
Abstract
BACKGROUND:
Proprioception is the awareness of the position, movement, and muscular force generated by the body and its musculoskeletal parts, and is an important somatosensory impairment to assess in people with stroke. We know that rehabilitation clinicians self-report to assess proprioception in approximately two-thirds of people with stroke. What we do not know is what type of assessments are used, or the true frequency of their use in clinical practice. This study aimed to provide a preliminary description of the type and frequency of proprioception assessment used by clinicians working in stroke rehabilitation in Australia, and their knowledge about proprioception impairment.
METHODS:
We surveyed Australian physiotherapists and occupational therapists who were involved in the rehabilitation of people with stroke. The online cross-sectional survey ran from March to October 2020. While they were blind to the aims of the study, respondents answered questions about clinical decision-making in a case study of a person with stroke and proprioception impairment. Then, they were asked questions about proprioception.
RESULTS:
There was a total of 165 survey responses, of which 58 contained complete datasets suitable for analysis. Only 55% (n = 32) of respondents selected an assessment of proprioception for the person described in the case study. The majority of respondents defined proprioception to be the sense of joint / limb (n = 38, 65.5%) or body (n = 27, 46.6%) position and used ‘eyeball’ judgements of limb matching accuracy (56%, n = 33) as an assessment.
CONCLUSIONS:
These preliminary data suggest that proprioception is likely under-assessed in stroke rehabilitation and that clinicians understand proprioception to be the sense of joint position and movement, but lack awareness of other proprioceptive senses, such as the sense of muscle force. These factors may reduce the ability of clinicians to rehabilitate proprioception impairment in people with stroke.
Introduction
Knowing where your limbs are in space is important for most people, but it is especially important for people who undergo rehabilitation after a stroke [1]. Knowledge of limb position occurs through proprioception, a set of somatosensory processes that also allow judgement and representation of muscle force, body movement, and body shape [2, 3]. Proprioception is critical to learn, plan, execute, and correct motor actions; when people lose proprioception, such as in cases of loss of all activity in large-diameter afferents, they are effectively paralyzed [4]. Approximately half of all stroke-survivors have impaired proprioception [1], and it is therefore important to consider proprioception in stroke rehabilitation. Unsurprisingly, impairment in proprioception is associated with poor recovery of upper and lower limb motor function [5, 6], and reduced independence in activities of daily living after stroke [7].
Proprioception has multiple component parts, and so a comprehensive assessment of proprioception impairment should ideally assess each of them. Such an assessment would include tests of the senses of position and movement [8], the sense of muscular force [9–11], and of the body model to which they contribute [12, 13]. Additionally, it is increasingly clear that there are two distinct forms of proprioception: low-level and high-level [14]. Tests of low-level proprioception require people to detect, discriminate between, or match proprioceptive signals; for example, “Bend your left elbow to match the angle of your hidden right elbow.” Conversely, tests of high-level proprioception assess higher brain functions that integrate proprioceptive signals into other reference frames. These judgements are important to everyday function, for example, we must know “where is the tip of my index finger in visual space?” when we reach for an object.
However, published assessments of proprioception for people with neurological conditions are time-consuming to use, and limited to low-level tasks such as movement direction or position matching [15]. These formal assessments also typically grade a person’s proprioception as normal, impaired, or absent which means they cannot track more subtle changes in impairment severity over time [16, 17]. These limitations may explain the decision of 70% of Australian physiotherapists and occupational therapists not to use published, standardised sensorimotor assessment tools with people with stroke [18].
In the stroke rehabilitation multidisciplinary team [19], physiotherapists and occupational therapists typically assess and manage impaired proprioception. While we know that a large percentage of these clinicians use an informal limb-matching or movement detection task to assess proprioception, we do not know precisely how they implement these assessments. Additionally, we know that when surveyed, clinicians indicate they assess proprioception in approximately two-thirds of people with stroke. However, self-reported measures are biased and may not accurately reflect current clinical practice [20]. An alternative way to investigate clinical practice is through case vignettes, which ask clinicians to describe the actions they would take in response to a short description of a clinical scenario [21–23].
This study aimed to clarify the frequency and type of proprioception assessment in stroke rehabilitation, and surveyed Australian rehabilitation physiotherapy and occupational therapy clinicians. We first asked participants clinical-reasoning questions based on a case vignette of a person with stroke and proprioception impairment. Clinicians answered these questions while they were unaware of the specific aims of the study. The, we asked clinicians to describe their knowledge of and attitudes to proprioception assessment.
