
Abstract
OBJECTIVES:
To assess the feasibility of a 30-minute education session for patients with patellofemoral pain on levels of catastrophizing and kinesiophobia.
DESIGN:
Randomised feasibility study
SETTING:
Three sites within a single NHS Organisation in England.
PARTICIPANTS:
Thirty-one adult patients were screened for inclusion, resulting in twenty-four who had a clinical diagnosis of patellofemoral pain being randomised equally to either the intervention or control group.
INTERVENTION:
Participants were randomised to either control or intervention conditions; both received standardized physiotherapy while the intervention/experimental group received a 30-minute educational session addressing causes of pain, beliefs about noise that comes from the joint, the impact of the pain on activity, the influence of other family members’ experience and beliefs about knee pain. Intervention participants were also given an education leaflet: ‘Managing My Patellofemoral Pain’.
MAIN OUTCOMES:
recruitment, retention, intervention fidelity.
Patient reported outcome measures (PROMs): Knee injury and Osteoarthritis Outcome Score for patellofemoral pain and osteoarthritis (KOOS-PF), Pain Catastrophizing Scale (PCS) and Tampa Scale for Kinesiophobia (TSK).
RESULTS:
The study was successful in recruiting and retaining participants and was delivered as intended. In addition, sufficient clinical data were generated to calculate the required sample size for a future study of efficacy
CONCLUSIONS:
This study which featured a 30-minute education session targeting levels of catastrophizing and kinesiophobia is feasible and identified that the TSK may be the most appropriate PROMs for a future study of efficacy of this intervention. Allowing for a drop out of 20% as identified in similar studies, 86 participants (per arm) in a two-arm study would be required for a traditional randomised controlled trial design.
Introduction
Patellofemoral pain (PFP) is characterised by peri or retropatellar knee pain, which is reproduced upon activities of daily-living when there is load or stress on the patellofemoral joint such as when climbing stairs, squatting and sitting [1]. The impact of PFP may extend to social engagements and participation in physical activities including sports and occupational tasks [2].
One in five of the general population will have experienced PFP within the last year [3] and there is a poor prognosis with 91% reporting pain and dysfunction four years post-diagnosis [4]. Symptoms may persist for decades after their first onset; with estimates ranging from 16 to 20 years [4–7], therefore it is appropriate to consider PFP can become a chronic musculoskeletal condition in some instances. Forty to 57% of patients will experience unfavourable long-term outcomes despite receiving evidence-based treatments [2] including strengthening exercises, often prescribed to address biomechanical faults during activities [8, 9]. A significant number of patients who have PFP have been found to have lower levels of strength in their quadriceps and gluteal muscles than individuals without PFP [10]. However, research by Selfe et al. (2016) [11] identified a subgroup of PFP patients, predominantly males with higher levels of hip abductor and quadriceps strength who were classed as ‘strong’. This might help to explain why some patients who receive evidence-based strengthening exercises continue to have poor outcomes. Similar to other chronic musculoskeletal conditions, chronic PFP is associated with high pain intensity, low quality-of-life and increased risk of ceasing participation in sports [12]. The psychological impact of PFP [13] offers a challenge to the traditional biomedical approach to the management of PFP. The most recent Consensus Statement from the International Patellofemoral Pain Research Retreat [10] recommends a greater emphasis be placed on addressing psychosocial factors and pain sensitization.
Robertson et al. (2017) [14] explored the beliefs of patients with PFP about crepitus and the impact of this on their behaviour. The key emergent themes influencing behaviour were: patients’ beliefs that crepitus was damaging, the influence of others and avoiding the noise. Patients, with PFP have also been found to have higher levels of catastrophizing, kinesiophobia [15] and mental distress [16] than people without PFP. Smith et al. (2017) [17] demonstrated, the importance of understanding the significant negative effects of living with PFP on peoples lifestyles and how it impacted on their well-being. The study highlighted the possibility that improved outcomes could potentially be achieved by supporting people living with PFP to overcome psychological barriers.
Biopsychosocial interventions targeting catastrophizing and kinesiophobia are yet to be fully explored in patients with PFP. Research from other chronic pain conditions suggest that focusing on reducing kinesiophobia might be promising as it is moderately associated with lower pain and higher function following appropriate education [15, 18]. Similar to the traditional clinical management of PFP, the usual patient education approach for PFP is also through a biomedical lens where anatomy and biomechanics are the main foci [18]. However, pain is complex; it is a sensory and emotional experience [18, 19] which can have a longer term impact on behaviour [19]. Therefore, the intervention in this feasibility study adopted a biopsychosocial approach focussing on catastrophizing and kinesiophobia, whereby the participants own lived experience and beliefs were discussed in reference to how they manage and respond to their pain.
Methods
The primary aim of this study was to determine the feasibility of a RCT comparing standardised physiotherapy with an education intervention addressing patients’ catastrophizing and kinesiophobia. Both groups received the same standardized physiotherapy while the experimental group also received a 30-minute educational session addressing kinesiophobia and catastrophizing. The specific uncertainties for this study were recruitment, retention, intervention fidelity [20], which meant that a feasibility study in the first instance was appropriate. Secondary objectives were to generate data that would inform a sample size calculation for a future study by collecting data from three different patient reported outcome measures (PROMs) [21].
