
Abstract
BACKGROUND & OBJECTIVE:
The treatment outcome is influenced by the relationship between health care providers and patients. So far, there is no validated tool/scale in Hindi which can be used in the Indian population to gather data on empathy and holistic care provided by the healthcare professionals during their consultation. The primary goal of the study is to translate and cross-culturally adapt the CARE scale to Hindi. Also, to determine its content validity and reliability so that further research can be done on the Hindi speaking Spinal Cord Injury population.
METHODS:
The study was conducted in three phases, namely Translation-Cultural Adaptation, Content Validity, & Reliability. The CARE measure was translated into Hindi and qualitative and quantitative content validation through the expert opinion and the content validity ratio (CVR) method was tested on a purposive sample of 30 spinal cord injury (SCI) individuals in two rehabilitation centres in New Delhi, India. Item analysis was conducted (on 50 SCI individuals) to determine internal consistency reliability.
RESULTS:
The Hindi CARE measure high has high internal consistency reliability (Cronbach’s alpha = 0.924). CVR and qualitative review done by the panels of experts validated the content of the CARE measure.
CONCLUSION:
The CARE measure- Hindi version is a validated and reliable tool to be used in Hindi speaking Spinal Cord Injury population context. Further work is required to establish test-retest reliability and studies on bigger sample size.
Introduction
Spinal cord injury (SCI) is an irreversible, life altering event in which patients’ takes years to recover. SCI persons tend to experience a higher prevalence of secondary conditions and multimorbities and it has a significant impact on a person’s quality of life [1]. However, SCI persons often use healthcare facilities more as compared to the people with other disabilities. In the recent years, the healthcare model has shifted more towards the Patient Centered Care (PCC) [2] which helps improving the quality of life of persons with such disabilities. Balint et al defined PCC is a another way of medical thinking where the patients examined by the healthcare providers as a whole person, and the diagnosis can be called as whole diagnosis [3]. Also, every patient should be considered “as a unique human being” in the process of Patient centered care [3]. People with disabilities (such as Spinal cord Injury) often use healthcare services as compared to the people without disabilities due to their secondary complications. Literature supported that the challenges among people with SCI is not uniform across the globe [4]. Therefore, challenges like limited access to the healthcare system, poor communication, indifferent treatment, accessibility, confidentiality issues, varied consultation fees, secondary complications (pressure sores, pain, respiratory-gastrointestinal-urological complications etc.) may diminish the quality and patient-centeredness of care [5, 6]. Further patients’ have experienced some form of stress, anxiety, loss of control due to their condition at various points of time in their lives. Researchers have worked hard to develop various scales/instruments such as Anxiety Depression Stress Scale (ADSS) which help to access anxiety, depression and stress at one time or another. The development of instruments which help accessing the present condition of the patients help the medical fraternity to work on the patient wellbeing rather than direct medicines [7].
Healthcare system should always revolve around patient centered approach, which helps understanding the patients “as a whole person” and it boosts the patient-healthcare provider relationship. Literature supported the fact that the quality of the relationship between health professionals and patients can affect the outcome of treatment. The relationship between the healthcare professional and patients has increased with the good care provided and it also helps in developing the confidence amongst the patients [8–11].
Mercer and his colleagues (2004) defined the empathy and Patient centered care (PCC) through “Consultation and relational empathy (CARE)” scale. It is a measure which is based on the comprehensive definition of Empathy, holistic care and patient centered care. This measure helps finding out the patients’ perspective toward his/her consultation with healthcare provider irrespective of their social class/socio-economic status. In clinical context, the Empathy is described (1) as wide range of emotions and experiences feel by the patients, (2) as an ability to understand and communicate patients’ perception and his/her emotional state based on visual and verbal signs [11, 12]. The scale is widely validated in both primary and secondary care i.e. Nursing, General practice, Sexual health, Spinal cord injury by healthcare professional. The scale has also been validated and reliable in languages other than English such as Japanese, Dutch, Swedish etc [13–15]. To study the patient centered care and relational empathy in Hindi speaking country like India, the scale needed to be cross-culturally adapted and validated. Hence, the purpose of this study is to translate and cross-culturally adapt the CARE measure scale to Hindi language. Also, to determine its content validity and reliability so that further research can be done on the Hindi speaking Spinal Cord Injury population.