Methods
Design
A cross-sectional design using an online survey.
Population
Clinicians were eligible to complete the survey if they a) were an Australian Health Practitioner Registration Agency registered physiotherapist or occupational therapist, b) had been working for at least 6 months in the past year in a rehabilitation setting, c) had a minimum of three months experience working with people with stroke, and d) were not currently participating in the development of clinical guidelines for stroke.
Survey structure
The survey was open from March to October 2020 and had three sections with different question types (Appendix A): Basic clinician demographic information (multiple choice). Case vignette interpretation, including questions about impairments and assessment choices in a case study of a person with stroke (open-ended). Questions about knowledge and attitudes to proprioception (visual analogue scales and open-ended).
The research team created two case vignettes (Appendix B) that described a typical person with stroke in both inpatient and community settings as a proxy for clinical practice [21–23]. The survey title was generic to stroke rehabilitation, which kept respondents unaware that the study specifically aimed to investigate proprioception until they had completed the case vignette questions. Respondents could not return to change their answers to the vignette questions after they moved on to the questions about proprioception. The maximum possible value for all visual analogue scales was 10 except for the percentage of people with stroke that clinicians estimated to assess for proprioception impairment, which was 100.
Survey development
Demographic questions were based on those included in a Canadian National Survey of stroke clinicians [21]. Three cues that described a proprioceptive impairment were developed by the research team and inserted into each case vignette. These cues included “when sitting, he often has difficulty finding the (L) arm rest to guide himself down” (inpatient) and “she has trouble finding her dentures on her bedside table before her husband turns on the light” (community). To ensure that strength impairment was not the primary explanation for these deficits, both case vignettes described people with all muscle groups at a minimum of 3/5 on manual muscle test, which meant that they were able to actively move their limbs through a full range of motion against gravity. Three physiotherapists and two occupational therapists with clinical experience that ranged from less than one year to greater than ten years were consulted to ensure the cues actually indicated a proprioception impairment and the vignettes were easy to read.
Survey questions were developed first in consultation with a study author with subject matter expertise (SG), and then with a variety of clinicians that worked in stroke rehabilitation. The full survey was piloted on a sample of four clinicians (two physiotherapists and two occupational therapists) to check that questions were clear and to determine how long the survey took to complete. These four clinicians participated in a focus group facilitated by author GF, who checked their understanding of the survey questions and gave opportunity for feedback. The clinicians agreed that the survey could be completed in approximately 20 minutes. However, they recommended ensuring that participants could save and return to complete the survey, which would allow intermittent completion throughout a clinical workday. Based on this and other recommendations of the focus group, the research team revised the survey into its final online form. The final survey was made available to clinicians using the Qualtrics software platform [24].
Participant recruitment
For the survey pilot, clinicians were recruited from the professional networks of the research team. For the survey proper, clinicians were recruited via advertisement through the mailing lists and social media pages of PT, OT, and stroke organizations in Australia. In addition, the survey link was distributed to the physiotherapy and occupational therapy department heads of Australian hospitals with a dedicated rehabilitation unit. Participants were eligible to win one of four $25 gift cards as an incentive to answer the survey. The study was approved by the University of Technology Low Risk Research Ethics Committee, approval no. UTS-ETH19-4402 and UTS-ETH20-4768.
Data and statistical analysis
Sample size
There was no sample size calculation as the study aim did not include hypothesis testing. The research team contacted the Australian Physiotherapy Association, Australian Occupational Therapy Association, and the Australian Health Practitioner Regulation Agency to attempt to obtain an estimate of the number of clinicians working in rehabilitation settings with people with stroke or neurological conditions in Australia. Each of these organisations indicated that they do not collect such data.
Qualitative survey data analysis
A framework analysis methodology [25] was used to evaluate the survey open ended questions using NVivo software [26]. The research team developed a coding framework (Appendix C) a priori in consultation with subject matter experts and using reviews of proprioception [2, 8]. The final framework had scope for novel codes where data did not fit the pre-determined codes for each question. Two members of the research team (GF, DK) independently extracted and coded the data from each survey via the process of analysis set out by Gale, Heath et al. [25]. Disagreements were resolved through discussion. Raw counts of the frequency of each code were calculated and illustrative quotes extracted for each question.
