
Abstract
PURPOSE:
Sport-related concussions (SRC) are common, especially in rugby (3.00 incidents per 1000 athletic exposures) and American football (0.08 per 1000 athletic exposures). Physiotherapists should be aware of how to assess and manage cases with SRC. The purpose of this study was to assess the knowledge of SRC among physiotherapists.
METHODS:
The self-administered survey consisted of 16 questions related to physiotherapists’ knowledge in managing SRC patients, case identification, and preventive measures. Countries were divided into regions based on World Physiotherapy regions. Data were analysed using a one-way Analysis of Variance (ANOVA) with Tamhane’s T2 post hoc test.
RESULTS:
A total of 276 male (53.4 %) and 241 female (46.6%) physiotherapists participated. The survey scores ranged from 40% to 100%, with an average score of 62.7%. A master’s degree was the highest educational qualification (46.4%) recorded. There was a difference in the score based on participant qualifications (Welch’s F (4, 58.37) = 15.03, p < 0.001). Participants with a Doctor of Philosophy (PhD) degree (73.8±14.6%) or a fellowship (73.0±19.5%) or a masters’ degree (MSc) (62.7±18.5%) obtained greater scores than participants holding a bachelors’ degree (56.7±13.8%, p < 0.001). Furthermore, there was no difference in the survey score based on participants’ region (Welch’s F (4, 143.3) = 0.08, p = 0.988).
CONCLUSIONS:
The results suggested that many physiotherapists worldwide are aware of the current SRC assessment and management guidelines.
Introduction
A sport-related concussion (SRC) can be described as a traumatic brain injury while engaging in a sports event or exercising [1]. It results from a direct or indirect biomechanical force conveyed to the head, leading to physical, cognitive, emotional and sleep changes [2, 3]. Researchers found that sports categorised as contact sports such as American football, basketball, and rugby had the highest number of SRC [4–6]. In a systematic review by Prien et al. [7], rugby matches comprised the highest SRS incident rate at 3.00 concussions per 1000 athletic exposures (AEs) compared to the lowest incident rate of 0.08 per 1000 AEs in men’s football training. Similarly, an epidemiological study by Fraser et al. [8] looking at 11 National Collegiate Athletic Association Sports (NCAA) found the highest injury rates of 8.82 per 10,000 AEs in women’s softball, 7.20 per 10,000 in women’s field hockey and 7.20 per 10,000 in men’s baseball. More specifically, SRC accounted for 16.1% of all ball-contact injuries. In elite soccer, it was reported that 58% of SRC occurred due to impact from heading movements, 41% occurred from impact to the head from the upper extremity, and 33% were due to other head-to-head impacts [9]. West et al. [10] concluded that SRC was the most common injury in English rugby, showing an increased incidence rate from 2011 to 2019.
SRC makes up 15% to 20% of the reported mild traumatic brain injuries [11]. It is reported at a rate of 0.23 concussions per 100 player-seasons in baseball, 0.75 concussions per 100 player-seasons in basketball and as high as 3.66 concussions per 100 player-seasons in American football [12]. In Pennsylvania, SRCs alone account for 59.9% of the concussion incidents reported in students [2]. A pooled analysis revealed an incidence rate of 19.1 per 1000 match hours in amateur players in rugby league compared to semi-professional players, who experienced 3.1 incidents per 1000 training hours. However, semi-professional players had three times greater concussion risk than their amateur counterparts during matches [13].
SRCs have gained more attention recently due to their detrimental short-term and long-term effects on the players. Short-term effects of SRC may include headaches and decreased reaction times. On the other hand, long-term effects, which can last up to one year after the injury, include a significant decline in cognitive abilities such as executive functions and decision-making, decreased attention spans and decreased processing speed leading to a decline in the quality of life [11, 14].
When researching the knowledge of SRC amongst the individuals who would be present during a competition like the fans, coaches, athletes, parents of young athletes, and physiotherapists, it was shown that the public’s knowledge of SRC is considered modest [15]. For example, when interviewing young soccer players between ages 8 and 14, many failed to recognise common concussive symptoms like confusion, nausea, and sleep disturbances [16]. High school and collegiate athletes in South Korea also showed a deficit in SRC awareness [17]. A recent study by Churton et al. [18] indicated that secondary school students know about the onset of symptoms, actions to avoid post-concussion, the possible complications, and the less distinguishable symptoms of SRC.
