
Abstract
BACKGROUND:
Proprioceptive neuromuscular facilitation (PNF) is one of the neurophysiological techniques aimed at reducing pain and disability. This systematic review objective addresses the current evidence on PNF techniques’ effectiveness in chronic low back and neck pain.
METHODS:
Literature search in PubMed, Scopus, Cochrane, Wiley and Ovid databases were searched until 2021. The content of the titles and the abstracts were analysed to gather information about the effects of PNF in chronic back and neck pain with outcomes of pain and disability. The quality of the studies was analysed by the Joanna Briggs Institute (JBI) critical appraisal score. Meta-analysis was performed on Visual Analogue Scale (VAS), Numerical Rating Scale (NRS) for chronic low back pain and Oswestry Disability Index (ODI), Roland Morris Disability Questionnaire (RMDQ) for disability.
RESULTS:
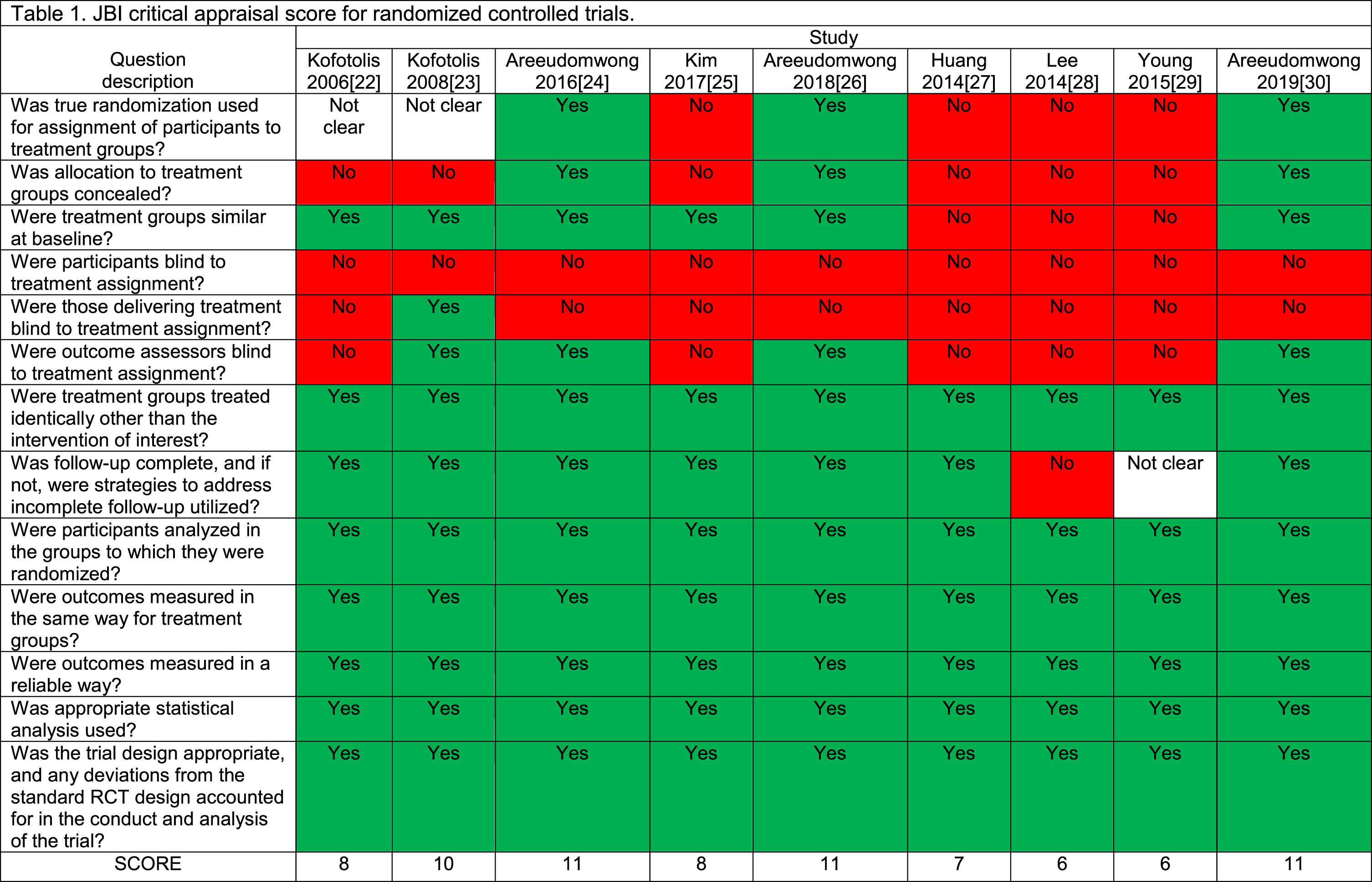
Nine studies addressed the different PNF based interventions on chronic low back pain, with a total of 416 participants. The intervention period ranged 3–6 weeks, and two studies conducted 12-weeks follow-up. Many studies measured pain using a VAS and NRS, whereas the disability through ODI and RMDQ. The JBI score ranged from 6/13 to 11/13. None of the PNF studies treated chronic neck pain.
CONCLUSION:
PNF might be beneficial for reducing low back pain and related disability. The long term effects of PNF on chronic low back pain, and also to determine its benefits on chronic neck pain are warranted in future studies.
Introduction
Mechanical backpain is described as pain occurring due to an injury, deformity or overuse of the spinal anatomical structure such as bone, ligaments, intervertebral discs, apophyseal joints, spinal nerves, and meninges associated with mechanical stress and prolonged abnormal posture, as well as psychosomatic issues [1]. A persisting pain for 12 or more weeks is stated to be chronic. Mechanical neck pain is attributed to the generalised neck and/or shoulder pain, and the symptoms are provoked by