Methods
Study participants were recruited from two rehabilitation centers at Vasant Kunj, Delhi. Participants visited the centers for their rehabilitation and general exercises after Spinal cord injury. A total of 150 SCI individuals were approached to be a part of this study. Only 80 participants agreed to participate in the study.
Inclusion and exclusion criteria
Participants older than 18 years of age and above with acquired Spinal cord injury (SCI) with at least one year post injury were taken in the study. The participants who were able to read, speak, understand Hindi were included in the study.
Participants who had not given consent, had co-morbidities like cognitive dysfunction and vulnerable participant groups were excluded as they cannot cooperate in study well.
Description of the CARE measure
The CARE measure was originally developed by Dr. Stewart Mercer et al. at the Departments of General Practice in Glasgow and Edinburgh University in 2004 [11]. The scale comprises 10 questions and each item uses a 5 point Likert Scale ranging from ‘poor’ to ‘excellent’ i.e. poor’ = 1, ‘fair’ = 2, ‘good’ = 3, ‘very good’ = 4, and ‘excellent’ = 5. It generates the values between 1 and 5. All ten items are then added, giving a maximum possible score of 50, and a minimum of 10. Up to two ‘Not Applicable’ responses or missing values are allowable, and are replaced with the average score for the remaining items. The responses with more than two missing values or ‘Not Applicable’ responses are removed from the analysis. Items of the scale are presented in Appendix II.
Translation, validation & internal consistency of the CARE measure in Hindi language
The study involved the translation, cultural adaptation of the English version of the CARE measure and also to investigate the content validity and reliability of the Hindi version of the same. All participants had given the written consent. A written approval was also taken from the original author to develop the scale into Hindi Language. The procedure of translation and cross-cultural adaptation was carried out following the guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures by Beaton DE et al. [16]
The study was divided into two phases (1) English to Hindi translation and the cultural adaptation of the scale; (2) to determine the content validity and reliability of the Hindi version of the scale.
Phase 1: Translation and cultural adaptation
The following are the five steps were performed in “Phase 1” Forward translation Synthesis of 2 translations Back translation Creation of pre-final version Test of pre-final version
Forward translation
This step was carried out by 2 bilingual and independent translators, who translated the CARE Measure from English into Hindi. One of the translators (T1) was known to the subject and the other (T2) was not.
Synthesis of translations (T1 & T2)
In this step, both the translations were read thoroughly by the third person who was known to the subject and good command on the language. A discussion was held amongst the third person and the translators (T1 and T2) to compare the 2 versions and analyze any ambiguous expressions. The aim of this step was to reach a consensus and a single version of the translated questionnaire.
Back-translation
In this step new bilingual translators were invited to back translate the questionnaire into English. The purpose of this step is to confirm whether the translated version represented the original version of the questionnaire.
Creation of the pre-final version (Expert committee review)
The fourth step was the formation of a committee of experts made up of methodologists, health professionals, language professionals, and the translators (forward and back translators). The original developers of the questionnaire were also a part of this review. The expert committee analyzed all versions of the questionnaire, discussed differences in translation, revised translations, back translation and then suggested the changes which help developed the final version of the questionnaire with appropriate cultural equivalence.
Test of the pre-final version
In this last step of the translational and cultural adaptation, the questionnaire was administered to 30 individuals with Spinal cord Injury (both traumatic and non-traumatic) with at least one year post injury.
Participants were asked about their understanding on the questionnaire (which called as cognitive debriefing) and any difficulties in completing the questionnaire. There were five questions (refer Table Appendix I) on each “Item” of the questionnaire which were asked to reach the consensus and participants’ understanding towards the concept of the questionnaire. This process also helps establishing the acceptability of the Hindi version of the CARE Measure.
Thirty out of ten participants admitted the following difficulties (in Item number 1, 4, 7, 8, & 9) while filling up the Hindi version of the questionnaire in pre-testing.
In Item number 1: Participants were found the words “Ease” & “Friendly” difficult in understanding in Hindi version of the questionnaire. Similarly, in item number 4,7,8, & 9: The Hindi translation of the word “relevant details” “Attitude” “Negative” “Positive” “Adequate Information” & “Lecturing” were found difficult by the participants.
However, all 30 participants could read the Hindi version of the CARE Measure with minimal assistance taken by the researcher. All participants reported that they understood the language (except few words) and the concepts of the 10 items within the questionnaire.
