
Abstract
BACKGROUND:
After cardiac surgery, various pulmonary complications develop which require specific care. These complications affect pulmonary functions and can lengthen the hospital stay of patients, causing increased hospital costs and becoming an important cause of morbidity and mortality.
OBJECTIVES:
To investigate the short-term effect of inspiratory muscle training on pulmonary function after mitral valve replacement.
METHODS:
A sample of Thirty five patients (35.5±3.29 years) who underwent mitral valve replacement. Spirometric parameters were measured before and after intervention including forced vital capacity (FVC), forced expiratory volume in the first second (FEV1) and ratio of forced expiratory volume in the first second to forced vital capacity (FEV1/FVC). All participants had received postoperative Inspiratory muscle training (IMT) from the first day in the inpatient unit after discharge from intensive care unit till hospital discharge. Paired t-test was used to investigate differences between means of pulmonary function measures (P < 0.05). Effect size was calculated and post hoc power analysis was performed.
RESULTS:
After one week of postoperative IMT there was a statistically significant improvement in the studied spirometric parameters (FVC, FEV1, FEV1/FVC) (p = 0.01). All studied spirometric parameters showed very large effect size (d >0.8). The post hoc power analysis revealed that the study power was more than 90%.
CONCLUSION:
One week of post-operative IMT may have a beneficial short-term effect in improving pulmonary functions after mitral valve replacement.
Keywords
Introduction
Mitral valve disease patients may exhibit reductions in lung volumes due to inspiratory muscle weakness in cases of pulmonary vascular congestion. The inspiratory muscles are compromised due to poor nutritional status that lead to decreased muscle mass and strength, increased work of breathing, in cases of long-standing mitral valve disease [1, 2].
Pulmonary hypertension develops in these patients also, as a result of combination of transmission of raised left atrial pressure, pulmonary arteriolar vasoconstriction and obliterative changes in the pulmonary circulation [3].
The incidence of postoperative pulmonary complications is more common in upper abdominal and cardiothoracic surgeries and may include pleural effusion, atelectasis, pneumothorax, bronchospasm, respiratory infection, respiratory failure, pneumonia, acute respiratory distress syndrome (ARDS), and pulmonary embolism [4].
The cardiac surgeries predispose to abnormal changes in respiratory mechanics, lung volumes and gas exchange, leading to development of postoperative respiratory changes. These changes are due to various causes [such as the condition of the heart and lung preoperatively, the degree of sedation, intensity of surgical manipulation and the number of pleural drains] which leads to development of abnormal respiratory mechanics in the immediate postoperative period [5, 6].
Mitral valve surgery causes insufficient diaphragmatic breathing post operatively which contributes significantly to development of postoperative pulmonary complications. Consequently, there are consistent reductions in pulmonary volumes and flows, alveolar collapse, reduction of sputum clearance ability, increase of respiratory work and diminution of mechanical efficiency of the respiratory muscles [7, 8].
Inspiratory muscle training is one of the procedures followed to promote better efficacy in airway clearance, improving inspiratory pressure and prevent fatigue of the respiratory muscles [9], which aims to improve functional capacity, respiratory muscle strength and reduce imminent risks of developing post-operative complications in patients undergoing cardiovascular surgery [10].
In phase I of Cardiac Rehabilitation various physiotherapy techniques are routinely used such as diaphragmatic breathing exercises, effective cough, chest wall percussion and vibration, continuous Positive Airway Pressure (CPAP) may prevent further deterioration in pulmonary function and reduce the incidence of Post-operative pulmonary complications [4, 12]. Unfortunately, There is a controversy about the efficacy of these postoperative procedures in decreasing the incidence of Post-operative pulmonary complications and improving pulmonary flows and volumes [13].
Inspiratory muscle training (IMT) is a therapeutic tool and one component of pulmonary rehabilitation which improves respiratory muscle strength, reduce the severity of dyspnea, improve the exercise tolerance and improve pulmonary flows and volumes after cardiothoracic surgery [13, 14].