the movement or sustained neck positions or palpation of the cervical muscles [2]. Its prevalence increases by 43–66.7% with advancing age [3]. Worldwide, neck pain is the fourth leading cause of disability [4]. On an estimate, about 22–70% of the population experience neck pain at some point in their lifetime [5]. Mechanical low back pain extends superior to the inferior gluteal folds and inferior to the costal margin due to muscle tension, or stiffness over this region [6]. It is one of the most common disabilities encountered within 45 years of age and seems to be the most expensive health problem for those aged 20–50 years [7]. The highest global burden of disease related to years lived with a disability affect up to 85% of the population worldwide [8].
The interventions used for chronic neck pain (CNP) are physical exercise [9, 10], endurance training, strength training [11, 12], electrotherapy, manual therapy and moist heat pack [13–15]. A Cochrane review recommended the static and dynamic stabilisation along with stretching of scapular muscles [16], strengthening exercises and combined therapeutic exercise with manual therapy than a single treatment alone [17, 18]. A systematic review explained the deep cervical flexor (DCF) muscle training in CNP proving specific low-load craniocervical flexion exercise as a highly effective compared to other types of exercises [19]. The various rehabilitation techniques for chronic low back pain (CLBP) are manual therapy including thrust manipulation and non-thrust mobilisation procedures, trunk coordination, strengthening and endurance exercise, centralisation and directional preference exercises. Nerve mobilisation and progressive walking have been recommended for older individuals. Fitness activities, progressive endurance exercises, counselling and patient education, lower-quarter nerve mobilisation procedures, traction, and proprioceptive neuromuscular facilitation (PNF) techniques are the other treatment ideas recommended for the joint mobility, movement fault and muscle strength [20].