Study design and participants
In this single site feasibility study, twenty-four patients were recruited via an NHS teaching hospital. The study was approved by the North West –Liverpool Central Research Ethics Committee and HRA (18/NW/0725) and all participants provided written informed consent. The study was registered with Clinicaltrials.gov NCT03784339.
Patients who had been clinically diagnosed in a Musculoskeletal Clinical Assessment Service (MCAS) with PFP at 3 sites within an NHS teaching hospital trust were approached to take part in the study. Recruitment began in April 2019, patients were provided with information about the study by a participant identification physiotherapist. The research physiotherapist contacted patients interested in taking part to discuss and made arrangements to obtain informed consent as appropriate. Once enrolled onto to the study, randomisation software (Research randomizer: randomizer.org) was used to allocate participants to either intervention or control groups.
Eligibility was assessed by the research physiotherapist prior to taking written informed consent.
Inclusion criteria
Adults aged 18–40 years Able to understand written and spoken English. Clinical diagnosis of PFP [2] Able to attend for up-to 12 weeks of physiotherapy
Exclusion criteria
Patients who presented with referred pain from the spine or hip, or who had tibiofemoral pathology of any nature on the ipsilateral side. A diagnosis of PFJ osteoarthritis as confirmed by x-ray or MRI. Previous surgery to the symptomatic knee.
Outcome measures
The PROMs used in this study were Knee injury and Osteoarthritis Outcome Score –Patellofemoral subscale (KOOS-PF) [22, 23], Pain Catastrophising Scale (PCS) [24] and Tampa Scale of Kinesiophobia (TSK) [25].
The KOOS-PF includes five subscales; Pain, other Symptoms, Function in daily living (ADL), Function in sport and recreation (Sport/Rec) and knee related Quality-of-life (QOL). It also includes the 11-item patellofemoral pain and osteoarthritis subscale, developed for use with PFP patients. Items are scored 0–4; the sub-scales are calculated independently, and transformed to give a score from 0–100 with 0 indicating worse scores. The reported minimum clinically important change (MCIC) is 16 points [22].
The PCS is a 13-item questionnaire describing thoughts and feelings that individuals experience when they have pain. Participants reflect on their pain experience and indicate one of the 13 thoughts or feelings perceived at the time of pain. The scale ranges from 0–52, where 52 represents greatest catastrophic pain [24]; scores greater than 24 being associated with higher pain ratings [26]. The reported MCIC is 9 points for low back pain [27].
The TSK is a 17 item questionnaire used to quantify fear of movement and re-injury due to movement and physical activity on a scale of 0–68, where 68 indicates greatest fear of re-injury due to movement [25, 28]. A score of thirty seven has been suggested as the boundary for high and low fear [29]. The reported MCIC is 4 points [30].
Sample size
The sample size was informed by previous research [17, 32], suggesting a total of n = 24 participants (n = 12 per group) would be required to answer the feasibility objectives. Therefore in this 2 arm randomised feasibility study each group comprised 12 participants.
Baseline measures
Participants were asked to self-report their baseline characteristics including age, sex, and duration of symptoms, which were collected alongside baseline PROMs: KOOS-PF, TSK and PCS. These questionnaires were repeated after 12 weeks.
Study design
Participants were randomised to either the intervention (n = 12) or the control group (n = 12). All participants in both groups received their treatment directly from the research physiotherapist only.
Control conditions
Participants in the control group underwent standardised treatment, comprising an explanation of the diagnosis of PFP with a management plan and an individualised home exercise programme.
Experimental conditions
Participants in the experimental group (the intervention group) received the same intervention as participants in the control group plus an individual education session. The individual education session, lasted for 30 minutes and allowed a two-way face-face conversation to take place between the research physiotherapist and the participant. Topics covered in the education session were The causes of pain Beliefs about pain Beliefs about noises from the joint The impact of the pain on activity The influence of other family members’ experience and beliefs about knee pain
A patient education leaflet was also provided [33] as part of the intervention. Following the intervention session, participants received the same standardised physiotherapy as control participants. At 12 weeks, participants from both groups were asked to repeat the PROMs.
Recruitment
The study objectives were to assess recruitment, retention and intervention fidelity. Recruitment was assessed by keeping a log of all patients identified as having PFP by the clinicians in MCAS and the number of those who met the inclusion criteria by the research physiotherapist against the number of participants recruited to the study.
Retention
To optimise retention participants who were lost to follow up were telephoned and PROMs sent in the post with paid return envelopes enclosed. A log was kept of those who responded to telephone and PROMs.
Intervention fidelity
Self-assessment was used by the research physiotherapist to assess intervention fidelity [34]. The study protocol was reviewed to check if the pre-defined topics were discussed and if intervention participants received the education leaflet.