Despite the documented benefits of inspiratory muscle training in reducing Post-operative complications, its short-term effect on improving pulmonary function after cardiac surgeries is less clearly defined. So, this study was designed to investigate the short-term effect of inspiratory muscle training on pulmonary function after mitral valve replacement.
Methods
Study design
Single group pretest-posttest quasi-experimental study design.
Sample size calculation
The sample size calculation was initially performed with G*Power (version 3.1.0) considering the recommendations for adequate sample sizes to conduct experimental studies [15] using alpha level of 0.05, a confidence level of 95%, study power of 90%. The standard deviation and effect size for vital capacity of 0.9 and 0.8 respectively, were obtained from our previous unpublished pilot study. These assumptions generated a sample size of 35 participants taking into account a possible 20–30% drop-out rate.
Participants
A convenient sample of thirty patients aged 20–40 years with mean age (35.3 years±3.29) was recruited for the current study from 1st Jun till 30th July 2019. These participants had undergone elective mitral valve replacement in the university Hospital. The demographic characteristics of the study participants are presented in Table (1) and the flowchart of the study plan is displayed in Fig. (1). The participants were included in the study if they; 1) underwent elective mitral valve replacement; 2) post- operative clinically and medically stable; 3) normal body mass index (18.5- 24.9 kg/m2).
Baseline Demographic, Clinical and Operative Characteristics of the participants
Baseline Demographic, Clinical and Operative Characteristics of the participants
Continuous data are presented as mean (standard deviation), while categorical data are presented as absolute number (percentage %). BMI: body mass index.
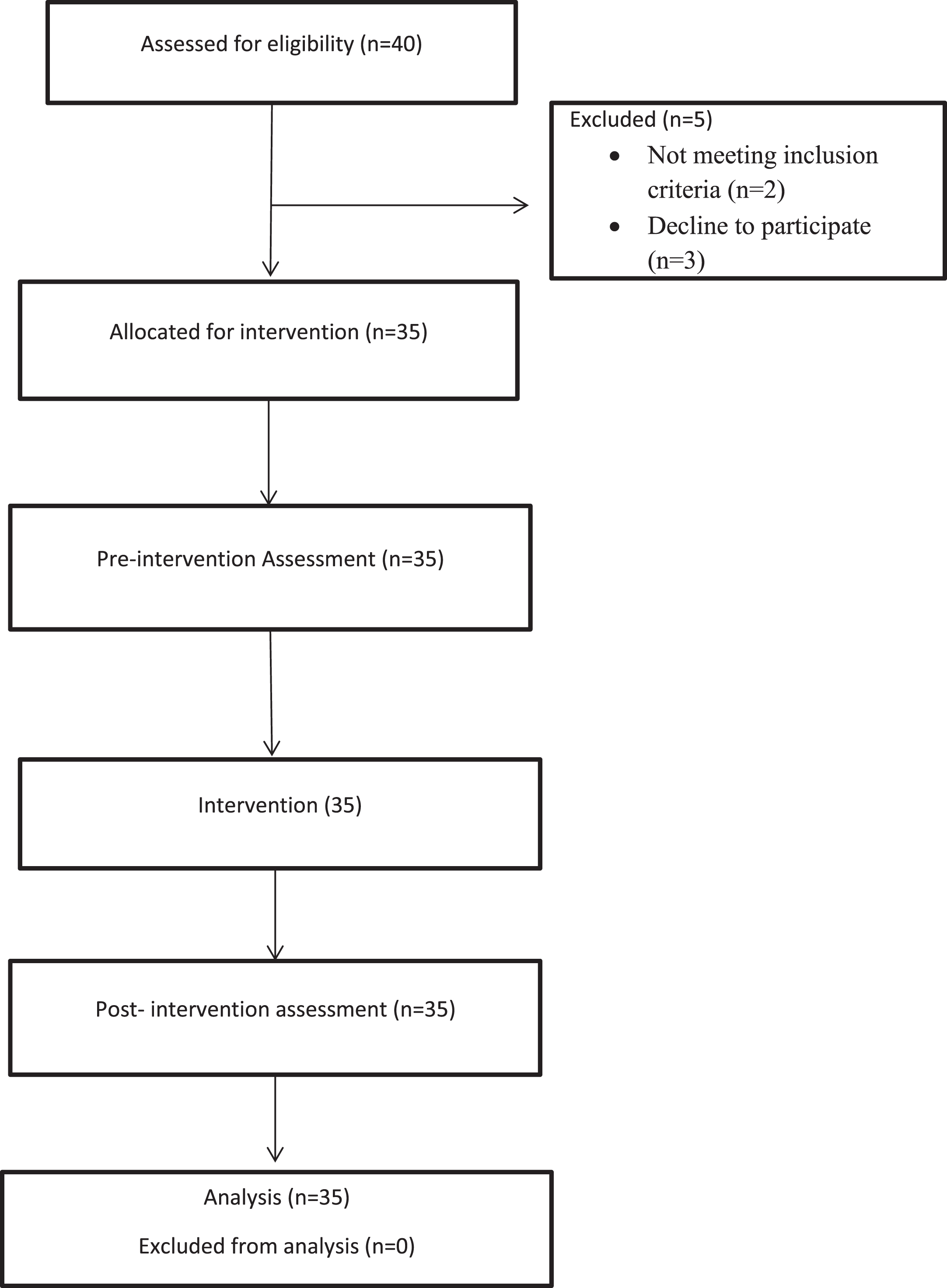
Flowchart of the study plan.
The exclusion criteria were: 1) obesity (BMI >30 kg/m2); 2) postoperative hemodynamic complications such as lung congestion or myocardial infarction; 3) history of pulmonary diseases such as chronic obstructive pulmonary diseases (COPD) or tuberculosis; 4) smokers; 5) post-operative renal failure or arrhythmia indicated for pacemaker; 6) post-operative prolonged ventilation [more than 24 hours].
The current study was conducted according to the code of ethics of the World Medical Association (Declaration of Helsinki) and had been approved by the Human Research Ethics Committee of South Valley University, Qena, Egypt.