PNF is a neurophysiological approach working on a similar criterion of relative muscle stiffness and weakness. PNF techniques emphasise muscle strength, flexibility, and balance by stimulating proprioceptors within the muscles and tendons. The PNF treatment is believed to induce similar therapeutic effects of strengthening, conditioning and endurance among individuals with chronic mechanical muscular dysfunction regimes. Additionally, PNF facilitates maximum motor unit response by enhancing coordination ability in response to neuromuscular stimuli [21]. However, few randomised controlled trials were conducted on PNF comparing it to the conventional physiotherapy treatments or any other experimental techniques to treat pain and disability in chronic low back pain [22–29]. They have selected PNF techniques’ patterns depending on their justification of the cause of the pain and disability. Nevertheless, the extend at which PNF benefits chronic back and neck pain and disability is not clearly understood.
This systematic review aimed to study the effects of PNF on pain management and disability in individuals with chronic back and neck pain conditions compared to other treatments. We examined the randomised controlled trials of PNF as an intervention in CLBP and CNP through a systematic literature search using the appropriate keywords.
Methods
The protocol has been registered a priori with the PROSPERO database (CRD42020165012). We followed PRISMA recommendations (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to conduct and report this systematic review.
Search strategy
A literature search was structured and conducted through the electronic databases of search in PubMed, Scopus, Cochrane, Wiley and Ovid for published articles until 2019. An updated search was conducted until 2021 to observe if there have been any other potential articles.
We performed a systematic search strategy using relevant keywords with appropriate Boolean operators to identify the papers on chronic low back pain, chronic neck pain and proprioceptive neuromuscular facilitation. The keywords used were “chronic low back pain ”OR “CLBP” OR “mechanical low back pain” OR “non-specific low back pain” OR “aspecific back pain” OR “chronic neck pain” OR “CNP” OR “mechanical neck pain” OR “non-specific neck pain” OR “aspecific neck pain” AND “proprioceptive neuromuscular facilitation” OR “PNF” OR “rhythmic initiation” OR “combination of isotonic” OR “rhythmic stabilisation “OR “dynamic reversals” OR” neuromuscular facilitation” OR “reflex excitability” OR “hold-relax” OR “contract-relax” OR “repeated contraction” OR “stabilising reversal”.
Two independent reviewers conducted the search process for removal of duplicates, screening of titles and abstracts before considering the full-text articles. The consensus was reached in case of disagreements through the third reviewer.
Eligibility criteria for screening studies
Articles included were the standard randomised controlled trials having the titles and keywords confined to “proprioceptive neuromuscular facilitation” and “chronic low back pain” or “proprioceptive neuromuscular facilitation” and “chronic neck pain". The inclusion criteria of this review were: Adult men and women participants; PNF as an independent intervention for back pain or neck pain; low back pain or neck pain presenting chronic symptoms beyond three months; papers published only in English; and measurable outcomes to evaluate the effect of treatment. For this review, articles were excluded if they were non-experimental, case studies, quasi-experimental, non-standard randomised controlled trials, or uncontrolled design.
Study selection process
The electronic search for the articles was performed using the data mentioned above until December 2019 and then an updated search for last two years 2020-21. The duplicates were removed through EndNote (version 7) and a manual search by the first reviewer. Non-relevant articles were removed after the duplicate removal. The abstracts and full-text articles were screened for further relevance and eligibility, among which only nine studies met the inclusion criteria for this systematic review. The articles focusing on PNF as an intervention for treating CLBP or CNP were further analysed(Fig. 1).
