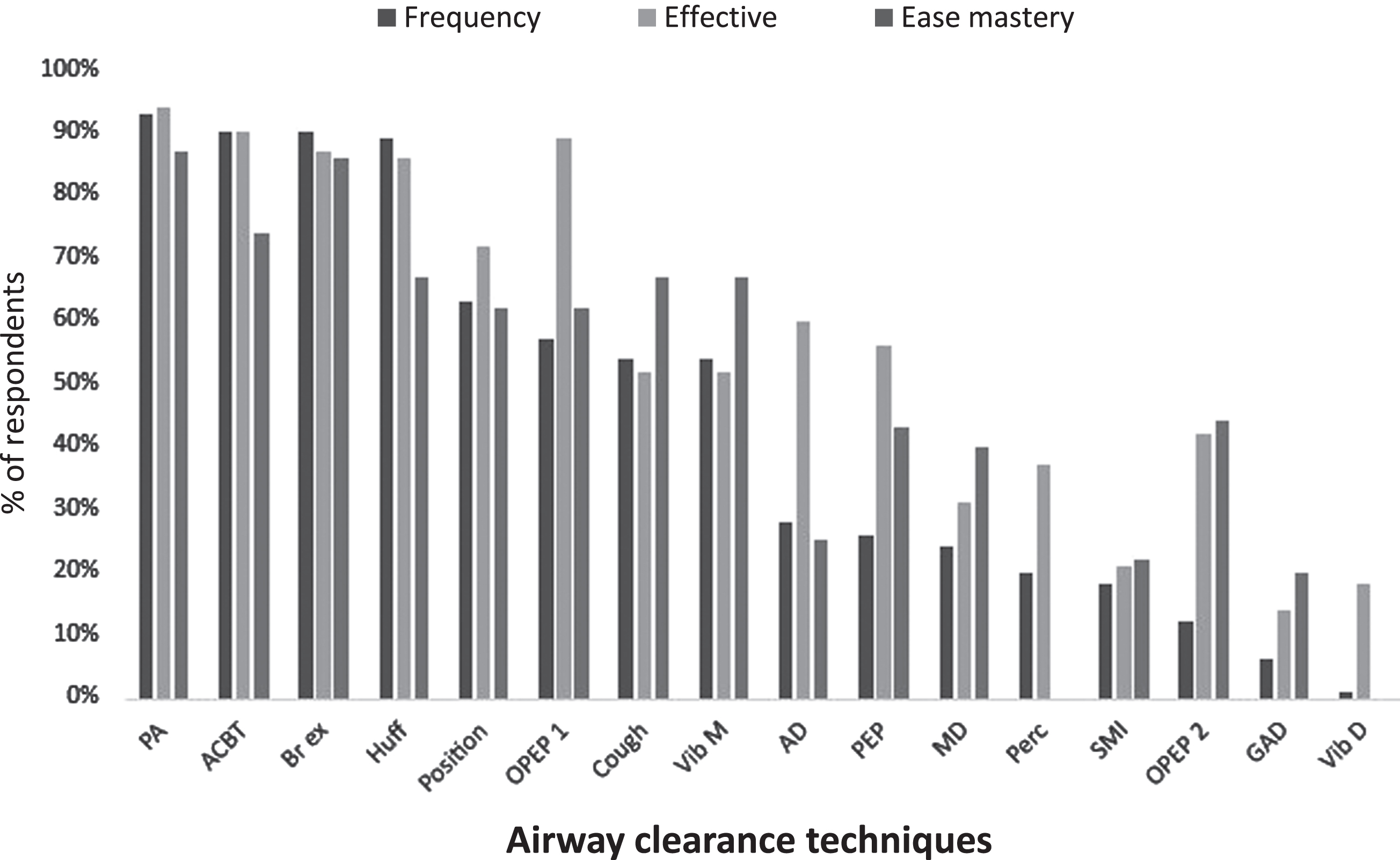
Frequency of use, perceived effectiveness and perceived ease of patients’ mastery of airway clearance techniques by physiotherapists in the Republic of Ireland. For each of frequency, effectiveness and mastery, Likert options were combined as follows: Frequency; very often or always/often. Effectiveness; very effective/ effective. Mastery; very easy/easy. PA = physical activity; ACBT = active cycle of breathing techniques; Br ex = breathing exercise; Huff = directed huffing; Position = positioning; OPEP 1 = oscillating PEP device (Flutter, Acapella, Cornet); Cough = coughing;VibM = manual vibration;AD = autogenic drainage; PEP = positive expiratory pressure; MD = manual drainage; Perc = percussions; SMI = sustained maximal inspiration; OPEP 2 = oscillating PEP (bubble/bottle); GAD = gravity assisted drainage; Vib D = mechanical vibration via device.