The final coding framework had sub-frameworks for each open-ended question. Codes for participant definitions of proprioception had sub-frameworks for sensory processes (e.g., sense of position, sense of movement), anatomical structures (e.g., muscle spindle, skin receptors), and neurophysiological processes (e.g., spatial integration). The codes for questions about proprioception assessment tools had sub-frameworks for assessments that were deemed specific to proprioception (e.g., signal detection, signal matching, and localisation of body parts) and for assessments that were non-specific (e.g., balance, co-ordination, observation of functional tasks). The codes for questions about position-sense assessment technique had sub-frameworks for the level of motor involvement in the reference and indicator limb, the measurement method (e.g., goniometer, eyeball), and if there was unilateral or bilateral limb involvement.
Quantitative survey data analysis
Raw counts of each category in the demographic questions were calculated. Normality tests were conducted for each quantitative survey question using the SciPy module in Python software [27]. Where data were normally distributed, we calculated means and standard deviations. Where they were not, we calculated medians and interquartile ranges. Finally, we calculated 95% confidence intervals for each question.
Results
Clinician characteristics
A total of 165 surveys responses were registered, of which 58 contained complete datasets suitable for analysis. There were missing data from one participant in two questions of the survey that are noted in the tables throughout. The average time taken to complete the survey was 1 hour and 40 minutes (SD 4 hours and 30 minutes), likely reflecting sporadic completion over a clinical day. Table 1 illustrates the characteristics of the 43 physiotherapists and 15 occupational therapists who responded to the survey completely.
Demographic characteristics of survey respondents
Demographic characteristics of survey respondents
The survey asked clinicians to list the components of their initial and subsequent clinical assessments of the person described in the case vignette. In their initial clinical assessment, 55% (n = 32) of survey respondents chose to assess proprioception. However, only 36% (n = 21) of respondents selected a tool that was specific to proprioception. In their subsequent clinical assessment, an additional 17% (n = 10) of respondents chose to assess proprioception. Only half of these additional participants (n = 5) selected an assessment tool specific to proprioception. Thus, a total of 44% (n = 26) of survey respondents correctly identified proprioception as an impairment in the case study and suggested a tool that was able to specifically evaluate proprioception in their initial or subsequent clinical assessment of the person in the vignette.
Proprioception knowledge and assessment (open-ended questions)
Survey respondents predominately understood proprioception to be the sense of joint / limb (65%, n = 38) or body (46%, n = 27) position, e.g. “The way I explain it (proprioception) to patients is the ability to know where your body is in space without looking at it”. When asked to describe a complete proprioception assessment, respondents described limb position matching (56%, n = 33), passive movement direction judgement (44%, n = 26), or passive movement detection (17%, n = 10), e.g. “(I assess the) ability to detect position/movement at joints”. However, 48% (n = 32) of respondents also identified methods that were not specific to proprioception as part of a complete proprioception assessment. The most common of these were observation of patient performance (43%, n = 25), typically during tests of coordination (e.g., finger to nose) or functional tasks (e.g., gait analysis). Only four respondents (7%) identified a published assessment as a component of a complete proprioception assessment.
In the survey, clinicians were asked to describe the assessments of proprioception that they used in their day-to-day clinical practice (Table 2). Most respondents described either a verbal judgement of the direction of passive movement (40%, n = 23) for example, “(I would) flex or extend a joint e.g. thumb . . . and see if the patient can tell me which direction (it moved)”, or a limb position-matching task (53%, n = 31). The majority of respondents performed matching tasks that used two limbs (67%, n = 39), for example, “the therapist moves affected limb into position, (and) patient replicates with unaffected limb”. Only 9% (n = 5) of respondents reported use of a standardised measurement of position matching, with the remainder either reporting ‘eyeballing’ of the match (47%, n = 27) or an unclear method of measurement (28%, n = 16). More than half of respondents also reported use of a non-specific assessment of proprioception in their clinical practice (55%, n = 32), again predominately observation of functional or coordination tasks (45%, n = 26), “I watch the client’s quality of movement, to check if needing to assess (proprioception) further”. A report of the full counts of respondent numbers per code is in Supplementary Data 1.