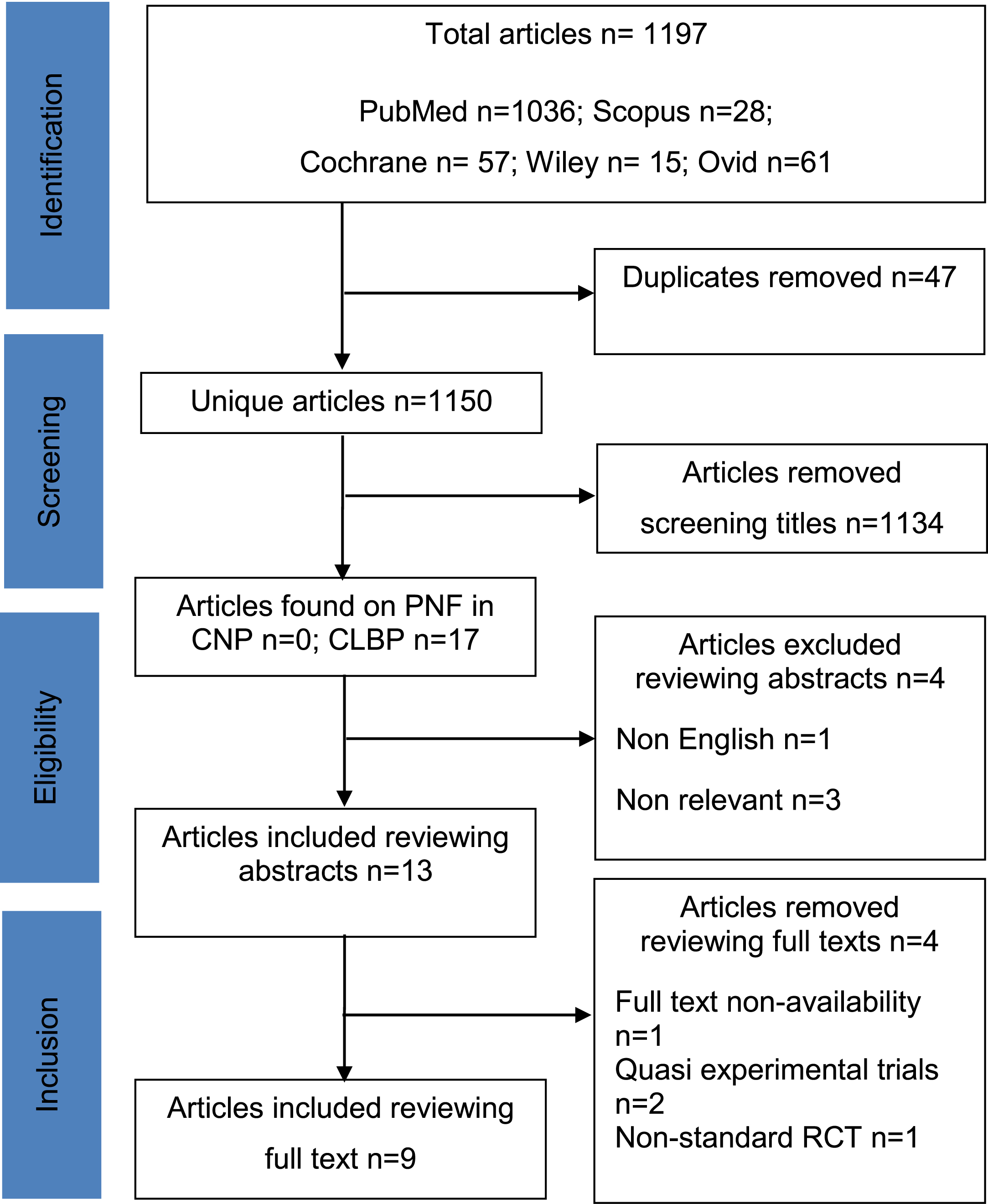
Review articles selection flow diagram.
Methodological quality check for each included study was done by two reviewers and cross-verified by the third reviewer. Joanna Briggs Institute (JBI) critical appraisal tool was used for the quality assessment for minimising the bias of studies [31]. It has 13 questions for the quality check. The scores were moderate to high ranging from 6/13 to 11/13. Five of the eight studies were assessor-blinded. Two studies had no form of blinding, and none of the included studies was triple-blinded.
Data synthesis
With sufficient homogeneity of the outcome measures in at least three articles, we conducted a meta-analysis of pooled mean differences of Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) comparing the PNF with other treatment using a random-effects model. The statistical heterogeneity among the studies was assessed by Chi2 and I2. Statistical significance was considered with a two-sided p < 0.05. RevMan 5.0 was used to perform the analysis.