Results
Recruitment
As illustrated by the CONSORT diagram, thirty-one patients were screened; seven of whom were ineligible (n = 1 did not speak English, n = 2 had undergone previous knee surgery, n = 4 declined to participate). The remaining twenty-four were recruited and consented from April to November 2019 at a rate of three per month.
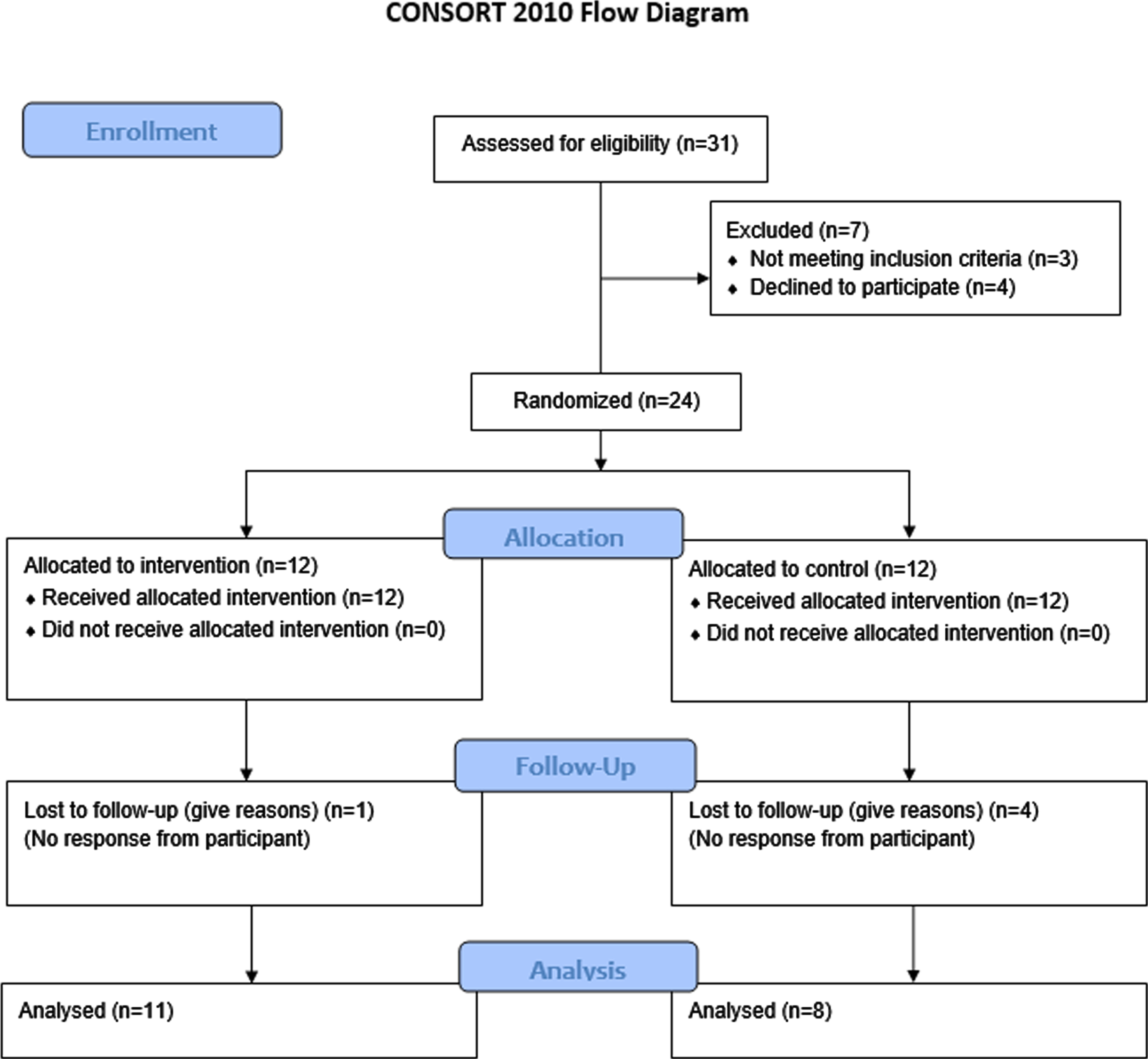
Consort flow diagram.
Baseline characteristics: means (standard deviations) indicated
Mean age was higher in the intervention group and both groups had more females. Mean duration of symptoms was longer in the intervention group. The group also had higher mean scores on PCS and TSK. As this was a randomised design, baseline characteristics were not analysed for significant differences. This was because we already know that these would have arisen by chance. Furthermore this practice of analysing for baseline differences is actively discouraged in randomised designs [35].
The average (mode) number of treatment sessions attended was three and four in the intervention and control group respectively. There were no specific or fixed number of treatment sessions predefined for both intervention and control group participants.
Nineteen out of the 24 participants were retained in the study. One (female) was lost to follow-up in the intervention group, four (3 female and 1 male) were lost to follow-up in the control group.
Intervention fidelity
This self-audit by the research physiotherapist identified that the intervention was delivered as planned, all pre-determined topics were covered in the intervention session (experimental conditions), and thus fidelity was 100% with every participant.