Understanding the physiotherapists’ knowledge about SRCs is of particular interest. In the United States of America, physiotherapists were found to have adequate SRC recognition and management knowledge. Physiotherapists achieved an average of 13.4 correct answers out of 15, and 97% of them correctly identified a cluster of symptoms following a concussion. Also, 89.8% believe that the most critical action is to refer the patient to a physician if post-concussion symptoms appeared [19]. More recently, Reid et al. [20] showed that trained physiotherapists in New Zealand knew SRC symptoms and management.
Even though the reported statistics indicate that physiotherapists know about sports concussions in particular countries [19, 20], there are no internationally reported statistics. Moreover, inconsistencies in the concussion recognition, assessment, and management on an individual level due to the varying educational background can affect the outcome and the decision-making process [19]. Additionally, identifying the role of physiotherapists within a multidisciplinary team in managing cases with an SRC is essential. Considering how involved physiotherapists are in recognising and managing SRC, it is vital to assess their awareness and ultimately correct any misconceptions in specific SRC recognition and management areas. Many registered physiotherapists worldwide hold varying levels of education; thus, the purpose of this study was to investigate SRC awareness amongst international physiotherapists and examine any association it may have with their geographical location and education level.
Methods
Survey development and dissemination
A survey to assess the awareness of international physiotherapists in SRC was explicitly developed for this study. The survey questions were developed based on information published by the University of Michigan School of Kinesiology Concussion Center [21]. Before disseminating the survey, a pilot test was conducted by questioning 30 licensed sports physiotherapists of various experience levels. The participants were requested to rate each question for clarity and relevance on a scale of one to five. Questions scoring below an average of four were discarded. However, all questions did score five and were considered suitable for this study.
The self-administered survey consisted of sixteen questions in English. The first question was regarding the informed consent and participation agreement. The following five questions aimed to collect information about the participants’ demographics, including age, sex, education level, job title, and country of practice. The remaining ten questions were related to specific areas of SRC via multiple choice answers in the following domains: (1) knowledge of concussion signs and symptoms; (2) assessment and referral; and (3) management of concussion cases. The first domain was based on a cluster of concussion signs and symptoms, while the second domain consisted of case scenarios. Lastly, questions of the third domain were based on decision-making statements.
A survey invitation was distributed through the World Physiotherapy member’s associations to include the broadest range of physiotherapists, including specialised in sports injuries rehabilitation. The invitation provided a summary of the survey and encouraged physiotherapists with or without SRC experience to participate. Participants were prompted to click on an electronic link that led them to the survey description and the survey itself. The survey was completed anonymously via a web-based form and was available from April through October 2020. The Biomedical Ethics Committee at Umm Al Qura University reviewed and ethically approved the study (Approval Number: HAPO02K012202010464).
Survey software and administration
The survey was uploaded to Survey Monkey (SurveyMonkey Inc. San Mateo, California, USA), a recognised online survey software. The respondents were provided with the link, and once a respondent had submitted the survey, they could not respond again. Results were compiled using the Survey Monkey software. All responses were voluntary, anonymous, confidential, and for research purposes only.
Sample size and statistical analysis
According to World Physiotherapy, there are 625,000 physiotherapy members worldwide. Considering a 5% margin of error at a 95% confidence level, the target number of physiotherapists was 384.
The score of each question was binary (correct answer = 1; incorrect answer = 0). The scores of the survey were computed into percentages for data analysis and data reporting. Responses were organised in Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA, USA).
Descriptive statistics were computed to describe the participant’s demographics and survey data. A one-way Analysis of Variance (ANOVA) was used to determine differences in the overall survey score based on respondents’ qualifications and World Physiotherapy regions. Graduate and postgraduate qualifications were categorised as a Bachelor of Science (BSc), Master of Science (MSc), Doctor of Physiotherapy (DPT), Doctor of Philosophy (PhD) and Fellowship. Like the World Physiotherapy classification, the countries were organised into regions into Africa, Asia Western Pacific, European, North America Caribbean and South America regions. Tamhane’s T2 post hoc test was used to explore pairwise comparisons. The Alpha level was set at 0.05 for all analyses. Statistical analysis was performed using SPSS version 24.0 (SPSS Inc, Chicago, Illinois, USA).
Results
A total of 600 invitations were sent, and 517 participants from 57 countries completed the survey with a response rate of 86.2%. Most participants were males (n = 276, 53.4%) and the majority aged 20 to 29 years (n = 208, 40.2%). The most-reported educational qualification recorded among the respondents was having an MSc degree (n = 240, 46.4%) followed by a BSc degree (n = 138, 26.7%). Regarding the job title, most respondents were specialists (n = 288, 55.7%) and senior specialists (n = 159, 30.8%). Based on the region, the biggest participation rate was from the European (n = 194, 37.5%) and Asia Western Pacific regions (n = 134, 25.9%). The participants’ characteristics are presented in Table 1.