Therefore, the lead researcher had replaced those difficult words in Hindi version of the CARE measure in due consultation with the translators (T1 & T2) (Appendix III).
Phase 2: Content validity
Content Validity refers how well the content material was sampled in the measure. It can be characterized as face validity or logical validity. Face validity specifies that the measure appears to be valid, “on its face.” However, Logical validity specifies a more meticulous process, such as using a panel of experts to evaluate the content validity of a measure through qualitative and quantitative approach [17, 18].
The following three steps were helped establishing the content validity:
Establishment of the panel of experts
The total of ten experts included SCI compromised individual from the community were invited. Seven of them accepted the formal invitation in which 3 were subject experts, 2 were psychologists, 1 was social scientist and 1 was SCI compromised individual (from past 22 years). The study material as well as evaluation sheets were given to the experts for their suggestions.
Qualitative review of the items of the scale
In this section, experts were requested to provide their reviews as well as recommendations on ‘Appropriateness of the scale title, Directions for the scale, Content of the scale and Items of the scale.’ Also, experts were requested to provide the recommendations and comments (if any). Item number 4 of Hindi version CARE measure was reworded as suggested by the experts (refer Appendix III) to make the item more easy and clear.
Quantitative review of the items of the scale
In this section, experts were requested to give their valuable feedback/scoring under the following heads:
Relevance, clarity & essentiality (Not essential, useful but not essential, essential)
The responses were recorded in the excel spreadsheet and codes were given to avoid the discrepancies: Not Essential: 0 Useful but not essential: 1 Essential: 2
The content validity ratio (CVR) was calculated by using the following formula:
Similarly, content validity index (CVI) was calculated for the whole test. It is simply the mean of the CVR values of the retained items.
Phase 3: Reliability
Reliability refers to the consistency of the results in research. It is difficult to assess all tests of reliability and validity of a measure/scale in a single study which itself is a complex process. In the present study, we have tried established the internal consistency (in 50 individuals) of the Hindi-CARE Measure by using the approaches which have previously employed in the cross-cultural translation, adaptation and validation of the CARE measure in its original language (i.e. English) as well as from other different languages. This help us to ensure how well the items of the scale are consistent to each other.
Statistical considerations
The study used descriptive statistics to describe the participant’s characteristics. “Face validity and acceptability” were established by the participants to give their views and rating the importance of each item of the Hindi version of the CARE measure. Similarly, acceptability was established while performing the cognitive debriefing as well as the number of “Not Applicable” scores recorded for each of the 10 items.
Content validity of the Hindi version of the CARE Measure was done through qualitative and quantitative (CVR and CVI value) approach. Cronbach’s alpha was calculated to assess ‘Internal Reliability’ of the CARE Measure and to determine if removal of any of the 10 items weakened the reliability. All statistical calculations were performed with IBM Statistical Package for Social Sciences (SPSS) version 26.
Results
Patient characteristics
A total of 80 SCI individual participated in the study. The translation and cross-cultural adaptation process was carried out with 30 participants. The analysis of internal consistency was carried out with 50 participants.
The socio-demographic details of the participants are as follows:
We collected demographic data on sex, age, religion, level of education, marital status, place of residence, living arrangements, as well as injury characteristics (includes level of injury, date of injury, cause of injury and type of injury). Eighty individuals with SCI participated in the study. The age of the participants ranged between 18 to 67 years. The mean (±SD) age of the participating patient was 31.5(±11.1) years. Of them, 28.7% were residing in Delhi, the national capital of India and 71.2% were from other states (which includes Haryana, Bihar, West Bengal etc). The majority of the population were males (85%) and of them, 42.6% were married.
In 37.5% of the participating patients, the highest level of education was “Graduate”. Of the participants, 33.7% were employed after the injury. The injury characteristics are listed in Table 1. The socio-economic classification was carried out according to the Modified Kuppuswamy scale [(19, 20], a standard scale for the Indian population. The majority of the primary earners (67.5%) were unemployed, rest 32.5% of the participants were craft and trade related or skilled workers. There were 56.3% of the participants were fall in the “Upper Lower (IV)” socio-economic class. Only 1.3% of the participants were from “Lower (V)” socio-economic class (Fig. 1).