Outcome measures
All participants improved their scores on each of the three PROMs; KOOS-PF, TSK and PCS, except for one whose KOOS-PF score deteriorated. Mean pre-intervention, post-intervention and change scores are presented for each outcome measure (Table 2).
Pre, post and change scores for outcome measures: mean (standard deviation) and minimally clinically important change (MCIC) score
Pre, post and change scores for outcome measures: mean (standard deviation) and minimally clinically important change (MCIC) score
Pre and post-scores for each of the questionnaires for the intervention and control groups are shown in box plots in Figs. 2–4. Figure 2 shows that both groups improved their KOOS-PF scores, with the range being greater post-intervention in the intervention group.
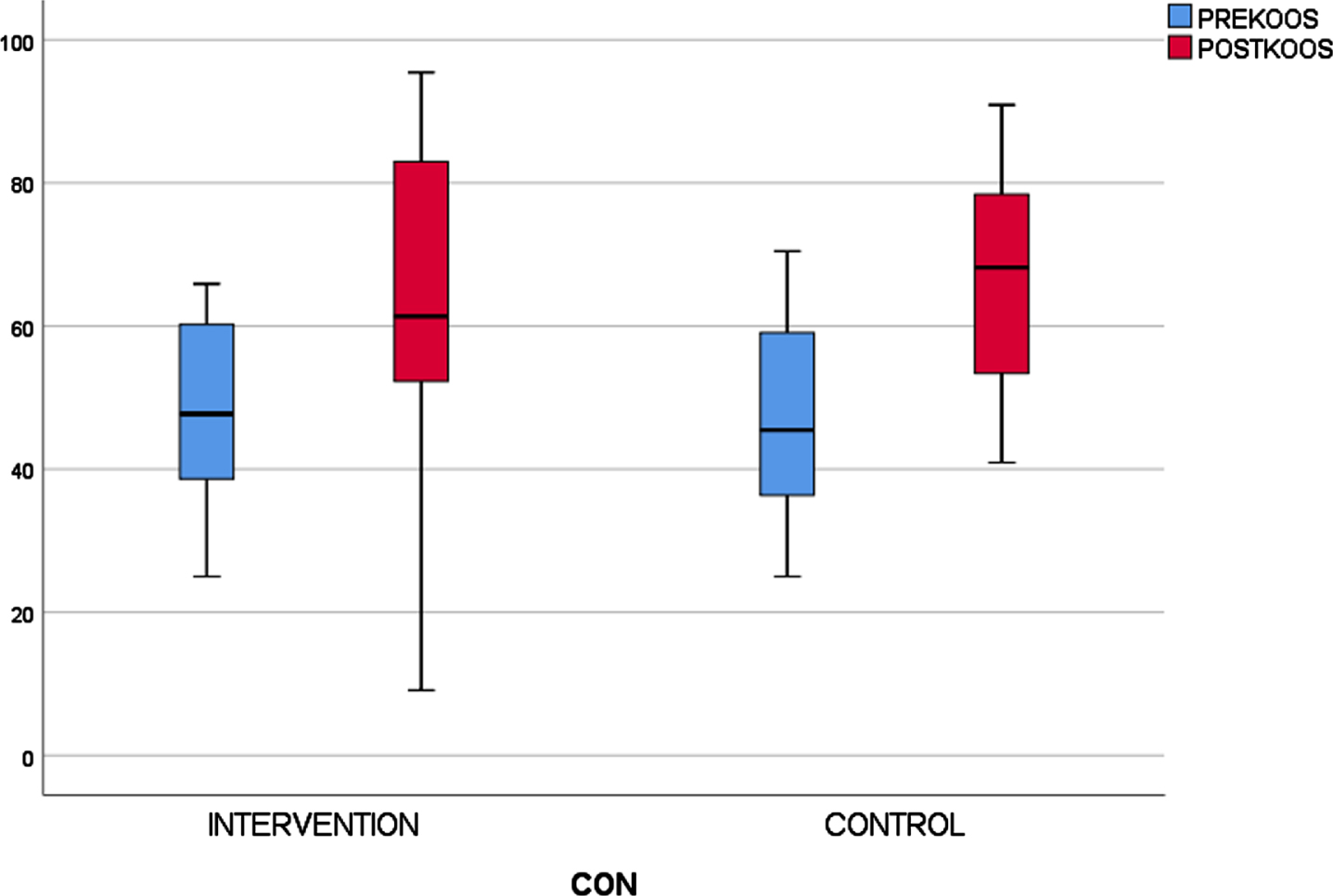
Pre and post-intervention KOOS scores for each group.