Before surgery all patients were routinely refereed to physiotherapy department for pre-operative educational session of the traditional chest physiotherapy such as breathing exercise, cough mechanism, bed mobility. During this pre-operative education session, the study objectives and significance were explained to all patients as well as the importance of post-operative physiotherapy to avoid postsurgical complication. The post-operative Inspiratory muscle training had been explained in details. All patients were instructed that they have the right to refrain from the study any time as they wish. Written informed consents had been received from the participants before enrollment in the study.
After receiving the informed consent, demographic characteristics and medical history of each participant had been collected as shown in Table (1). After the preoperative educational session, each patient was scheduled for surgery and then referred to the ICU. During this period, no researcher had an influence on the management protocol adopted by the cardiothoracic surgery team.
After discharge from the ICU and in the first day in the inpatient ward, the pre-intervention evaluation of pulmonary function was performed. Pulmonary function tests were carried out in cardiopulmonary exercise testing unit (Oxycon pro-jager). A device used for measuring pulmonary function. According to American Thoracic Society (ATS) guidelines, Spirometry is an excellent outcome measure used for assessing pulmonary function [16]. Spirometry was performed with the patient in the seated position. It incorporates a microcomputer that processes the measurements and displays the calculated data. The measurements consisted of forced vital capacity (FVC), forced expiratory volume in one second (FEV1) and forced expiration ratio (FEV1/FVC). Pulmonary function values were based upon obtaining three technically acceptable maneuvers and the best of the three results were considered for analysis.
All patients initiated inspiratory muscle training with a pressure linear load inspiratory muscle trainer device (Threshold® Respironics® IMT) [Respironics, Cedar Grove, NJ 07009-1201; USA]. It is a small plastic handheld device with a mouthpiece and spring-loaded calibrated valve. A constant inspiratory pressure training load is controlled through a valve and the patient must generate an inspiratory pressure in order to open the valve and allow air entrance. The resistance can be changed up or down by changing the position of the spring-loaded valve.