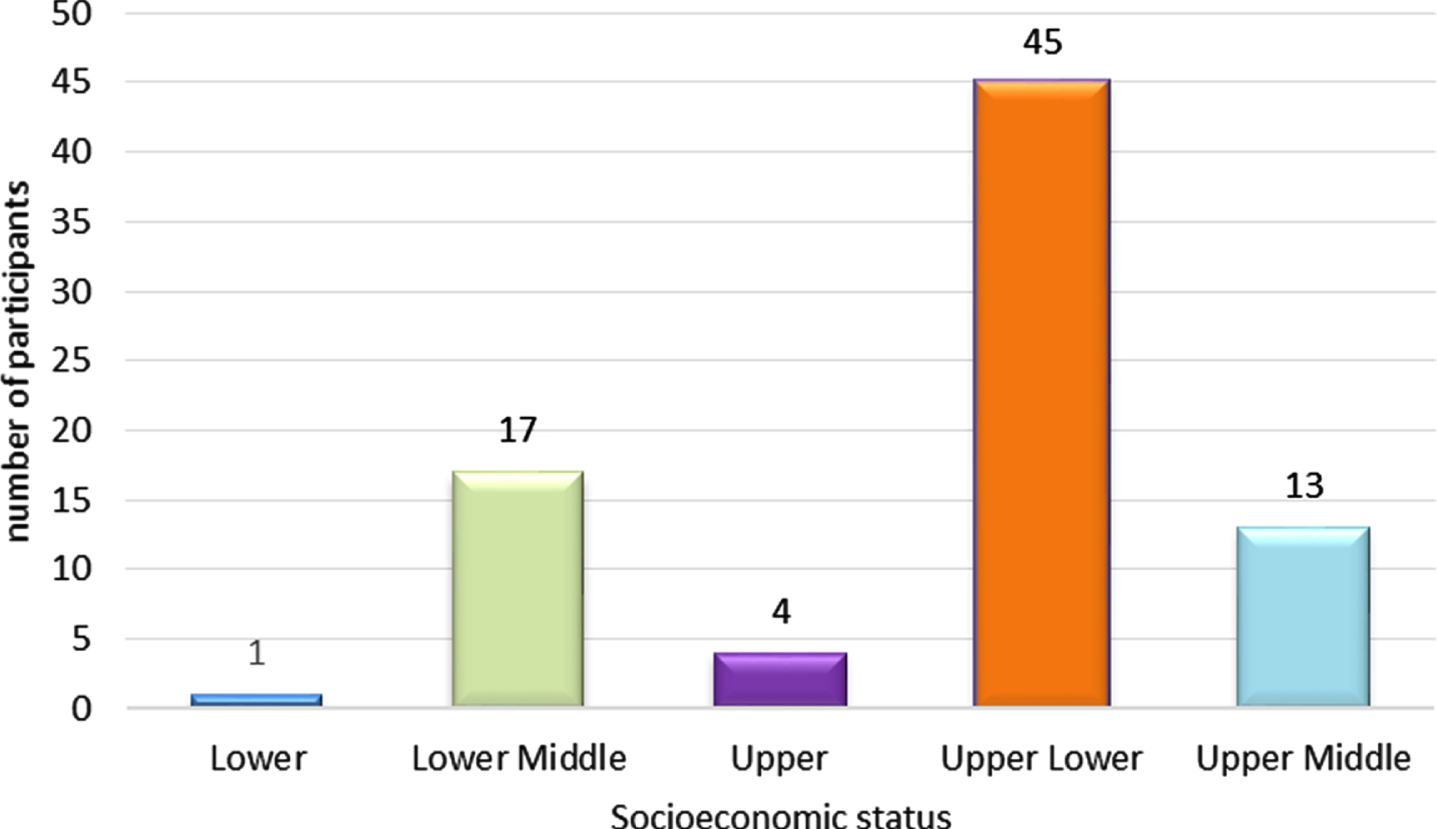
Demographic data: figure depicts the socioeconomic status (SES) of the participating population. Figure depicts the socioeconomic status (SES) of the participating population. Majority of the participants are from “Upper Lower” class.
It shows the characteristics of the sample, both for the participants in the translation and cross-cultural adaptation process (n = 30), and the participants in the process of analyzing the measurement properties (n = 50). Some information regarding the patient’s pain, secondary complications and the other questionnaires were not collected from the sample of the translation and cross-cultural adaptation phase because they were not relevant for this phase
*As per Modified Kuppuswamy Scale.