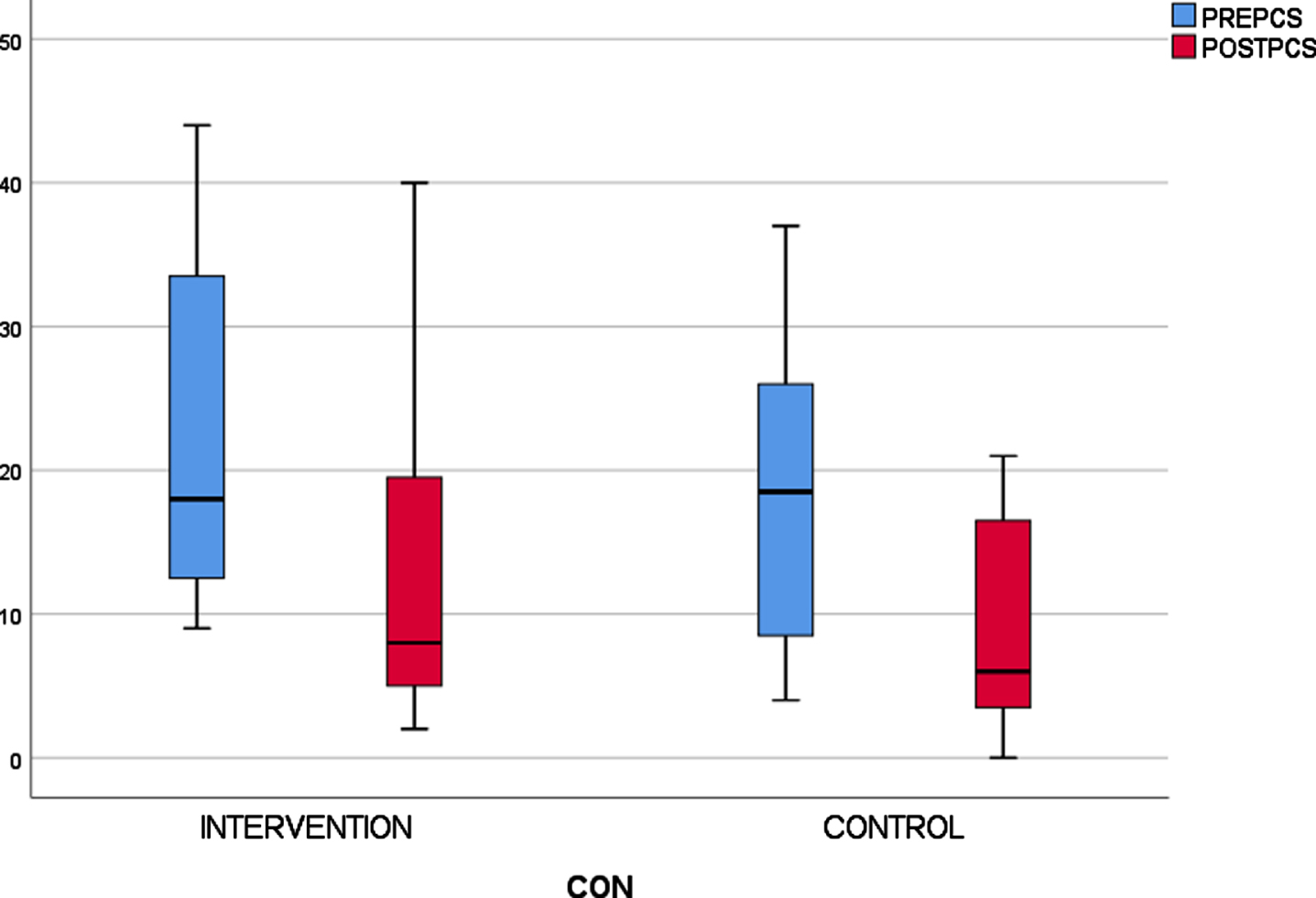
Pre and post-intervention PCS scores for each group.
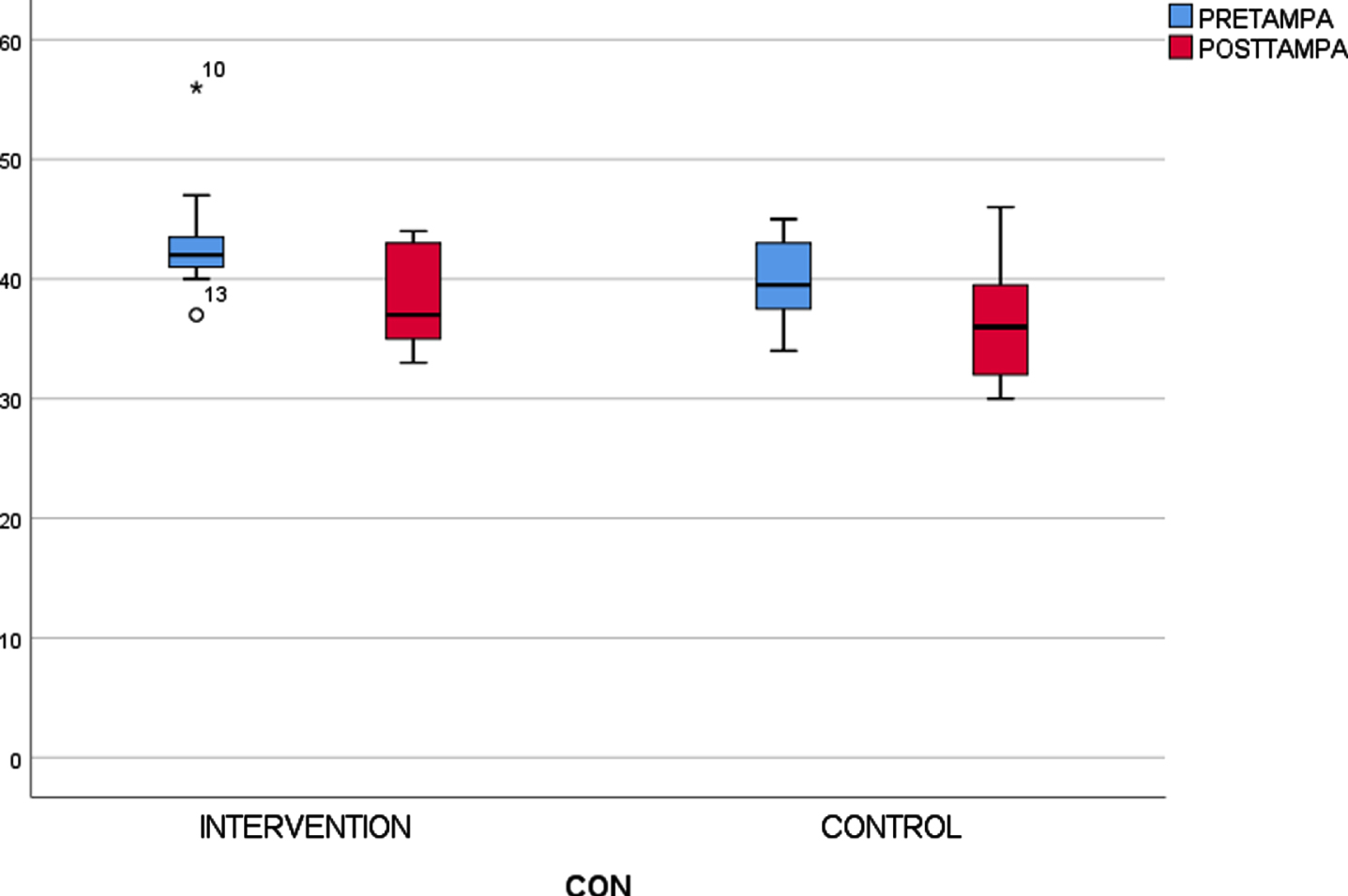
Pre and post-intervention TSK scores for each group.
PCS scores in Fig. 3 shows reduced post-intervention scores in both of the groups, with the same pattern as the post-intervention KOOS-PF in the intervention group. TSK scores in Fig. 4 demonstrated the same pattern, although the spread of the data was not as wide.
Sample size calculation.
Inspecting the raw data identified an outlier in the intervention group, which appears to be responsible for the large spread, as seen in Fig. 2. The participant’s pre-intervention KOOS-PF score was 25.0, but this reduced to 9.09 which was contrary to the participant’s subjective report that her