The patients identifies the effort at the point that they can successfully execute 10 breaths against maximum resistance by the inspiratory muscle trainer depending on the patient’s rate of perceived exertion [17]. The rate of perceived exertion was determined by the modified Borg Scale of perceived exertion, as it is a reliable and valid tool for assessment of perceived exertion [18].
Training started with a load equal to 30% of the patient’s maximum inspiratory pressure. The patients had been advised to use the inspiratory muscle trainer from sitting position. The patients were instructed to avoid leaning forward during IMT, as this leads to overestimation of the values. This training was performed 3 sets with 10 repetitions of deep breaths against the trainer twice daily until hospital discharge and the recommended training time was (15 to 20 min).
On the day of hospital discharge, Spirometric parameters [FVC, FEV1, FEV1/FVC] were reevaluated in order to compare the results with the pre-intervention values. The pre- and post-intervention pulmonary function evaluations were carried out by an independent examiner who was a senior cardiopulmonary physiotherapist with 15 years of clinical experience. This examiner was blinded to the objectives of the study and the participants’ identity.
Statistical analysis
The quantitative variables were expressed as mean and standard deviation (SD), while the qualitative variables were expressed as an absolute value and percentage (%). The measured pulmonary function values were expressed as mean (SD). The normality of data was investigated using Shapiro-Wilk test. Paired t-test was used to investigate the difference between pre and post-intervention results. Effect size and post hoc power analysis were performed to determine the level of type II error. Effect size was interpreted according to Cohen’s Classification of effect size [small = 0.2; moderate = 0.5; large = 0.8] [19]. All statistical tests were conducted using IBM SPSS statistics for Windows, version 23 (Armonk, NY: IBM Corp). The level of statistical significance was set at P<0.05.
Results
Descriptive statistics of the demographic and clinical characteristics of the participants were presented in Table (1). The data were normally distributed according to Shapiro-wilk test (P = 0.18). There were no missing data in the current study.
The mean value of FVC was (2.61±0.28 L) before the intervention program and was (3.04±0.25 L) after the inspiratory muscle training. Paired t-test revealed statistical significant difference (P < 0.05) between the pre and post-intervention values of FVC (Table 2).
Pulmonary functions before and after inspiratory muscle training
Pulmonary functions before and after inspiratory muscle training
MD: Mean difference; SD: standard deviation; FVC: forced vital capacity; FEV1: forced expiratory volume in one second; FEV1/FVC: forced expiration ratio; L:Liter. *paired t-test.
The mean value of FEV1 for the study group was (2.07±0.29 L) before the program and was (2.63±0.23 L) at the end of program. The Paired t-test revealed statistical significant difference between the pre and post-intervention values of FEV1 (P < 0.05). Similarly, there was a statistical significant difference between the pre and post-intervention in FEV1/FVC values (P < 0.05) as presented in Table (2).
It is evident that the current study is sufficiently powered (>90%) for the outcome measures [FVC (94%); FEV1 (98%); FEV1/FVC (91%)]. This was further confirmed and justified with the large effect size (>0.8) that had been demonstrated by the studied spirometric parameters (Table 2). Hence, these results prove that there is significant improvement of pulmonary function measures after the post-operative program of IMT with type II error less than 10%
The aim of this study was to investigate the short-term effect of inspiratory muscle training on pulmonary function after mitral valve replacement surgery.
This study revealed significant improvement in pulmonary function after receiving a postoperative IMT program for a short period of time (one week) in the patients who underwent mitral valve replacement. This improvement was reflected by significant increase in the studied spirometric parameters (FVC, FEV1 and FEV1/FVC) after receiving IMT program (p < 0.05). This was further confirmed and justified by a very large effect size (d >0.08) and power analysis of more than 90%, reflecting the beneficial effect of IMT on pulmonary function.