Results
Search results and characteristics of included studies
Of 1197 articles were yielded at the initial search, 1150 articles remained after removal of duplicates. We removed 1134 articles after screening the titles. Seventeen articles were found on PNF treating CLBP, and none for PNF treating CNP. Four articles were removed after reviewing abstracts, among which one was a non-English article and three were not relevant. Among the remaining 13 articles, four were removed after reviewing the full text of the articles. One article due to non-availability of the full text, two were quasi-experimental trials, and another paper was not an RCT study. Finally, nine eligible articles were included in this review.
Participants
This review analysed nine relevant studies having a total of 416 participants. The mean sample size was 46, ranging from 12 to 108 participants. All the studies included both men and women participants except for two studies conducted by Kofotolis and colleagues [22, 23]. Young et al. [29] had only elderly participants in their study.
Interventions used in the included studies
Five studies [22–26] compared the various PNF treatment techniques with the conventional physiotherapy techniques such as general trunk exercises, educational booklets and numerous other electrotherapy agents. In contrast, the rest of the four PNF studies [27–30] compared to neuromuscular joint facilitation, gym ball exercises and core stabilisation exercises (Table 2). Each study mostly used more than one technique of PNF in combination. Five studies [22, 30] used rhythmic stabilisation, five studies [22–24, 30] used a combination of isotonics, two studies of Areeudomwong [26, 30] used chop and lift. Kim et al. [25] applied rhythmic initiation and stabilising reversals in their study. Besides, Lee [28], Young [29], and Huang [27] and their colleagues used the sprinter and skater patterns techniques, PNF integration pattern, and front inferior pelvic pattern, respectively. The mean duration of intervention was 4.5 weeks and ranged 3–6 weeks. None of the studies had a follow-up except for Areeudomwong et al. [24] who conducted 12-weeks follow up.
PNF studies characteristics
PNF studies characteristics
PNF = Proprioceptive Neuromuscular Facilitation; RST = Rhythmic Stabilization; COI- Combination Of Isotonic; TENS = Transcutaneous Electrical Nerve Stimulation; CL = Chop and lift; VAS = Visual Analogue Scale; ODI = Oswestry Disability Index; NRS = Numerical Rating Scale for pain; RMDQ = Roland Morris Disability Questionnaire; HRQL- PCS = Health Related Quality of Life- Physical Component Summary; HRQOL-MCS = Health Related Quality of Life- Mental Component Summary; GPES = Global Perceived Effect Scale; EMG = Electromyography; OLST = One Legged Standing Test; LES = Lumbar Erector Spinae; TUG = Timed Up and Go.
Pain
The pain outcome was mainly measured through VAS and NRS. Four studies [25, 27–29] used VAS and showed a statistical improvement (Fig. 2a) of pain after the PNF intervention. The scores ranged from 0.7 to 4.2 points on the scale. Kim et al. [25] showed the most significant improvement. Areeudomwong in all three PNF studies [24, 30] used NRS to measure pain and showed a considerable change score of 2.33 to 2.54 points (Fig. 2b). Kofotolis and colleagues [22] observed 1.1 points change in Borg back pain intensity scale and 0.7 point change in back pain severity in their yet another PNF study [23].

Forest plot after meta-analysis. 2a. Visual Analog Scale.

Numerical Rating Scale.
The functional disability was mostly measured by the Oswestry Disability Index (ODI) and the Roland–Morris Disability Questionnaire (RMDQ). The ODI was used in three studies [22, 25], and the improvements ranged from 7.1–12 points. Kim et al. [25] showed a more significant change of 12 points in ODI post-PNF treatment (Fig. 2c). Three studies [24, 30] measured RMDQ with a mean difference of 2.27–4.23 points, Areeudomwong et al. [26] demonstrated the most substantial improvement of 4.23 points following PNF treatment (Fig. 2d). The physical component summary of health-related quality of life (SF-37v2) alone showed a significant change of 9.75 points in the disability, but not in the mental component among the population with CLBP [24].