Physiotherapists perceived the most effective techniques for clearing sputum (very effective/ effective) to be physical activity (n = 66, 94%), followed by ACBT (n = 63, 90%), oscillating PEP (n = 62, 89%) and directed huffing (n = 60, 86%). With respect to patient mastery of ACTs, respondents perceived physical activity (n = 61, 87%), deep breathing (n = 61, 86%) and ACBT (n = 52, 74%) to be easiest (very easy/easy). There was no statistically significant relationship between perceived importance of ACTs and years of experience working in cardiorespiratory physiotherapy (p = 0.439). Frequency of use, perceived effectiveness and perceived ease of patients’ mastery of airway clearance techniques is summarised in Fig. 1.
Factors influencing prescription
The most frequently identified indicators for prescribing ACTs were “difficulty managing secretions” (n = 67, 96%) and “recent change in sputum characteristics” (n = 63, 90%) (Fig. 2). The vast majority of respondents reported their primary aim of prescribing ACTs was “to clear sputum” (n = 68, 97%), “to improve oxygenation” (n = 59, 84%), “enhance recovery from AECOPD” (n = 57, 81%) and “improve quality of life” (n = 53, 76%). Physiotherapists’ reasoning for choosing between different ACTs was made on the basis of those deemed “easiest to master” (n = 51, 73%), followed by “access to resources/equipment” (n = 45, 64%), “degree of dyspnoea” (n = 42, 60%) and “patient preference” (41/70, 59%).

Indicators for use of ACTs by physiotherapists in the Republic of Ireland. Difficulty = difficulty managing secretions; Change = a recent change in sputum characteristics; IECOPD = clinical signs suggestive of infectious exacerbation; Education = patient in need of education; Secretions- presence of secretions; Productive = anyone with productive cough; Usual ACTs = patients who usually perform ACTs as part of management of their condition; >30 mls/day = patients who produce >30 mls sputum/day; Other.
While 40% (n = 28) of respondents believed there was evidence supporting the use of ACTs during AECOPD, 40% (n = 28) believed the evidence was “conflicting, inconclusive or non-existent to support or refute use of ACTs”. Twelve respondents (20%) declared feeling “unsure what the current evidence is”. Of the 80% of respondents who felt they were familiar with the literature, no differences were evident in terms of the extent of their experience between those working in cardiorespiratory more or less than 5 years and their awareness of the evidence for the effectiveness for ACTs with AECOPD (p = 0.534). There was also no significant relationship between respondents who felt ACTs were important in the management of patients with AECOPD and perception of the strength of evidence to support the practice of ACTs for patients with AECOPD (p = 0.377). Fifty (71%) respondents indicated they were not familiar with Irish guidelines for the use of ACTs for patients with AECOPD.
Discussion
This was the first study of its kind to examine current practice of physiotherapists in Republic of Ireland with respect to ACTs for patients with AECOPD. While caution is advised in interpreting findings from this small sample size, results suggest practice patterns appear comparable to those reported in other countries. ACTs were commonly used by physiotherapists in the management of patients with AECOPD and physical activity was perceived to be the most effective ACT. There appears to be a high degree of uncertainty regarding the evidence to support this practice and poor awareness of existing national guidelines to support clinicians regarding this area of practice, as identified in other similar work [19]. It has been useful to identify these trends locally and this information should inform future research in relation to this important population of patients.
Treatment session duration (5–20 minutes) among physiotherapists from Republic of Ireland appears consistent with previous reports [18, 19], however the high rate of ACT prescription (93%) was greater than data from Australia (65%) [18] and Sweden (75%) [19]. This is despite similarities in the reported prevalence of COPD between countries. While the relationship between rate of prescription of ACTs and respondents perceived importance of them was not statistically significant in this study, an interesting observation between studies using this survey instrument has been the relationship between perceived importance of ACTs and years working in cardiorespiratory physiotherapy. As in this study, the Swedish study [19] did not report any significant differences in the frequency of prescription of ACTs and respondents working in cardiorespiratory more or less than 5 years. In the study conducted by Osadnik et al. [18], however, respondents with less than 5 years’ experience in cardiorespiratory reported prescribing ACTs more often than those with greater than 5 years’ experience (p = 0.017). This discrepancy may be reflected in undergraduate and postgraduate curricula, where more emphasis may be placed on teaching ACTs at undergraduate level in Australia. Further research would be warranted and may reveal some disparity in the delivery of such educational content internationally.