The improvement in pulmonary function in the current study after IMT is most probably attributed to restoring of the respiratory muscle strength and endurance as well as maintaining airway patency leading to better prognosis and reducing the hospital stay [9, 20].
Moreover, it was reported that IMT induces an improvement in the size of type II muscle fibers of the respiratory muscles leading to increase in the shortening velocity and of inspiratory muscles, allowing more time for expiration and reducing lung hyperinflation [17, 21]. This may facilitate lung emptying and explain the improvement in pulmonary function observed in the current study.
The current study results were consistent with the study done by Cordeiro et al., (2016) [9] which investigated the effect of inspiratory muscle training on functional capacity and inspiratory muscle strength in patients undergoing cardiac surgery. They concluded a significant improvement in inspiratory muscle strength and functional capacity after inspiratory muscle training program during hospital stay.
The results of the current study were supported by Weiner et al.,(2004) [22] who concluded that IMT had improved inspiratory muscle strength, functional capacity presented by 6-minute walk test (6MWT) and a clinically significant decrease in dyspnea sensation at rest as well as during exercise.
The current study results were consistent with the previous study [23] which reported that the positive effects of the inspiratory musculature training on pulmonary ventilation were demonstrated by improved forced vital capacity (FVC) and FCV/FEV1 ratio. Moreover, Sasaki et al.,(2005) [14] reported that Inspiratory muscle training enhances respiratory muscle function and can potentially reduce the severity of breathlessness and improve exercise tolerance with the possibility of increasing walking distances and resulting in a better quality of life.
The current study results also agree with the results of the previous study done by Enright et al.,(2004) [24] which showed significant increases in lung volumes, diaphragmatic thickness and improvements in exercise capacity following IMT in age-matched subjects with cystic fibrosis.
A recently published systematic review[25] supported the current study. This systematic review reported that Pre- and postoperative inspiratory muscle training showed to be an effective intervention for patients undergoing cardiac surgery as it improves pulmonary function and reduces postoperative complications leading to reduction in the length of postoperative hospital stay.
Another study conducted by Riera et al.,(2001) [26] supports the current study results as the authors reported a significant improvements in inspiratory muscle function, walking capacity, pulmonary function, and health-related quality of life after IMT.
On the other hand, the current study results were inconsistent with the study done by Ahmed et al., [27] which evaluated the short-term effect of IMT combined with chest physiotherapy on lung function in moderate hospitalized COPD patients. They concluded that an increase in FEV1/FVC could be seen only after 4 weeks of IMT. The differences between results may be attributed to the differences in the sample characteristics (COPD patients) and the methodologies used which make the comparison between results of the studies difficult to be achieved.
What does this study add?
The current study has valuable clinical implication in the field as it proved that short period of post-operative IMT (7 days) is enough to improve pulmonary functions after mitral valve replacement. Based upon the current study results, IMT should be included as a basic part in the post-operative cardiopulmonary rehabilitation as it seems promising to improve lung functions and consequently avoid development of the post-operative pulmonary complications.
Limitations
The convenience sampling followed in this study and using a single group has a limitation for generalization of the obtained results. Moreover, the intervention protocol of IMT in the current study was designed for a short period of time (during hospital stay for one week), so further research is needed to investigate the long term effect of IMT on pulmonary functions after cardiac surgery with a better chance to follow up the patients over longer periods.
Conclusion
Deposit this is a single group quasi-experimental study conducted on a convenient sample, the short term effect of one week of post-operative IMT may have a beneficial effect in improving pulmonary functions after mitral valve replacement surgeries. However, further research regarding this issue should be addressed in the future.
Footnotes
Acknowledgments
Authors would like to express their gratitude to the patients who participated in the current study.
Author contributions
All authors contributed equally in the study, revised the manuscript and provided the final approval for publication.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The current study had been approved by the Human Research Ethics Committee of South Valley University, Qena, Egypt.
Funding
None.