Participant characteristics
Participant characteristics
Notes: *, or equivalent.
The survey scores varied from 40% to 100%, with an average score of 62.7%. Correct answers ranged between 89% to 100% for the knowledge of concussion signs and symptoms section and 68% to 100% for the assessment and referral section. Lastly, lower scores between 27% and 46% of the correct answers were reported to manage the concussion. Out of all areas, questions related to the concussion law for youth athletics and activity recommendation scored the lowest (27% and 34%, respectively). Further details about the results of the question can be found in Table 2.
Survey questions, domains and analysis
The ANOVA test results indicated a statistically significant difference in the survey scores based on participant qualifications (Welch’s F (4, 58.37) = 15.03, p < 0.001). The highest mean (±[SD (Standard Deviation)]) reported scores were for participants holding a PhD degree (73.8±14.6%) and a fellowship (73.0±19.5%) compared to the other qualifications. Pairwise comparisons revealed that participants with a BSc as a base degree scored significantly lower than participants holding a MSc or PhD degrees (M = –6.00, 95% CI (Confidence Intervals) [–10.72, –1.28], p = 0.004; M = –17.13, 95% CI [–23.56, –10.69], p < 0.001). Similarly, participants holding MSc or DPT degrees scored significantly lower than participants with a PhD degree (M = –11.13, 95% CI [–17.59, –4.66], p < 0.001; M = –12.95, 95% CI [–21.47, –4.43], p < 0.001). Furthermore, there was no statistically significant difference in the survey score between participants with a fellowship and those holding a PhD (p = 0.999). Similarly, participants holding MSc degrees showed no differences in scores when compared to the participants with a DPT (p = 0.999) or a fellowship (p = 0.755). Figure 1 depicts the mean plots for survey scores based on participants’ educational qualifications.
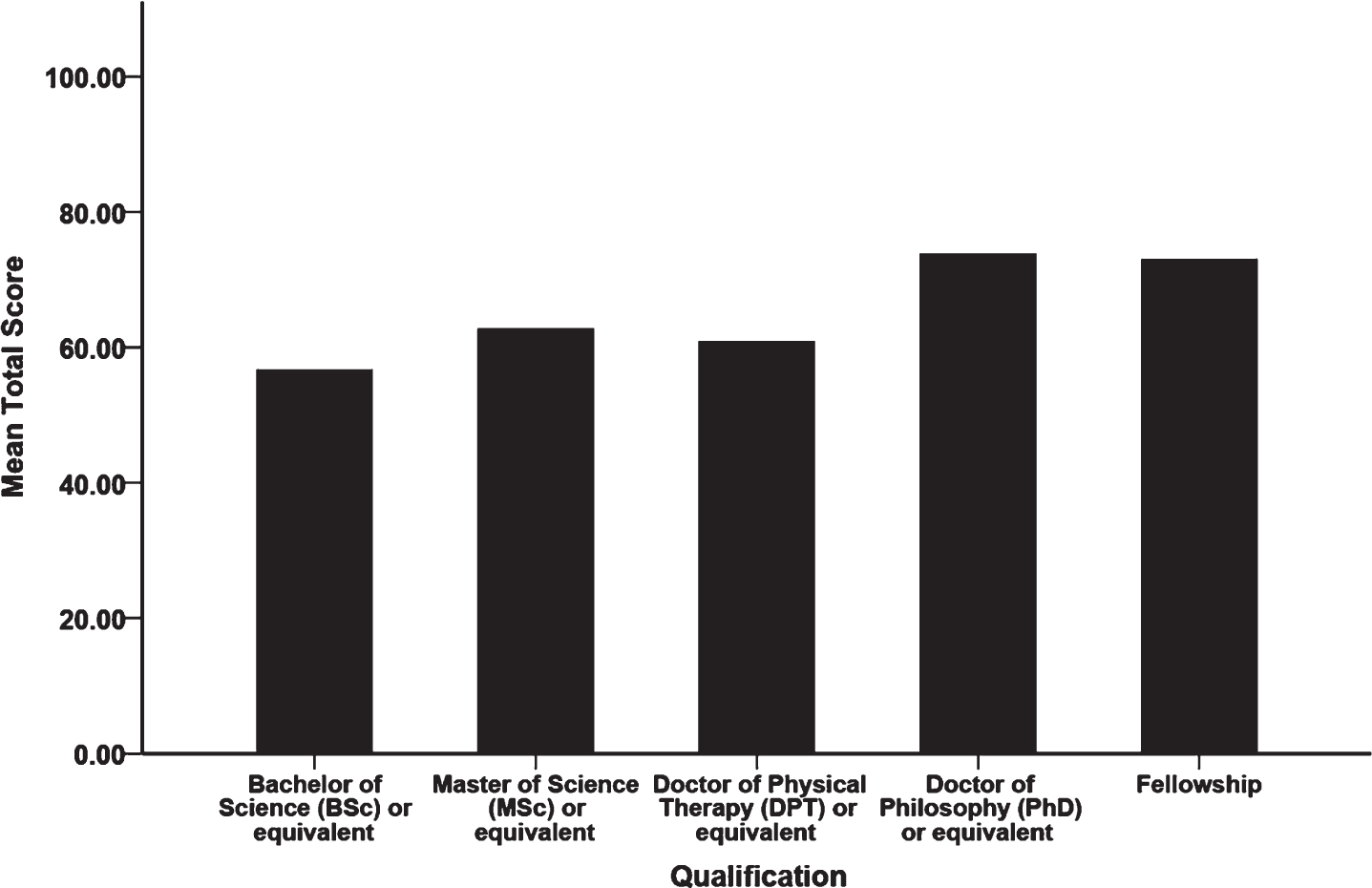
Distribution of the participants’ qualifications.