To establish the content validity of the scale, the items of CARE measure (in Hindi) having a minimum CVR value is 0.99, as the number of experts included in the panel was 7 [18]. Hence, there is no such items which have CVR less than 0.42. Therefore, no items from the Hindi version of the CARE measure has been deleted.
Item number 1,4,7,8 & 9 were revised by the expert committees to make them easy and understandable for the participants. Appendix III shows the different translations and the consensus version. These changes were made so that the target audience could comprehend the questionnaire better. In the pretest of the final version, the participants answered the questionnaire effortlessly, making it possible to produce the final version of the questionnaire. There were only 10 (20%) of participants marked their answers “Not Applicable” in item 1–10. There were no missing entries as such (refer Table 2).
Frequency for number of participants with marking “Not Applicable” & “Missing Entry” in 1–10 items
Frequency for number of participants with marking “Not Applicable” & “Missing Entry” in 1–10 items
The mean of the score for a sample (N = 50) of 10 items of the scale ranged from 3.12 to 3.88 (Table 3).
Descriptive Statistics (mean of scores and standard deviation of items for subjects, N = 50)
Descriptive Statistics (mean of scores and standard deviation of items for subjects, N = 50)
In this phase, 7 (14%) of participants marked their answers ‘Not Applicable’ in item 1–10. There were no missing entries as such (refer Table 2). Internal reliability was computed with the help of Cronbach’s alpha. For the Hindi version of CARE measure the Cronbach’s alpha is 0.924. The corrected item total correlations were found to be high in all items, with a minimum 0.601 (ranged from 0.601 to 0.833) refer Table 4.
Item-total statistics
We have translated the CARE measure into Hindi and carried out the validation and reliability (through Internal Consistency). Our findings showed high internal reliability as the computed value is 0.924. We are assuming that the participants found the scale relevant and understandable as there are no “Missing entries” and low number of “Not applicable” responses. This also helps suggesting the high face and content validity. We have not done any pilot run at this point of a time. Our results have shown a promising presentation like other published work on the translation CARE measure [13–15]. Participants found the scale very relevant and interesting as there are very few questionnaires available that focuses on empathy and patient centred approach especially in spinal cord injury population. CARE is a 10-item questionnaire, on a Likert scoring from “Poor to Excellent”. There is option to mark “Not Applicable”, if any of the item is not relevant to the consultation provided to the participants. The scale has clinical relevance in various psycho-social and chronic disabilities, as it helps to find out the patients’ perception towards their consultation with the healthcare professional. Certainly, empathy can facilitate positive outcome between patients (suffering with psycho-social problems, chronic disability/illness) and providers [12]. It is also considered to be a significant component of therapeutic relationships [19]. Dulmen SV et al, found a positive and strong correlation between patients, his/her levels of distress and clinical outcomes. It has also seen a constructive finding with regard to patient enablement [21]. The positive healthcare professional–patient relationship helps patients improving clinically such as in chronic pain, improving function, and enhancing the use of self-management skills, through multidisciplinary biopsychosocial approach which include empathy and it can assessed through questionnaires/scales commonly used in medical settings, such as the Consultation and Relational Empathy (CARE) Measure [22, 23].
Clearly, it is important to establish the translation, cultural adaptation, and validation of the CARE measure into the Hindi language, so that this can be used in the bigger sample of Hindi speaking population. The response rate was favorable, and participants from varied socioeconomic backgrounds contributed significantly to the current study. This indicates that the scale is equally understandable to individuals of various socioeconomic backgrounds. We have confidence that the scale will perform well in the larger sample size of all socioeconomic spectrum.
Conclusion
We have established a Hindi version of the CARE Measure scale and it appears to be valid and reliable enough in our chosen population. Further studies including more diverse populations and on a bigger sample size with depth psychometric analysis can be performed.
Limitations
The study was conducted with a purpose to establish the Hindi version of the Consultation and relational empathy scale. The study was performed on a lesser sample size just to ensure the reliability.
Conflict of interest
The authors declare no conflict of interest and that no funding has been availed for this manuscript.
Ethical considerations
The study got approved from Research Review committee (RRC) and Institutional Ethics Committee (IEC) of Indian Spinal Injuries Center, Vasant Kunj Delhi with reference number ISIC/RP/2021/31.
Footnotes
Appendices
| English Version of CARE Measure | Hindi Version after Pre-testing &Expert opinion |
| Item 1: |
|
| Item 4: |
|
| Item 7: |
|
| Item 8: |
|
| Item 9: |