Oswestry Disability Index.

Roland Morris disability questionnaire (RMDQ).
The sagittal planar mobility of lumbar range of movement was measured in two studies by Kofotolis et al. [22, 23]. The lumbar flexion and extension range increased by 7.1–13.5 degrees, and 5–5.5 degrees, respectively after four weeks of PNF intervention in individuals with CLBP [23]. Besides pain and disability, there were other outcome measures also used in different PNF studies. Lee et al. [28] analysed the electromyography activity of transversus abdominis and erector spinae muscles with PNF training, and they observed a change of 8.2% and 6.04% in maximum voluntary isometric contraction. Two other PNF studies [24, 30] used patient satisfaction scale and marked a change score of 0.69 (0.20–1.89) points in the afore-mentioned measure. Areedomwong found improvement by 8.54 (4.73–12.35) points in the physical component of health-related quality of life. Kim et al. [25] measured the lung capacity and showed a change of 0.64 (0.21–0.97) points in FEV1 after 6-weeks PNF intervention.
Two studies [26, 29] measured balance capacity. Areedomwong [26] studied single leg standing on a platform and showed an ellipse-sway area during eyes-opened [129.09 (64.93–175.25) mm2 ] and eyes-closed [336.27 (109.67–562.87) mm2] sensory conditions. The centre of pressure velocity during eye opened and eye closed conditions changed 6.68 (4.41–8.95) mm/s and 6.77 (4.01–9.54) mm/s, respectively. Young et al. [29] showed a change score of 1.79 centimetres measured using functional reach test following 6-weeks PNF intervention. Huang et al. [27] measured the benefits of 4-weeks PNF regime on the cross-sectional area of trunk muscles, and the thickness of multifidus and transversus abdominis increased by 0.2 cm2 and 0.02cm2, respectively. Those who underwent PNF training showed a quickness of walking ability (8.89 seconds) in the timed up and go test [29]. Table 3 shows the within-group change of PNF intervention across many studies. We did not perform pooled analysis for these outcome measurements due to the heterogeneity group. The outcome measures within and between groups changed significantly with PNF intervention except for the study by Huang et al. [27] who showed substantial benefits with neuromuscular joint facilitation.
Comparison of outcome measures within and between groups
Comparison of outcome measures within and between groups
FEV1 = Forced expiratory volume in first second; CoP = Centre of pressure; MVIC = Maximal voluntary isometric contraction; NSEO = Normal standing eyes opened; NSEC Normal standing eyes closed; SSEO = Semi-tandem standing eyes opened; SSEC = Semi-tandem standing eyes closed; HRQOL - PCS = Health Related Quality Of Life Physical Component Summary; HRQOL - MCS = Health Related Quality Of Life Mental Component Summary; OLST –EO = One-legged stand test with eyes opened; OLST –EC = One-legged stand test with eyes-closed; FRT = Functional reach test; TUG = Timed up and go test. *p < 0.05 = statistically significant within group; ** statistically significant between groups; ***p < 0.001 = highly statistical significance; NS- Not significant; a, b, c & d = statistically significant from G1, G2; G3 and G4, respectively; and e = statistical significance at follow-up.
Main results
This review aimed to examine PNF evidence as an intervention to treat chronic back and neck pain. The primary observation was that all retrieved nine papers studied the benefits of PNF in CLBP. Secondly, no PNF studies were found among individuals with CNP. Although many authors measured different outcomes using various PNF techniques among people with CLBP, majority of them brought about significant change in pain and disability. The authors supported their view about PNF philosophy and its possible pain relief mechanism and function in individuals with CLBP.