symptoms had improved prior to completing the questionnaire. Once this outlier was removed, the central tendency and distribution of the data was more consistent with the anticipated results.
The time taken to complete the KOOS-PF was within the suggested time frame of 10 minutes [23] with the TSK and PCS taking less than five minutes each. Patients were able to complete the three questionnaires without assistance in 15 to 20 mins.
Sample size calculation
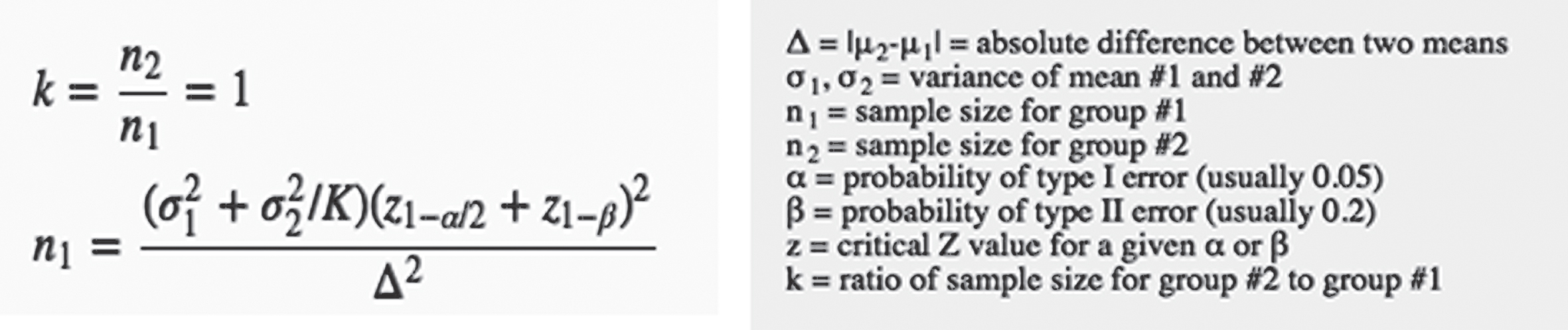
The data from the results for each of the outcome measures was used in the following equation (Equation 1). This was used to determine the number of participants required for a larger study with α= 0.05 and β= 0.2 [36] to calculate sample size for a two arm efficacy study.