Just under half of respondents believed there was evidence to support the use of ACTs during AECOPD. Yet, interestingly, a minority of respondents (36%) reported they consider the evidence when choosing a suitable ACT. This finding has been previously observed [18, 19] and may reflect a degree of confusion interpreting the key messages from existing literature. It was concerning to observe the majority of respondents (71%) were unaware of guidelines published by the Health Services Executive in the Republic of Ireland [3] in relation to the management of COPD, although these were only published one month prior to the survey and may not have been widely available. Further research is required to explore the factors contributing to this finding in order to identify perceived barriers and facilitators to clinicians timely access to relevant information.
While the use of physical activity as an ACT has not yet been directly examined in people with AECOPD, efficacy data is reported in people with stable cystic fibrosis. A single exercise session in a small adult CF sample (n = 14), FEV1 range 19–108%, was found to improve ease of sputum clearance [24] and a subsequent study by the same group [22] (n = 24) found PEP and treadmill exercise augmented sputum clearance equally effectively. The mechanism proposed to explain these findings suggests PA increases peak expiratory flow and water content of viscous secretions, thus facilitating clearance. Differences between populations and pathophysiology of acute exacerbations, however, render it difficult to determine whether such findings would translate to people with AECOPD. Further enquiry into this area of practice would be of benefit to clinicians and patients, particularly in light of a recent study [26] that showed Australian physiotherapists frequently prescribe physical activity for patients with AECOPD, often in conjunction with huffing and coughing.
While a recent Cochrane systematic review reported physical activity to be no more effective as an airway clearance technique for people with cystic fibrosis than other ACTs, it must be acknowledged that there is a paucity of high quality robust randomized controlled trials available for both this and the COPD population [33].
A more recent randomized cross-over trial measured the effect of treadmill exercise on mucus clearance in 14 adults with mild to severe cystic fibrosis, when compared to use of positive expiratory pressure (PEP) therapy and resting breathing (control) [34]. Significantly more sputum was cleared from the central lung region immediately after the exercise intervention when compared to the control (2.6%, p < 0.001, CI 95%) but less sputum was cleared after exercise when compared to PEP therapy for the same region (–12.9, p < 0.001, CI 95%). The use of PEP therapy in this small study included forced expiratory techniques and coughing, which have been reported to positively influence bronchial airway clearance [8, 30]. Future studies should investigate the effects of exercise to include forced expiratory techniques and coughing in the COPD population in order to explore further the association between physical activity and its relationship to airway clearance.
Furthermore, as ‘ease of mastery’ was cited as an important factor determining choice of specific ACT, it would be useful to investigate the patient experience of performing ACTs, including physical activity, during AECOPD to reveal insights to further guide physiotherapy prescription.
Limitations
Findings from this survey need to be considered in light of some limitations. The convenience sample was not based on a pre-determined sample size calculation, meaning we were likely underpowered to detect some relationships via inferential statistics. Although 202 surveys were distributed, it is also difficult to ascertain the precise number of people to whom this survey was distributed due to ‘snowballing’ recruitment methods and possible overlap of individuals across multiple dissemination sources and workplace settings. The low estimated response rate may mean insights lack some generalisability across broader Irish and international physiotherapy practice and selection bias may also have occurred due to the sampling methods of the study. It would be interesting to explore whether a blended method of paper-based and online surveys, or a focus group study, might have optimised responses in order to collect the depth and breadth of information required to meet the aims of the study. The term physical activity was open to participants interpretation as a clear definition was not provided. As we did not record study participants characteristics we were unable to explore the potential for differences in ACT practice between physiotherapists working in outreach / integrated care sites and those based in hospitals, differences in relation to age, gender or education level. This would be useful to ascertain in future research. Finally, self-reported questionnaires are known to be susceptible to recall bias, however the nature of questions included in the instrument aimed to minimise this effect.
Conclusion
Physiotherapists in the Republic of Ireland frequently prescribe ACTs for the management of patients with AECOPD and perceive physical activity to be the most effective individual technique despite a lack of evidence to support its rationale for this purpose. There was a low response rate to this study, which limits the generalisability of the findings and their clinical implications, however results may be useful in directing future research. It is clear that awareness of national guidelines for the management of COPD was very low and further investigation is warranted to better understand the reasons for this. Future research should aim to explore the use of physical activity as an airway clearance strategy in people with COPD, as this study, and others have reported that physiotherapists consider physical activity an effective and popular choice of ACT for AECOPD. This study has also identified a lack of awareness of the literature and guidelines to support the use of ACTs in AECOPD- this should be an area of priority for future research and educational strategies. It is clear from this study that variations in the use of ACTs for AECOPD exist, and in the absence of clear evidence and guidelines for their use, physiotherapists must make judicious decisions regarding the use of airway clearance techniques to optimize the individualized management of patients with AECOPD.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflict of interest to report.