PNF techniques in CLBP
The Kirkaldy-Willis degenerative cascade explains the abnormal movements causing damage due to reduced endurance, flexibility, increased fatigue and insufficient strength, abnormal neural control caused by the movement pattern in mechanical low back pain [32]. The combination of isotonic was applied for motor learning, increasing muscle strength and intra-inter muscular coordination in many studies. The combination of isotonic is an agonist technique in which the pattern is performed in a combination of concentric, eccentric and static contractions without losing the muscle tension. Kofotolis et al. [22] stated that the combination of isotonic technique initiates the body reflexes to relax the muscle and increases flexibility. The use of all the types of muscle contractions, including isometric, eccentric and concentric muscular work shall result in better lumbar mobility and muscular endurance. The timing of isotonic contraction and elongation of the lumbar erector spinae muscle emphasises the irradiation from the strong muscles synergy [24].
On the other hand, the rhythmical stabilisation techniques utilise a static nature of isometric contraction, both agonist and antagonist groups that initiate and learn a coordinated movement along with dynamic stability of spinal segments [22–24]. The sustained isometric contraction using rhythmical stabilisation technique promotes muscular coactivity and active static stability of the spine. However, the rhythmical stabilisation was also conditional for improving the sagittal planar lumbar mobility for those who were reluctant in performing dynamic exercises. The reciprocal innervation and inhibition and successive induction might be the possible explanations for muscle relaxation and increased muscles flexibility utilising the basic principles and procedures of PNF [33]. The muscle relaxation further gives rise to a greater stretch magnitude during training, sequentially superior flexibility gains. Additionally, it enhances muscle endurance involving muscular work at significantly progressing intensity levels after adjusting to individual patient performance [23].
PNF on pain in CLBP
The weakness of anterior abdominal muscles produces disuse atrophy in lumbar pain. It also increases the anterior pelvic tilt, and lumbar lordosis for those suffering from LBP [34, 35], warranting muscular strengthening [25]. The trunk chop and lift techniques are coupled movement of trunk lateral flexion and rotation to the same side, which might reinforce the weaker trunk muscles through irradiation of strong trunk and extremities [36]. The abdominal muscles’ contraction, particularly the deep-seated internal oblique, transversus abdominis, paraspinal and multifidus through their thoracolumbar myofascial connections, shall increase the intra-abdominal pressure by discharging the air to outside of the diaphragm, which is required for bucking for airway clearance [37]. The transversus abdominis and multifidi muscles are the postural set responsible for lumbar stability as they are the first ones to contract before the limb initiated movements [38]. As the trunk stability improved by PNF regime through the active contraction of anterior abdominals and better strength, the individuals with CLBP experience reduced pain and absence of back pain recurrence [25]. Areeudomwong summed up the chopping and lifting techniques along with rhythmical stabilisation and combination of isotonic for better muscle co-contraction, dynamic stability, and mobilisation of the vertebral column [33, 39]. Better activation of the trunk muscles is critical for lumbar stabilisation, helping pain management and participation in daily activities [24, 26]. Furthermore, improved balance capacity with PNF is believed to improve motor control of the transversus abdominis and lumbar erector spinae [24, 36] and alleviate pain intensity [40].