Post-intervention means and standard deviations for each of the outcome measures in each of the groups (Table 2) were used in the equation. The participant who was an outlier on KOOS-PF was included in all sample size calculations. Each total sample size has been inflated to include a 20% drop out allowance: KOOS-PF: 2124 PCS: 150 TSK: 172
Although the dropout rate for this current study was slightly higher at 20.8%, a 20% drop out rate has been used in the sample size calculations as this is consistent with other PFP research.
Discussion
This randomised feasibility study achieved its primary objective by demonstrating that it would feasible to evaluate the intervention in a future study. Additionally, it also addressed the secondary objective and informed a series of sample size calculations for a future study by collecting data from three different patient reported outcome measures (PROMs)
This study was necessary because research shows that patients diagnosed with PFP have elevated levels of kinesiophobia and catastrophizing [37], however the optimal treatment approach to influence these psychological factors has not been identified.
Recruitment
Prior to the study commencing, audit data suggested 104 patients would be eligible to participate over a 12-month period, with a recruitment rate of eight per month from three sites in one NHS hospital trust. However, participants were recruited at a slower rate of three per month.
Recruitment to the study was conducted by participant identification physiotherapists in the MCAS service. Review of referrals to the study identified that more participants (n = 16) were recruited by the most senior rather than the junior participant identification physiotherapists (n = 8). This was unexpected as there was a ratio of 1 : 4 for these staff groups. This might have been because junior clinicians were less confident in their diagnosis of PFP, as opposed to it being an issue of competence. Research has identified that physiotherapists’ with one years’ experience are competent at diagnosing knee disorders [38], which is supported by this study where only three of the 31 participants screened were ineligible, suggesting that the participant identification physiotherapists were competent. Time management could have been an issue, with junior clinicians having less time available to discuss the study, again this is consistent with previous research, which identified that time can impact on recruitment into RCTs [39]. A potential solution would be to utilise research clinicians, who are experienced in screening patients and whose sole role is to recruit to research.
Retention
Five participants were lost to follow up (control n = 4, intervention n = 1), representing ∼20.8% of participants, which is similar to other studies [40].
In this study, recruitment and retention may have been affected by the intervention being at one site only. This was a pragmatic decision as the research physiotherapist was based there, but it did mean that only patients able and willing to travel could participate.
Future studies are likely to have multiple physiotherapists delivering the intervention at different sites, or alternatively employ online or digital platforms. Both of these strategies would reduce the burden on patients and might encourage their participation in research [37]. These strategies might then translate into enhanced recruitment and retention.
If there is concern about slow recruitment and borderline retention, a future study could also use an adapted RCT design whereby an internal pilot with clear progression rules are used to assess if the study should continue onto a main trial, thereby ensuring the research is robust and resources are not wasted [41].
Intervention fidelity
Self-reflection of the intervention identified fidelity, with multiple sites, would continue to be ensured with ongoing training and monitoring within and between sites, this is particularly important if multiple clinicians deliver the intervention. Another potential strategy to promote fidelity might include using treatment manuals [42] or video to deliver the intervention as it would ensure that every participant receives the same information regardless of the clinician. This strategy has been used successfully to reduce maladaptive belief in adolescents with PFP [37], although, the results should be interpreted with caution as this study was underpowered. If videos are considered this should be done with caution to ensure that it does not change the intervention to the point that the findings of this feasibility study are compromised.
Sample size for a future two arm efficacy study
Alternative sample sizes for a future two arm efficacy study were calculated using each of the outcome measures using the post-intervention means and standard deviations; which resulted in different sample sizes for each measure.
The MCIC for KOOS-PF is recommended as 16 [22]. In this study an average change greater than 16 was found in both the control and intervention groups respectively (19.3, 16.5). Removing the outlier’s scores increased the mean change in the intervention group to 19.8; this might indicate that some participants may struggle to complete the KOOS-PF. It should be made clear to participants that they must ask if there is anything that they do not understand with the research physiotherapist readily available. Using the KOOS-PF to calculate a sample size for a future study suggested 2124 participants would be needed. This would be a significant challenge in terms of recruitment even if a multicentre approach were to be conducted.
The PCS MCIC is reported to be 9 points [27]. In this study the average change for the control and intervention was –9.3 and –8.4 respectively demonstrating a greater change in the control group. However the PCS MCIC for PFP has not been identified and the score of 9 was recommended for lower back pain patients [27].
Scott et al. (2014) [26] has stated that a high score for the PCS was considered to be greater than 24. In this study the average pre-scores, 18.4–23.3 for PCS was considered at the low end; in which case the educational based intervention may have had less of an impact as there was less room for improvement in patients with PFP. This has implications when considering future suitability of this outcome as a primary outcome measure in a larger study.
The TSK cut off point between individuals with high and low fear is 37 [29]. This study had a pre-score of 43.2 in the intervention and 39.9 for the control, placing both in the high fear grouping. There were 9 in the control group and 12 in the intervention group with pre-TSK scores of 37 or more.