Regarding the World Physiotherapy region, the regions’ mean survey scores were remarkably close with no significant difference between the regions (Welch’s F (4, 143.3) = 0.08, p = 0.988). Further description of the analysis is demonstrated in Table 2.
SRC carry a small proportion of all sports injuries but may result in significant functional and cognitive changes. It is prevalent in rugby and match games compared to soccer and training sessions [7]. The current study results indicated that physiotherapists worldwide seem to understand SRC assessment and management. These results are comparable to research by Yorke et al. [19], who surveyed 1416 physiotherapists in the US using a 55-question electronic survey. More than 97% of participants correctly identified the main symptoms of concussion. The same study showed that more than 94% of the participants correctly utilised multiple assessment tools in evaluating patients suffering from a concussion. Similar results were also reported by Reid et al. [20], with 98% of the New Zealand physiotherapists recognising the SRS signs and symptoms.
The survey results showed no significant difference in awareness levels between participants with a fellowship and those holding a PhD. In contrast, physiotherapists holding only a bachelor’s degree scored much lower than their peers holding graduate degrees. Generally, the participants seemed to have a significantly greater awareness of SRC assessment and management if they had graduate degrees, proportional to the degree’s level. It is not surprising since SRC and other causes of concussions are not thoroughly explored in physiotherapy bachelor programs. A study involving 344 students from four different universities in South Africa evaluated the SRC assessment, management, and return to play plans knowledge of these students. The results indicated that only one student passed the minimum “safe” mark set at 75% by the surveyors. Thus, the study authors suggest that most physiotherapists with a bachelor’s degree as the highest educational qualification cannot adequately assess and manage an SRC on or off the playing field [22]. These superior responses are most likely due to the day to day contact these participants have with athletes sustaining an SRC.
The academic qualification level may not be the only factor, but the information delivery method may also play a role. In their attempt to determine if a traditional teaching approach may enhance healthcare professionals’ knowledge about concussion, Hunt et al. [23] divided 35 novice healthcare providers into two groups. College sophomore medical dietetics students received no specific training. In contrast, the sophomore medical students studying athletic training completed a didactic intervention comprised of the related concussion assessment, management, and clinical experience. Halfway between the intervention and clinical experience, the group receiving concussion-related classes showed considerably higher scores than the other group (F1,33 = 5.40, P = 0.026; Cohen d = 0.664). However, at 30-week follow-up, their scores showed a significant drop in knowledge (F1,15 = 5.983, P = 0.027; effect size; Cohen d = 0.698). The authors concluded that poor retention might be why, which raised the alarm to review the teaching methods currently applied in medical schools. Provvidenza and Johnston [24] argue that problem and evidence-based practice, socialisation and peer-assisted learning are the three best educational strategies offering optimal learning for athletic and physiotherapists. Such methods ensure knowledge transfer and meet the needs of the various learning styles of the learners.
The results suggested that many sports physiotherapists worldwide are aware of the current standards and guidelines regarding SRC assessment, with correct answers ranging between 68% and 100%. In contrast, it seems they are not adequately aware of its management with correct answers between 27% to 46% only. Yorke et al. [19] also found that more than one-third of the participants in their study were unsure or believed that youth sustaining a concussion should not be managed more conservatively than adults. Such an impression is not accurate since youth are more susceptible to second-impact syndrome. Complete recovery from a previous concussion may lead to severe disability or even death [25].