PNF on pain, motor control and disability in CLBP
Majority of the PNF studies reflect on the theoretical philosophy and the physiological mechanisms to alleviate pain through autogenic inhibition, reciprocal inhibition, stress relaxation and gate control mechanism [33]. Poor trunk movement control of individuals with CLBP during the daily activities is due to the functionally impaired neuromuscular adjustments and absence of continuous feedback of trunk proprioception [50]. The impaired trunk proprioception and abnormal intersegmental hypermobility of the lumbar spine were explained by the notation that the lumbar spine is at higher risk of abnormal loading and nociceptive activation in the presence of weak core muscles and altered the sensory-motor control mechanisms [42–44]. The pain provocation might further worsen the proprioception of the spine [45, 46]. There is a positive correlation between lumbar proprioception and VAS in people with CLBP [47, 48]. Such a vicious cycle between pain and motor control has been suggested to contribute to low back pain [49–51]. The unresolved proprioceptive impairments of prior episodes are the potential causes of recurrence and chronicity of low back pain, thus reducing the ability to maintain a neutral posture and intra and inter muscular incoordination. This subsequently gives away the spinal control and adds up with stresses and strains on the spine prolonging the pain state, leading to further loss of proprioception [53–56]. Areeudomwong et al. [30] believed that the core strengthening exercise brings about the neuromuscular system’s restoration. The coactivity of lumbar muscles with rhythmical stabilisation and dynamic nature of the combination of isotonic shall explain for trunk stabilisation. Subsequently, it results in increased activation of deep trunk muscles leading to injury prevention and pain relief. Lee et al. [28] introduced the sprinter and skater patterns of PNF for individuals suffering from CLBP based on an imbalance between stability and mobility of muscles, along with the length changes [41]. They supported their view by stating that the benefits were not only because of the muscle strengthening with large-scale movement, but also the functional training effects on active motor control, intra and intermuscular coordination, active range of motion, and efficient motor control [29].
Strength and limitations
There is reliable information to use PNF techniques, mainly the combination of isotonic and rhythmical stabilisation as a treatment option in CLBP. The dynamic reversal, a strengthening technique of agonist and the antagonist groups might be useful following a combination of isotonic in CLBP, but not incorporated in any of the included studies [52]. Rhythmic initiation is an agonist technique aimed at muscle activity and motor control initially assisted by the therapist followed by active-assisted, resisted and active movement of the patient throughout the joint range of motion. The stabilising reversal is a technique in which isometric contraction of agonist and antagonist occurs without relaxation; thus the steadiness of desired positions is encouraged. Rhythmic initiation and stabilising reversals techniques were not majorly administered in all studies except one [25]. Despite the anatomical and pathomechanics characteristics of the lumbar and cervical spine being similar in many ways; the published PNF studied had no emphasis on pain and disability among people with CNP. The muscular strength and endurance of deep cervical flexors dynamically support and orient the head in space and modulates the muscle forces between head-neck and trunk [57]. A systematic review of the properties of deep cervical flexor muscles in individuals with CNP reported a reduction in their muscle strength, endurance, activation size and the presence of pain [58]. The cervical spine’s dynamic stability and the maintenance of lordosis posture are brought about by these muscles [59]. Any reflex-inhibition due to proprioceptive deficits, and relative weakness and stiffness of deep cervical flexors and upper cervical extensors, respectively might be the source for compensatory over-activity of superficial anterior scalene and sternocleidomastoid muscles leading to early fatigability and pain among people with non-specific neck pain [60]. As PNF techniques have proven to be effective in pain management and function of individuals with CLBP by improving the strength and motor control of abdominal muscles, the techniques of combination of isotonic and rhythmical stabilisation might also be useful in enhancing the motor control and strength of deep cervical flexors among people with CNP. Future PNF studies in CNP might confirm this notation.
Conclusion
Implications for practice
The basic principles and procedures of PNF and its techniques adopt the above-mentioned theoretical facts. The participating individuals with CLBP might have benefited from pain intensity and overcoming the disability. Therefore, the PNF training could help decrease pain and increase the functionality of people with CLBP.
Implications for research
The PNF papers included in this review demonstrated significant positive changes in pain and disability compared to other rehabilitation ideas. Considering the moderate to high-quality studies by the JBI scoring and meta-analysis, and the mean changes of outcome measures post-PNF training, this review recommends PNF training to alleviate pain and disability in CLBP. Future PNF trials might examine the real benefits of various techniques on pain and related outcomes in CLBP. Although PNF studies used many outcome measurements in people with CLBP, more robust measures are needed in future trials. Till date, there were no studies examined the benefits of PNF among people with CNP warranting appropriate treatment techniques in future trials.
Conflict of interest
There is nothing to declare as competing interest.