Proprioception assessment in respondent clinical practice codebook and frequencies. Multiple answers were permitted, so that combined totals do not equal the number of study participants
Proprioception assessment in respondent clinical practice codebook and frequencies. Multiple answers were permitted, so that combined totals do not equal the number of study participants
All VAS question data were normally distributed. Two data points were missing in the question pertaining to clinician confidence in treating proprioception. On a scale from ‘Not at all confident (0)’ to ‘Completely confident (10)’, clinicians rated themselves as a mean of 7.5 (SD 2.5, 95% CI 6.83–8.16) in assessing proprioception and 5.6 (SD 2.1, 95% CI 5.1–6.2) for treating proprioception (Fig. 1). Clinicians rated the importance of proprioception assessment in people with stroke as a mean of 8.1 (SD 1.8, 95% CI 7.6–8.5) on a scale from ‘Not important at all (0)’ to ‘Extremely important (10)’. Finally, clinicians reported routinely assessing proprioception in an average of 64.2% of the people with stroke that they work with (SD 29.8%, 95% CI 56.3–72.1%).
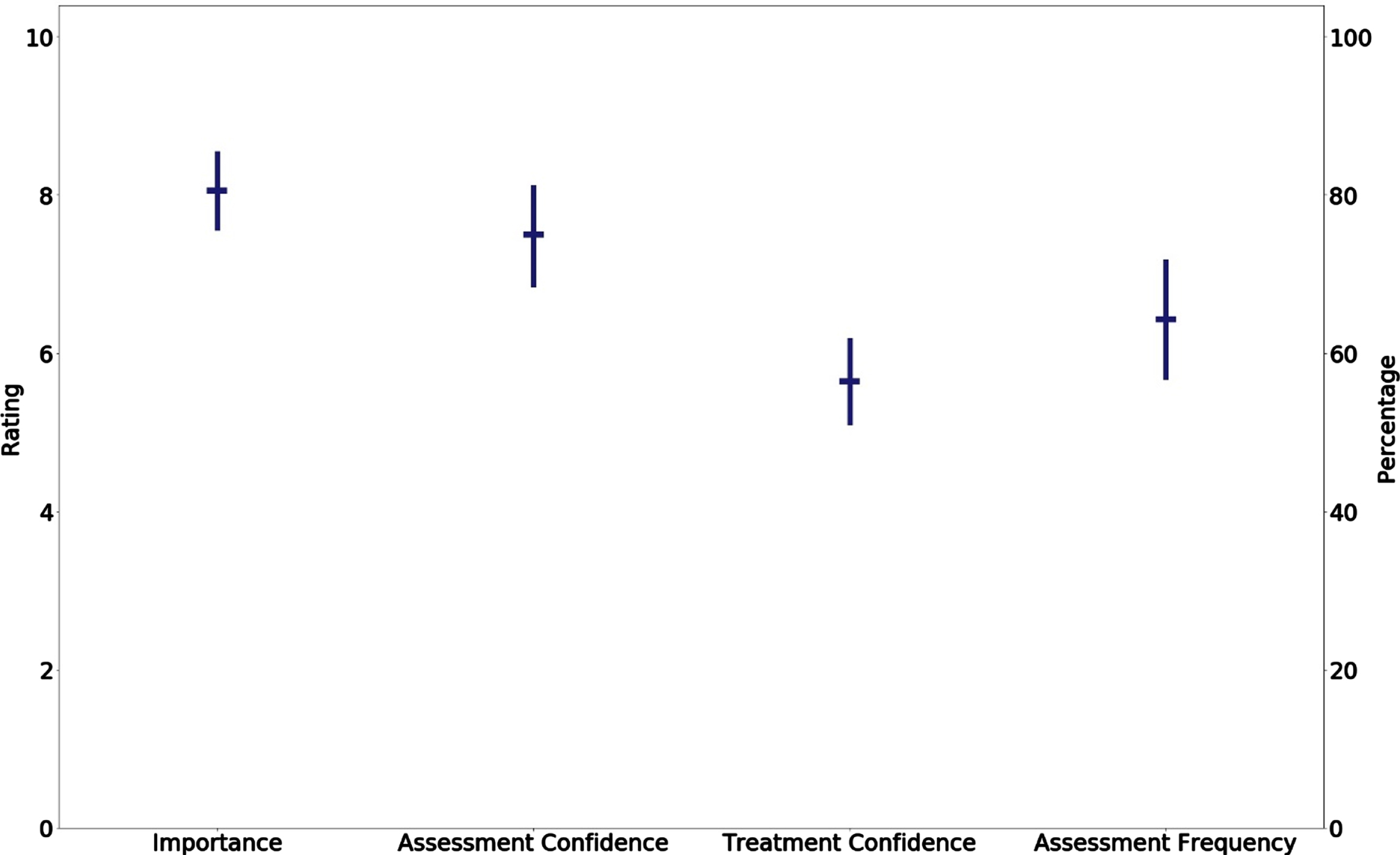
Means and 95% confidence intervals of clinician self-rating for VAS questions. Assessment frequency was rated as a percentage of total assessments, while all other questions were a self-rating out of 10.