Literature shows that gaps in physiotherapists’ knowledge of SRC are present in its management, as shown in this study. The low concussion management score of 35.6% was due to the low score of law knowledge for youth athletics reported at 27%. This lack of awareness in some SRC management regions may be due to the unfamiliarity of the updated information that could be achieved through continuing education that requires being updated on the published guidelines about SRC management. For instance, Schneider et al. [26] systematic review provides valuable information on the rest, management and rehabilitation following SRC. More recently, Schneider et al. [27] explained a decision-making model based on an individualised approach to tackle each case. To improve the physiotherapists’ knowledge, Yorke et al. [19] suggest employing neuroimaging, severity scales and implementing a more comprehensive application of concussion-related treatment in youth. On the other hand, Reid et al. [20] believe physiotherapists should be more associated with assessing and managing patients with SRC.
Based on the results of a multidimensional assessment process, SRC management is recommended to consist of rest for 24–48 hours, a gradual return to physical activity and sport [27]. Treating SRS in the youth population may be required to include conservative treatment and utilising diagnostic neuroimaging techniques and severity scales [19, 28]. Youth suffering from vestibular symptoms may also benefit from vestibular rehabilitation. Thus, practitioners dealing with sports cases are required to be experts and highly knowledgeable in assessing and managing SRC since sports activities carry the most significant risk of sustaining concussion injuries along with falls and motor vehicle accidents [28, 29].
The below-average score in specific areas related to the knowledge, assessment and management of concussion-related cases may be several reasons. It may be attributed to a lack of hands-on experience with injury and exposure. Another reason may be that the undergraduate academic programs’ curriculum content resembled higher average scores of physiotherapists holding graduate qualifications. More specifically, graduate degree holders may have been exposed to such cases due to their more ample clinical experience or familiarity during their graduate studies. As a practical application, Fremont et al. [30] utilised a massive open online course (MOOC) to educate SRC stakeholders such as healthcare professionals, parents, or persons who suffered concussions. Out of the 8368 registrants, 54.6% were healthcare professionals other than medical doctors. About 30% (2538 individuals) passed the six modules course, and 579 individuals intend to update or implement the concussion management protocol (CMP). Even though the number of stakeholders willing to implement the CMP is relatively low, MOOCs’ application, mainly if they were free, could positively impact the knowledge about SRC in the long term. Such observation supports the notion that increasing continuing education opportunities for physiotherapists may increase awareness. Moreover, Provvidenza and Johnston [24] indicated that evidence-based practice, socialisation and peer-assisted learning are amongst the most effective educational methods for physical and athletic therapists.
Limitations
The study covered a range of physiotherapists with varying academic degrees and geographical locations. However, the number of physiotherapists participating in a similar study could be increased by directly contacting physiotherapy associations and specialised interest groups in sports physiotherapy. Moreover, physiotherapists’ specialisation or interest in orthopaedics, sports injuries, SRC, or other disciplines was not identified.
Conclusion
International physiotherapists are knowledgeable about the signs and symptoms and assessment of SRC. However, according to the survey results, most of them are not aware of its management. Due to the importance of such a topic in treating sports cases, it is crucial to address the existing knowledge gaps related to the SRC. It can be achieved by combining clinical and field expertise with the latest guidelines in dealing with SRC. Utilising problem-based learning and evidence-based practice approaches as teaching methods may also prove to be beneficial. Such a method allows the best incorporation of the sports therapists’ skills in managing SRC conditions in sports and playfields with scientific knowledge and evidence.
Footnotes
Acknowledgments
The authors would like acknowledge Prof. Ross H. Sanders, Prof. Mohammed Alghamdi, Prof. Amir El Fiky, Dr. Ahmad Qasem, Dr. Amirah Akkam, Dr. Ehdaa Khaledi, Dr. Fahad Alkabkabi, Dr. Ibrahim Alramadhani, Dr. Mashaer Alyami, Dr. Nasser Alshamrani, Dr. Raed Almalki, Dr. Walaa Abutaleb for their expert opinion. The authors would like to thank all physiotherapists who participated in this project.
Conflict of interest
The authors declare that they have no conflicts of interest.
Data availability
Data are available upon request.
Ethical considerations
All procedures performed in studies involving human participants were following the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This project was reviewed and ethically approved by the Biomedical Ethics Committee at Umm Al Qura University (Approval No. HAPO02K012202010464).
Each participant read the participant information statement and consent to participate.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.