The average post-intervention change for the TSK score was –3.5 for the control and –4.5 for the intervention. Therefore, only the intervention group achieved the reported MCIC of 4 [30]. Priore et al. (2019) [43] reported a change of –5.64 in TSK when using a knee brace with PFP participants, although this study was limited to 6 weeks. The changes in the TSK scores are in line with those from this feasibility study. Although this was a feasibility study and not powered to detect differences between the 2 groups the TSK was able to identify a clinically important change in the intervention group.
In this study, the TSK appeared to be the most appropriate outcome tool for assessing the education session delivered to this patient population and yielded a suggested future sample size of 172 which with appropriate resourcing could be achievable through a multicentre study.
Strengths and limitations
Risk of bias
There are inherent risks of bias in this study. It was not possible to mask or blind participants to their group allocation due to the nature of the intervention and the outcome measures were also self-reported. In addition, the research physiotherapist collected participants’ outcome data and delivered the intervention, which might also have introduced social desirability bias if participants felt compelled to report better outcomes than they were actually experiencing. This could be mitigated by having sufficient funding to ensure the involvement of multiple research physiotherapists; e.g. one to deliver the intervention and one to assist in outcome data collection.
Recruitment
Recruitment was slower than anticipated, thus prolonging the duration of the study, however this finding was beneficial as it should provide a more realistic recruitment timescale for a future appropriately powered study.
Retention
The drop out from this study was consistent with similar studies which also had a dropout rate of 20% [44]. Retention may have been impacted by participants’ ability to regularly attend the intervention site for treatment. A future study should consider ‘releasing’ participants back to the original site once they have completed the intervention to undergo usual care or the use of supportive digital technology.
Greater involvement of patients with PFP as part of patient and public involvement (PPI) would be essential in taking the results of this study and refining the design for future research. This is particularly important because it is likely that the PPI group would identify potential difficulties and solutions to the proposed design, which would have a positive impact. This is particularly important if multiple-centres are to be considered for an efficacy study, which would be pragmatic as the required sample size to assess efficacy is large, and would not be realistic to conduct in a timely fashion at one site only.
Intervention fidelity
A limitation of this study was that it was delivered solely by the research physiotherapist who was restricted to a satellite clinic and there were no resources available to fund an independent assessment of intervention fidelity. Furthermore our fidelity assessment focused only on delivery and not other aspects of fidelity, such as receipt; ensuring participants understood the information provided in the intervention (experimental conditions), and enactment; whether or not the participant applies the information and knowledge they have acquired to their own lives [34]. However, the study protocol was pre-registered with Clinicaltrials.gov NCT03784339 was used to review if the intervention had been delivered as intended.
Future research recommendations
This feasibility study has answered some of the uncertainties around the feasibility of conducting this research. Following amendments highlighted from this study it should now be tested further in a pilot study, guided by the MRC framework [20] prior to a larger suitably powered study to assess efficacy. An appropriately powered future study should endeavour to identify if the education session is effective across varying degrees of chronicity. In this study the mean duration of pain was over 3 years in both the control and intervention groups.
The control group in this study had a greater improvement in the KOOS-PF and PCS, but the intervention group had a greater improvement in the TSK. Future studies should consider only including participants with high scores on the identified pre-intervention outcome measures, or at least analyse large data sets further to see if the intervention has a greater effect on patients with high TSK scores and thus supports the theoretical proposition for the mode of action of the intervention. This would potentially demonstrate greater change in pre-post-intervention scores which would influence the sample size calculation. Furthermore, Machlachlan’s (2017) [37] systematic review into the psychological features of PFP recommends subgrouping patients to guide treatment, as although there is emerging evidence of the benefits of subgrouping and targeted physical intervention [10, 45] [9 & 44] it remains unknown if a similar approach would be useful for psychological features.
The stated aims of this study were to; determine the feasibility of a future two arm efficacy RCT comparing standardised physiotherapy with an education intervention addressing patients’ catastrophizing and kinesiophobia. A limitation of the study was that we did not include a specific outcome measure to identify levels of mental distress. However, the PCS has been found to have a significant degree of overlap, identified on correlation matrix, among all measures of emotional distress [24]. The secondary objectives were to generate and analyse clinical data from three different outcome measures to inform the appropriate sample size that would be required for such a future study.
This study has demonstrated that a larger study would be feasible based on the findings. The TSK appears to be the most appropriate outcome tool and yielded a suggested future sample size of 172 patients. A future pilot RCT would benefit from the inclusion of strict progression criterion in view of the challenges associated with recruitment and retention. The study has achieved its secondary objectives of generating enough clinical data to inform a sample size calculation for all outcome measures used.
Footnotes
Acknowledgments
JJ would like to acknowledge the support and input from their academic supervisors JS and PG who have contributed to manuscript revisions.
JJ would also like to thank the Musculoskeletal Association of Chartered Physiotherapists who provided a grant to allow him to attend a lecture on ‘Patellofemoral Pain Uncovered’ by Claire Robertson of Wimbledon Clinics.
Conflict of interest
The authors have no interests to declare.