In neurorehabilitation, stroke survivors must relearn how to plan, execute, and correct motor actions. Proprioception is needed for each of these processes [2], and it is therefore important to assess proprioception in stroke rehabilitation. To our knowledge, this is the first study to examine both if and how proprioception assessment occurred in clinical stroke rehabilitation using a clinical case where clinicians were unaware of the research aims. Clinician answers to questions asked using this method are likely to more closely reflect their actual clinical decision-making [23]. Respondents in the present study estimated that they assessed people with stroke for proprioception impairment 64% of the time. However, only 55% of respondents identified that the person in the case vignette needed an assessment of proprioception. The low rate of proprioception assessment is unlikely to be due to low awareness of proprioception, as survey respondents had a basic knowledge of proprioception and its assessment. It is also unlikely that proprioception assessment was not perceived as a priority; respondents rated proprioception assessment as highly important in stroke assessment and treatment.
Instead, other factors likely contribute to low frequency of proprioception assessment in people with stroke. Formal assessments of proprioception are typically part of sensorimotor assessment batteries [16, 17] that are time consuming to administer, which is a barrier to their clinical use. Assessment of proprioception is also more difficult in stroke-survivors with more complex clinical presentations, for example those with unilateral neglect, aphasia, or cognitive impairment. Additionally, unlike vision or hearing, proprioception does not have an obvious receptor. That is, while people can clearly perceive a post-stroke hearing impairment, it is harder to ‘feel’ a change in proprioception ability. Thus, proprioception impairment is likely also less apparent to people with stroke. Future work should aim to educate clinicians and stroke-survivors about proprioception impairment and its clinical presentation.
In our survey, clinicians understood proprioception as the sense of limb position or movement, but not as the sense of muscle force or of weight, or to include high-level proprioceptive judgements. This knowledge gap may be in part due to the fact that there are no conventional clinical assessments for the sense of force or weight for people with stroke, and no clinical assessments of high-level proprioception. The lack of assessment of the sense of force may also be due to the confounding influence of muscle weakness in people with stroke. However, assessment of the sense of force or weight is clinically suitable in certain subgroups, for example those with largely preserved strength but significant ataxia, or people in the chronic stages of stroke who have regained some degree of strength and function. Tests of these additional elements of proprioception are used in research studies [11, 28], and as such, the development of clinical versions, investigation of their clinical utility, and eventual translation into clinical practice are important areas for future research.
Similar to previous studies, no survey respondent reported use of a standardised proprioception assessment tool; for example, the Wrist Proprioception Test [29], or a test battery that includes proprioceptive item e.g., the Nottingham Sensory Assessment [16]. There are many barriers to the use of standardised assessment tools in clinical practice; they often require clinicians to source or purchase additional equipment [30], lack sensitivity to detect change in impairment magnitude over time, or are time consuming to use. Additionally, their reported correlation to functional outcomes varies widely between studies, and is low to moderate at best [1, 31]. This may be because standardised assessments of proprioception typically evaluate one joint at a time with tasks that measure simple movement detection or the ability to match proprioceptive signals. In functional movements, it is often more important to judge the configuration of an entire limb in space, rather than matching the position of one joint to another or detecting that a joint has moved.
The focus of evidence-based rehabilitation is to demonstrate quantitative improvement in impairment severity, and the impact of impairments on the functional outcome of a person with stroke [32]. As such, clinicians may perceive standardised assessments of proprioception as having limited use, and in their place may opt to use a simple screen for proprioceptive impairment (e.g., “did I move your thumb up or down?”), which is supported by our data. Importantly, screening assessments do not enable a therapist to evaluate the success of their therapy program in improving the proprioception of the person they are working with. To further quantify current clinical assessment of proprioception, clinicians could repeat their limb movement / matching assessment five times and then calculate a percentage correct score. However, given the limitations of current assessments, it is likely that development of new, functionally relevant, quantitative assessments of proprioception is needed.
A high percentage (55.2%, n = 32) of survey respondents reported use of non-specific assessments of proprioception, mostly the observation of functional tasks. This suggests that clinicians recognise the importance of proprioception to motor function in people with stroke. However, at present, there are no specific signs of proprioceptive impairment in functional task observation described in the literature. Instead, deficits in areas including coordination, motor planning, vision, and cognition can confound this form of assessment. Subsequently, functional task observation leaves assessment to clinical judgement alone. Experienced clinicians may hypothesise that proprioceptive impairment underpins the observed performance in functional tasks, but this is impossible to know without a test that is specific to proprioception. Future research should investigate functional assessment of proprioception to enable clinicians to assess the sense in a manner relevant to the rehabilitation outcome of the people with stroke that they work with. Functional assessments typically use familiar motor tasks, and may also make proprioception easier to assess in stroke-survivors with aphasia, or perceptual or cognitive impairments.
In our results, clinical proprioception assessment typically involved joint position matching or movement detection. These assessments measure movement detection or the ability to match signals that arise predominantly from the cutaneous receptors and the muscle spindle [2]. The amount and location of cutaneous feedback can alter the sense of joint position, and thus it is important to standardise clinician hand position in position matching or movement detection assessments [33]. Additionally, the contraction history of a muscle significantly alters the sensitivity of its spindles to stretch, a characteristic called muscle thixotropy [34]. A clinical example of this is where a person has contracted their biceps muscle (for example, during a biceps manual muscle test) prior to a position-match test where the elbow is passively extended. Here, the biceps muscle spindles are more sensitive to stretch, and the person detects a position change more quickly. The opposite is true for a biceps that has been passively shortened prior to elbow extension, where the spindles are less sensitive to stretch, and the person is slower to detect a position change. To standardise the effects of muscle thixotropy, clinicians can either ask a person with stroke to contract the muscles that will be lengthened in the position test [35], or perform a passive ‘waggle’, where the joint to be tested is alternately passively flexed and extended [36]. Importantly, no therapist in our sample reported the use of a control for cutaneous feedback or muscle thixotropy. As such, clinician education about the importance of standardising hand position and muscle contraction history is likely to be an important future goal of evidence translation in this area.
Limitations
Neither the Australian Health Practitioner Regulation Agency, the Australian Physiotherapy Association, nor Occupational Therapy Australia collect data on the specific practice area of their members. The number of therapists currently working with stroke clients and therefore eligible to participate could not be determined or formally contacted, which necessitated a convenience sample and precluded calculation of the survey return rate or any comparison between respondents and non-respondents.
Furthermore, the SARS-COV-2 pandemic occurred after two months of recruitment. The perceived importance of answering a survey while maintaining clinical loads in the face of high levels of uncertainty and policy change in this time would have been understandably low. As such, the study sample size was small and subject to respondent bias. The high attrition rate in the study could also have been due respondent completion of the survey in between clinical tasks, which the average time to complete the survey suggests. Returning sporadically to the survey over a day increases the risk of forgetting to complete it. The characteristics of clinicians that did have the time to complete the survey may have been different to those that did not. For example, more senior clinicians may not have had time to complete the survey due to their added responsibilities; their knowledge and assessment of proprioception would be different to junior clinicians.
Finally, while chosen to provide a more accurate description of clinical practice, the use of case-vignettes and open-ended questions may have contributed to the high survey attrition rate and brevity of responses. Future research using this method should consider question designs that do not bias participant answers but that also facilitate survey completion and answer depth.
Conclusion
Proprioception is likely under-assessed in clinical stroke rehabilitation. When it is assessed, methods are non-standardised, easily confounded, and fail to address all aspects of proprioception. Clinicians perceived proprioception assessment to be important; however, a complete clinical assessment of proprioception that is relevant to functional rehabilitation outcome is not available to them. Future research should focus on the development and translation into practice of clinical assessments of proprioception that consider the senses of force and limb position in peri-personal space and that can accurately quantify deficits. Improved clinical assessment of proprioception in people with stroke has the potential to improve rehabilitation outcomes and subsequently reduce the burden of disease in this population.
Conflict of interest
The authors declare no conflict of interest.
Funding
This study did not receive funding.
Supplementary material
The appendices are available in the electronic version of this article: https://dx.doi.org/10.3233/PPR-210597.